

RSS-Feed abonnieren
DOI: 10.1055/s-0045-1807721
Quantitative Diffusion and Perfusion MRI as Response Predictor in Cervical Squamous Cell Carcinoma Treated with CCRT
Autor*innen
Funding None.


Abstract
Purpose
This article evaluates the treatment response to chemoradiotherapy in locally advanced cervical squamous cell carcinoma using quantitative diffusion and perfusion magnetic resonance imaging (MRI) parameters and studies their role as response predictors.
Materials and Methods
Patients diagnosed with locally advanced squamous cell carcinoma cervix (LASCC) and planned for concurrent chemoradiotherapy (CCRT) were included. Diffusion-weighted imaging (DWI) and perfusion MRI were performed both pre- and post-CCRT. Statistical analysis of quantitative DWI (apparent diffusion coefficient [ADC]) and perfusion MRI parameters (Ktrans, Kep, Ve, Vp, SImax, SIrel, and time-to-peak) was done to assess the tumor regression rate and compare them between the residual and nonresidual groups.
Results
All the MR perfusion parameters showed statistically significant results (p < 0.05) for the evaluation of the treatment response of LASCC to CCRT using the obtained cutoff values, except for Vp. The highest diagnostic performance was of pretreatment Kep with a sensitivity of 100%, specificity of 80%, positive predictive value of 54.5%, negative predictive value of 100%, area under the curve of 0.833, and diagnostic accuracy of 74.2%. However, ADC values did not show any significant result for the evaluation of the treatment response of LASCC.
Conclusion
Quantitative MR perfusion parameters have a significant role in evaluating treatment response to CCRT in LASCC.
Introduction
Cervical cancer is the fourth most prevalent cancer and cause of death due to cancer globally, with an estimated new case of 604,127 and 341,831 fatalities.[1] In India, it is the second most common cancer and cause of death, registering 123,907 new cases annually and 77,348 fatalities.[2]
The revised FIGO staging 2018 (International Federation of Gynecology and Obstetrics), an internationally recognized staging system for cervical cancer, has allowed the use of any imaging modality and/or pathological findings.[3] In early-stage disease, before the parametrium is involved (less than IIb), endovaginal or endorectal ultrasound (US) might suffice, but it has a limited field of view (FOV). For a more definitive evaluation of local and extrauterine cervical cancer spread, the revised FIGO staging criteria now recognize cross-sectional imaging modalities like computed tomography and magnetic resonance imaging (MRI).[4] While assessing the size and extension of the mass, it is important to assess its perfusion. Quantitative contrast-enhanced US can monitor perfusion changes but lacks consistency.[5] Dynamic contrast-enhanced MRI (DCE-MRI), on the other hand, delivers promising results when touching on tumor perfusion.
It is a fact that MRI is the preferred imaging modality due to its superior soft tissue detailing capabilities, precise identification of stromal, uterine, vaginal, parametrial, and adjoining organ invasion, and nodal involvement.[6] Diffusion-weighted MRI (DWI) and DCE-MRI add to the diagnostic precision. The changes in the tumor's biological behavior at the molecular level precede morphological changes detectable at conventional MRI.[7] Both DCE- and DWI-MRI can evaluate changes in oxygenation, perfusion, and tissue physiology with the help of quantitative and semiquantitative parameters, which serve as biomarkers of tumor characteristics.[8]
Quantitative MR perfusion is considered a promising tool, capable of reflecting perfusion by enhancement pattern, permeability, and intratumoral angiogenic activity. It is used to assess physiologic information and anatomic details of the tumor and is important to assess treatment response. Few studies have shown a positive correlation between MR perfusion parameters and tumor response in cervical cancer patients.[9] To date, there is a paucity of literature about the predictive value of quantitative MR perfusion parameters in assessing the treatment response for cervical cancer patients treated with concurrent chemoradiotherapy (CCRT). The apparent diffusion coefficient (ADC), a quantitative parameter of DWI-MRI, exhibits decreased value in cervical cancer due to hypercellularity.[10] Few authors compared pretreatment ADC values in patients with and without tumor recurrence, revealing that low pretreatment ADC values serve as a strong predictor of tumor recurrence.[11]
FIGO has defined stage IB to IIA with a tumor of more than 4 cm, and stage IIB and higher stage as locally advanced cervical cancer (LASCC). LASCC has a poor prognosis, and the 5-year survival rate is only 40% after conventional treatment.[12] [13] Ineffective CCRT can cause toxicity, so predicting the response of a tumor to CCRT would have immense value in the management of LASCC.
This study was an endeavor to supplement the existing literature regarding the potential role of DWI-MRI and DCE-MRI in the assessment of the regression of LASCC treated with CCRT and to explore their role as diagnostic and prognostic tools.
Materials and Methods
The current prospective cohort study was performed in a tertiary care hospital for 18 months, and ethical approval (IEC/VMMC/SJH/Thesis/06/2022/CC-273) was obtained. The study comprised 31 patients with biopsy-proven LASCC planned for CCRT. Informed consent was obtained from all the patients. Diffusion and perfusion MRI, both pre- and post-CCRT (1 month after completion of CCRT), were done for every patient. Quantitative parameters were derived, and statistical analysis with a comparison between residual and nonresidual tumor groups was performed. Patients who received previous treatment/changed regimens or had severe respiratory, cardiac disease, or renal disease were excluded from the study.
Image Acquisition
The patient was imaged in the supine position using a 16-channel pelvic-phased array coil on a 3-Tesla scanner (GE Discovery MR 750 W). The urinary bladder was partially filled to improve the visibility of the cervix. The scanning area included the whole pelvis and the acquisition parameters included sagittal T2W TR/TE: 9290/94.64, flip angle 160 degrees, slice thickness 5mm, interslice gap 6 mm, matrix 288 × 288 mm; axial T2W TR/TE: 10150/94.66, flip angle 160 degrees, slice thickness 5 mm, interslice gap 6 mm, matrix 312 × 312 mm; coronal T2W TR/TE: 7339/89.64, flip angle 160 degrees, slice thickness 5 mm, interslice gap 6 mm, matrix 288 × 288 mm; axial T1W TR/TE: 777/19.65, flip angle 111 degrees, slice thickness 5 mm, interslice gap 6 mm, matrix 312 × 312 mm. The focused DWI was obtained in para-axial planes, and wide FOV DWI of the pelvis in axial planes. Diffusion was acquired by applying b values of 0 and 600 for focus DWI and 0 and 800 for wide FOV DWI.
MRI perfusion was done using gadolinium-based intravenous contrast (0.2 mL/kg) at a rate of 2 mL/s, followed by 20 mL Normal Saline (NS). The images were acquired from the uterine fundus to the vulva. DCE images were obtained sequentially every 8 seconds, beginning 12 seconds (first phase) before the bolus injection. A total of 32 slices were taken with no interslice gap. Rapid acquisition (every 8 seconds was performed for 32 consecutive phases with a total time of 256 seconds). Finally, delayed axial, sagittal, and coronal T1 fat sat (T1FS) images were obtained 5 minutes after injection. A posttreatment MRI was done using the same protocol after 1 month of completion of CCRT.
MRI Analysis
The images were analyzed by a single radiologist. The visible tumor in the cervix was outlined on T2WI and dynamic T1WI. The tumor size was measured in three dimensions. ADC maps were calculated on a pixel-by-pixel basis using built-in software. The central slice with the largest part of the tumor was selected, and regions of interest (ROIs) of at least 10 mm2 were placed in the solid components on a single ADC image, with the aid of T2WI, excluding necrotic areas. The adjacent normal myometrium was used as a reference. Three readings were taken, and the mean ADC value was calculated (×10−3) mm2/sec ([Fig. 1]).

Pharmacokinetic Analysis
Ktrans maps with appropriate color coding were created from the MR perfusion study. Time-intensity curves (TICs) were generated with the brightest foci on the Ktrans map (area of maximum enhancement of the tumor). The outer one-third of the tumor was the peripheral region, and the inner two-thirds was the central region. ROI was copied to the Kep, Ve, and Vp maps, and the mean value of each perfusion parameter was generated ([Fig. 2]).

Ktrans represents the volume transfer constant from blood plasma to extravascular extracellular space (EES), Kep is the rate constant from EES to plasma, Ve is the volume of EES per unit volume of tissue, and Vp is the fraction of plasma volume. The semiquantitative parameters obtained were SImax: maximum signal intensity over the time course of the enhancement curve, SIrel: (SImax – SI0)/SI0 × 100, and TTP: time-to-peak.
Statistical Analysis
Data was coded and recorded in an MS Excel spreadsheet program using SPSS v23 (IBM Corp.) for analysis. Group comparisons for continuously distributed data were made using the independent sample t-test. If data were found to be nonnormally distributed, appropriate nonparametric tests in the form of Wilcoxon test were used. Receiver operating characteristic (ROC) analysis was performed to predict an optimal cutoff for a continuous predictor predicting a binary outcome. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and diagnostic accuracy were calculated for assessing the diagnostic performance of predictors by making a 2 × 2 cross-table with the outcome. A p-value of < 0.05 was considered statistically significant.
Results
The present study comprised 31 patients (30–83 years; mean age 55.26 years). Carcinoma cervix was most prevalent in the 60 to 69 years (29%) and a minimum number of participants (6.5%) in the 70 to 79 years. Among these, 3.2% were stage IB, 38.7% were stage II, 38.7% were stage III, and 19.4% were stage IVA. Among these 31, 25 patients (80.6%) showed nonresidual status after completion of CCRT, and 6 patients (19.4%) showed residual disease.
In the present study, the pretreatment Ktrans (central) at a cutoff of 0.926 could predict treatment response with 100% sensitivity, 76% specificity, 50% PPV, 100% NPV, and 80.6% accuracy (calculated from ROC having area under the curve [AUC] of 0.823, p = 0.016) ([Fig. 3]). Ktrans (peripheral) at a cutoff value of 0.94 (calculated from ROC having AUC of 0.787, p = 0.032) had 83.3% sensitivity, 80% specificity, 50% PPV, 95.2% NPV, and 80.6% accuracy ([Table 1]).
Abbreviations: MR, magnetic resonance; ROI, region of interest; SD, standard deviation.
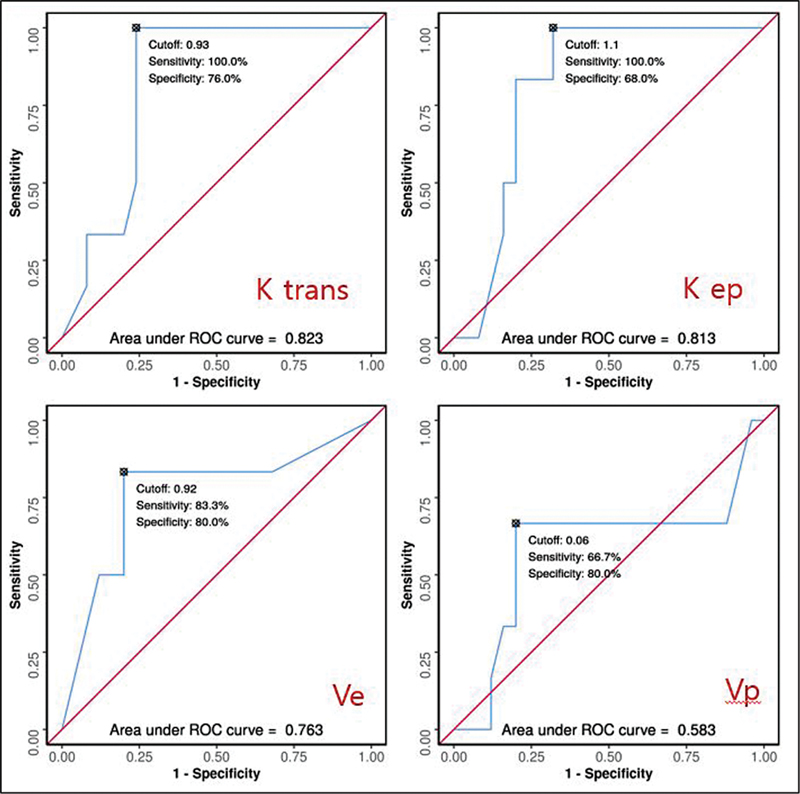
The treatment response could be predicted from pretreatment Kep (central) at a cutoff value of < 1.1 (calculated from ROC having AUC of 0.813, p = 0.020), with a sensitivity of 100%, specificity of 68%, PPV of 42.9%, NPV of 100%, and accuracy of 74.2% ([Fig. 3]). It can also be predicted from pretreatment Kep (peripheral) at a cutoff of < 1.2 (calculated from ROC having AUC of 0.833, p = 0.012), with a sensitivity of 100%, specificity of 80%, PPV of 54.5%, NPV of 100%, and accuracy of 74.2% ([Table 2]).
Abbreviations: ADC, apparent diffusion coefficient; CCRT, concurrent chemoradiotherapy; LASCC, locally advanced squamous cell carcinoma cervix; MR, magnetic resonance; NPV, negative predictive value; PPV, positive predictive value; ROC, receiver operating characteristic; TTP, time-to-peak.
The pretreatment Ve (central) at a cutoff of 0.92 (calculated from ROC having AUC of 0.763, p = 0.046) could predict treatment response with 83.3% sensitivity, 80% specificity, 50% PPV, 95.2% NPV, and 80.6% accuracy ([Table 2], [Fig. 3]). Ve (peripheral) at a cutoff of ≤ 0.986 had 100% sensitivity and 64% specificity (p-value 0.012). The cutoff and the diagnostic parameters for Vp were not reliable and not statistically significant (p = 0.150) ([Fig. 4]).

Significant differences were found in pretreatment SI max (peripheral) among the nonresidual and residual groups (p = 0.015); however, the SImax (central) was not significant (p = 0.724) ([Fig. 5]). No significant difference was found in pretreatment SIrel and TTP between the nonresidual and residual groups (p-values 0.132 and 0.391, respectively) ([Table 3]).
Abbreviations: ADC, apparent diffusion coefficient; MR, magnetic resonance; SD, standard deviation; TTP, time-to-peak.

The values of pretreatment ADC did not show a significant difference between the residual and nonresidual groups (p-value 0.080) ([Fig. 5]). At a cutoff of ADC (pretreatment) ≤ 879, it predicted the possibility of residual disease with 100% sensitivity and a specificity of 56%.
With the above results concerning the MR diffusion and perfusion parameters as response predictors in LASCC treated with CCRT, the trends observed that the best parameters in terms of sensitivity were Ktrans, Kep, Ve, SIrel, and ADC. For NPV: Ktrans, Kep, Ve, SIrel, and ADC. For diagnostic accuracy: Ktrans and Kep. For specificity and PPV: TTP ([Tables 2] and [4]). The best overall quantitative parameter was pretreatment Kep (peripheral), which at a cutoff of 1.2 had 100% sensitivity, 80% specificity, 54.5% PPV, 100% NPV, 0.833 AUC, and 74.2% accuracy, respectively, for the prediction of treatment response.
Abbreviations: ADC, apparent diffusion coefficient; CCRT, concurrent chemoradiotherapy; LASCC, locally advanced squamous cell carcinoma cervix; LR, likelihood ratio; MR, magnetic resonance; ROC, receiver operating characteristic; TTP, time-to-peak.
Discussion
Carcinoma cervix leads to significant morbidity and mortality. Therefore, accurate staging and treatment planning are crucial.[4] As of date, CCRT is the standard treatment for LASCC, and the primary challenge these patients face is resistance to treatment.[14] It is necessary to establish imaging parameters that can predict the response of carcinoma cervix to CCRT, thus significantly influencing clinical practice.[15]
However, on T2WI, recurrent or residual tumors exhibit high signal intensity and differentiating them from necrosis, inflammation, and edema poses challenges to radiologists.[16] To evaluate the treatment response effectively, the implementation of advanced biological and molecular techniques is much needed, as these changes precede the morphological changes. The vascularity of the tumor significantly influences the efficacy of CCRT, as vascular density determines the adequacy of delivery of chemotherapeutic agents and oxygen concentration within the tumor.[7]
DCE-MRI is a noninvasive method that evaluates the tissue perfusion and oxygenation within the tumor microenvironment, thus, it can be used to predict the response to therapy.[17] The quantitative analysis of DCE-MRI assesses changes in contrast concentration within tissue either as perfusion mapping or exchange of the contrast between the vascular and interstitial spaces as permeability mapping.[18]
DWI serves as a valuable tool for monitoring changes in tumor cellularity, and the ADC map facilitates quantitative evaluation of the tumor microenvironment.[19] Following CCRT, a rise in the ADC value is observed at the tumor site, suggesting a favorable response, but it cannot accurately distinguish residual tumors from fibrosis. The increase in ADC value is attributed to tumor lysis, increased extracellular space, and increased diffusion of water molecules. These molecular changes precede the macroscopic change in tumor size; thus, DWI-MRI offers a valuable opportunity for improving clinical outcomes.[20]
Of the 31 patients, 80.6% had nonresidual status and 19.4% had residual disease after completion of CCRT. In a similar study on 57 patients by Lu et al, 54.3% had complete recovery and 45.7% had residual disease. Also, DCE-MRI parameters (Ktrans, Kep, Ve) exhibited a significant difference between these two groups.[21] The discordance in the size of the two groups might be due to ours being a tertiary health care facility, a very effective CCRT regimen, and stringent follow-up.
In the present study, there was a significant difference in pretreatment Ktrans in both the central and peripheral regions between the two groups (p-value 0.016 and 0.032, respectively), exhibiting a potential predictive value in treatment response. The posttreatment Ktrans also had significant changes among the two groups (p-value < 0.001). In concordance, in a study done by Liu et al, mean pretreatment Ktrans, 3 days after starting the treatment, and change in Ktrans were higher in the nonresidual group than the residual group (p-value < 0.001, 0.025, and < 0.001, respectively) and these values served as important prognosticators.[22]
As per the statistics of our study, at a cutoff of 0.926, pretreatment Ktrans can predict the response with 100% sensitivity and 76% specificity. In a similar study by Feng et al, at a cutoff of 0.702, pretreatment Ktrans had a sensitivity of 77.3% and specificity of 81.2%.[23]
As per the literature, similar results have also been found in other cancers. In a study done by Tao et al, Ktrans was found to be a potential predictor of treatment response in lung cancer with 76.2% sensitivity, 80% specificity, and 77.8% diagnostic accuracy.[24] In another study done by Kim et al, the average value of Ktrans was significantly higher (p-value 0.001) in the complete response group of the head and neck malignancies.[25]
In the present study, there was a significant difference in pretreatment Kep in both the central and peripheral regions between the two groups (p-value 0.020 and 0.012, respectively), thus showing its potential predictive value in treatment response. Significant changes were also found in posttreatment Kep in both groups (p-value < 0.001). Lu et al also found a significant difference between mid- and pretreatment Kep and between post- and mid-treatment Kep in cervical cancer treated with CCRT (p-value < 0.001).[21]
We determined a cutoff value of pretreatment Kep as 1.1 with 100% sensitivity, 68% specificity, 42.9% PPV, 100% NPV, and 74.2% accuracy. Liu et al also exhibited a positive correlation of pretreatment Kep with the tumor regression rate in LASCC who underwent CCRT (p-value < 0.001).[22] Tao et al also found Kep to be a potential predictor of treatment response of CCRT in lung cancer with 66.7% sensitivity, 73.3% specificity, and 69.4% diagnostic accuracy.[24] Another study by Zahra et al found that higher Kep shows more tumor regression in cervical cancer (p-value 0.022).[26]
Higher Ktrans and Kep values indicate higher capillary leakage. CCRT depends on the local tissue perfusion and angiogenesis, thus tumors with higher local perfusion and higher values of pretreatment Ktrans and Kep exhibit a good response.[27]
The mean value of pretreatment Ve in the present study in the nonresidual and residual groups were 0.91 and 0.77, respectively (p-value 0.046), showing that it can be a predictive tool. However, no significant difference was found in posttreatment Ve (p-value 0.068). In the current study, at a cutoff of 0.92, pretreatment Ve had 83.3% sensitivity, 80% specificity, 50% PPV, 95.2% NPV, and 80.6% accuracy in predicting treatment response. In a study by Lu et al, a significant difference in mid-treatment Ve (p-value 0.039) was found between the complete and partial response groups.[21] Another study by Liu et al revealed that a change in Ve positively correlated with the tumor regression rate (p-value < 0.001).[22] Ve represents the EES; thus, a low value means high cellularity, and a high value means low cellularity in the tumoral tissue. Therefore, a tumor with low Ve shows a less favorable response to CCRT with more chance of residual disease and vice versa.
Presently, a significant difference was found in posttreatment Vp (peripheral) between the two groups (p-value 0.042). However, no significant difference was found in pretreatment Vp and posttreatment Vp (central) (p-value 0.545, 0.15, and 0.232, respectively). No previous study is available about the predictive role of Vp in the treatment response of cervical cancer. In most of the tumors, the value of Vp is small and not significant. It is mostly important in highly vascular tumors. The Vp at the central part of the tumor could be affected by intratumoral necrosis and heterogeneity in a large mass, thus affecting the tumor vascularity.
Significant differences were also found in pretreatment SImax (peripheral) (p-value 0.015), and at a cutoff of 1762, it had a sensitivity of 83.3%, specificity of 92%, PPV of 71.4%, NPV of 95.8%, and accuracy of 90.3%. Tumors with more angiogenesis will show an early high peak in TIC and higher SImax with good response to CCRT; however, the current findings were contradictory. After treatment, a responsive patient will have low SImax due to fibrous tissue and high value in patients with residual tumors. Tumors with more angiogenesis will show an early high peak and lower TTP. After CCRT, more fibrous tissue shows high TTP in the nonresidual group, in contrast to vascular tissue and low TTP in the residual tumor. However, the present results were not consistent. Gong et al found that the degree of enhancement in pre-RT scans has no relation with the tumor regression rate in cervical cancer; however, change in enhancement during the first 2 weeks has a significant correlation.[28]
In the present study, the increase in the ADC value in the nonresidual group was significantly higher than in the residual group. At a cutoff of 998 × 10−6, posttreatment ADC value can predict residual tumor with a sensitivity of 100%, specificity of 100%, PPV of 100%, NPV of 100%, and accuracy of 100% (p-value < 0.001). A similar result was found by Jajodia et al, who found that the ADC value provides a time window to modify the initial treatment regimen.[29] There was a significant difference between the two groups in terms of change in ADC with a p-value of 0.010. Using a cutoff of 226, a change in ADC can predict a response with 100% sensitivity, 68% specificity, 42% PPV, and 100% NPV. A similar study by de Boer et al revealed that change in ADC can predict response in cervical cancer patients.[30]
At a cutoff of 879, pretreatment ADC can predict response with 100% sensitivity, 56% specificity, 33% PPV, 100% NPV, and 64.5% accuracy (p-value 0.08). Meyer et al and Jajodia et al also concluded that pretreatment ADC values alone could not predict treatment response.[29] [31] Hypoxia, acidosis, and reduced vascularity prevail within the necrotic tumor, contributing to diminished response. In necrotic tumors with breakdown of the cellular membrane, ADC is high; however, in coagulative necrosis without membrane breakdown, ADC will be low. Therefore, pretreatment ADC is not an accurate parameter.[31]
The current standard treatment protocol for LASCC is CCRT for all the histological subtypes of the disease. Several studies have indicated that the adenocarcinoma cervix histologic subtype exhibits poorer response to CCRT and poorer overall survival compared with the squamous cell carcinoma histologic subtype.[13] To eliminate the potential impact of histological subtypes, we included only patients diagnosed with squamous cell carcinoma.
However, there were a few limitations as well. The study was single-centered, with a limited sample size. Due to the short follow-up time, the overall and progression-free survival could not be evaluated. The semiquantitative parameters were analyzed from the TIC, which are subjected to interobserver variations and are poorly reproducible as the relationship between contrast concentration and signal intensity is nonlinear. Achieving comparability across different centers necessitates the implementation of standardized software and parameters.
Conclusion
All MR perfusion quantitative parameters showed excellent predictive value in the treatment response of LASCC to CCRT, except Vp. The present study was a novel comparison between quantitative and semiquantitative MR perfusion parameters and DWI-MRI parameters and established specific cutoff values in evaluating the treatment response of LASCC to CCRT. Overall, the quantitative MR perfusion parameters performed significantly better than the semiquantitative parameters.
Conflict of Interest
None declared.
Acknowledgments
The authors wish to thank the Department of Radiodiagnosis, Vardhman Mahavir Medical College and Safdarjung Hospital staff for their support and cooperation throughout the study. All subjects were acknowledged for participation in this research.
Data Availability Statement
The cases and images are available from the Department of Radiodiagnosis, Vardhman Mahavir Medical College, and Safdarjung Hospital, New Delhi, India.
Authors' Contributions
N.B., the corresponding author, designed and revised the work, interpreted the data, and submitted the case. N.B. has approved the submitted version for publication. N.B. has drafted the work and approved the submitted version for publication. R.M. has revised the manuscript and approved the submitted version for publication. R.M. and R.N. have revised the work. S.S. provided the subjects for the study. C.A. provided the histopathology of all patients. All authors read and approved the final manuscript.
Patients' Consent
Written approval was obtained from the patients.
-
References
- 1 Sung H, Ferlay J, Siegel RL. et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71 (03) 209-249
- 2 Arbyn M, Weiderpass E, Bruni L. et al. Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis. Lancet Glob Health 2020; 8 (02) e191-e203
- 3 Bourgioti C, Chatoupis K, Moulopoulos LA. Current imaging strategies for the evaluation of uterine cervical cancer. World J Radiol 2016; 8 (04) 342-354
- 4 Zheng W, Xiong YH, Han J. et al. Contrast-enhanced ultrasonography of cervical carcinoma: perfusion pattern and relationship with tumour angiogenesis. Br J Radiol 2016; 89 (1065) 20150887
- 5 Pareja R, Rendón GJ, Vasquez M, Echeverri L, Sanz-Lomana CM, Ramirez PT. Immediate radical trachelectomy versus neoadjuvant chemotherapy followed by conservative surgery for patients with stage IB1 cervical cancer with tumors 2cm or larger: a literature review and analysis of oncological and obstetrical outcomes. Gynecol Oncol 2015; 137 (03) 574-580
- 6 Somoye G, Harry V, Semple S. et al. Early diffusion weighted magnetic resonance imaging can predict survival in women with locally advanced cancer of the cervix treated with combined chemo-radiation. Eur Radiol 2012; 22 (11) 2319-2327
- 7 Harry VN, Semple SI, Parkin DE, Gilbert FJ. Use of new imaging techniques to predict tumour response to therapy. Lancet Oncol 2010; 11 (01) 92-102
- 8 Yang W, Qiang JW, Tian HP, Chen B, Wang AJ, Zhao JG. Multi-parametric MRI in cervical cancer: early prediction of response to concurrent chemoradiotherapy in combination with clinical prognostic factors. Eur Radiol 2018; 28 (01) 437-445
- 9 Kuang F, Ren J, Zhong Q, Liyuan F, Huan Y, Chen Z. The value of apparent diffusion coefficient in the assessment of cervical cancer. Eur Radiol 2013; 23 (04) 1050-1058
- 10 Nakamura K, Joja I, Nagasaka T. et al. The mean apparent diffusion coefficient value (ADCmean) on primary cervical cancer is a predictive marker for disease recurrence. Gynecol Oncol 2012; 127 (03) 478-483
- 11 Katanyoo K, Sanguanrungsirikul S, Manusirivithaya S. Comparison of treatment outcomes between squamous cell carcinoma and adenocarcinoma in locally advanced cervical cancer. Gynecol Oncol 2012; 125 (02) 292-296
- 12 Liu Y, Bai R, Sun H, Liu H, Zhao X, Li Y. Diffusion-weighted imaging in predicting and monitoring the response of uterine cervical cancer to combined chemoradiation. Clin Radiol 2009; 64 (11) 1067-1074
- 13 He L, Wu L, Su G. et al. The efficacy of neoadjuvant chemotherapy in different histological types of cervical cancer. Gynecol Oncol 2014; 134 (02) 419-425
- 14 Padhani AR, Leach MO. Antivascular cancer treatments: functional assessments by dynamic contrast-enhanced magnetic resonance imaging. Abdom Imaging 2005; 30 (03) 324-341
- 15 Ruiz-Saurí A, García-Bustos V, Granero E. et al. Distribution of vascular patterns in different subtypes of renal cell carcinoma. A morphometric study in two distinct types of blood vessels. Pathol Oncol Res 2018; 24 (03) 515-524
- 16 Punwani S. Contrast enhanced MR imaging of female pelvic cancers: established methods and emerging applications. Eur J Radiol 2011; 78 (01) 2-11
- 17 Shukla-Dave A, Obuchowski NA, Chenevert TL. et al. Quantitative imaging biomarkers alliance (QIBA) recommendations for improved precision of DWI and DCE-MRI derived biomarkers in multicenter oncology trials. J Magn Reson Imaging 2019; 49 (07) e101-e121
- 18 Dappa E, Elger T, Hasenburg A, Düber C, Battista MJ, Hötker AM. The value of advanced MRI techniques in the assessment of cervical cancer: a review. Insights Imaging 2017; 8 (05) 471-481
- 19 Chen J, Zhang Y, Liang B, Yang Z. The utility of diffusion-weighted MR imaging in cervical cancer. Eur J Radiol 2010; 74 (03) e101-e106
- 20 Mayr NA, Wang JZ, Zhang D. et al. Longitudinal changes in tumor perfusion pattern during the radiation therapy course and its clinical impact in cervical cancer. Int J Radiat Oncol Biol Phys 2010; 77 (02) 502-508
- 21 Lu H, Wu Y, Liu X. et al. The role of dynamic contrast-enhanced magnetic resonance imaging in predicting treatment response for cervical cancer treated with concurrent chemoradiotherapy. Cancer Manag Res 2021; 13: 6065-6078
- 22 Liu B, Sun Z, Ma WL. et al. DCE-MRI quantitative parameters as predictors of treatment response in patients with locally advanced cervical squamous cell carcinoma underwent CCRT. Front Oncol 2020; 10: 585738
- 23 Feng Y, Liu H, Ding Y. et al. Combined dynamic DCE-MRI and diffusion-weighted imaging to evaluate the effect of neoadjuvant chemotherapy in cervical cancer. Tumori 2020; 106 (02) 155-164
- 24 Tao X, Wang L, Hui Z. et al. DCE-MRI perfusion and permeability parameters as predictors of tumor response to CCRT in patients with locally advanced NSCLC. Sci Rep 2016; 6: 35569
- 25 Kim S, Loevner LA, Quon H. et al. Prediction of response to chemoradiation therapy in squamous cell carcinomas of the head and neck using dynamic contrast-enhanced MR imaging. AJNR Am J Neuroradiol 2010; 31 (02) 262-268
- 26 Zahra MA, Tan LT, Priest AN. et al. Semiquantitative and quantitative dynamic contrast-enhanced magnetic resonance imaging measurements predict radiation response in cervix cancer. Int J Radiat Oncol Biol Phys 2009; 74 (03) 766-773
- 27 Zhu L, Zhu L, Shi H. et al. Evaluating early response of cervical cancer under concurrent chemo-radiotherapy by intravoxel incoherent motion MR imaging. BMC Cancer 2016; 16: 79
- 28 Gong QY, Brunt JN, Romaniuk CS. et al. Contrast enhanced dynamic MRI of cervical carcinoma during radiotherapy: early prediction of tumour regression rate. Br J Radiol 1999; 72 (864) 1177-1184
- 29 Jajodia A, Mahawar V, Chaturvedi AK. et al. Role of ADC values in assessing clinical response and identifying residual disease post-chemo radiation in uterine cervix cancer. Indian J Radiol Imaging 2019; 29 (04) 404-411
- 30 de Boer P, Mandija S, Werensteijn-Honingh AM, van den Berg CAT, de Leeuw AAC, Jürgenliemk-Schulz IM. Cervical cancer apparent diffusion coefficient values during external beam radiotherapy. Phys Imaging Radiat Oncol 2019; 9: 77-82
- 31 Meyer HJ, Wienke A, Surov A. Pre-treatment apparent diffusion coefficient does not predict therapy response to radiochemotherapy in cervical cancer: a systematic review and meta-analysis. Anticancer Res 2021; 41 (03) 1163-1170
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
04. Juni 2025
© 2025. Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Sung H, Ferlay J, Siegel RL. et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71 (03) 209-249
- 2 Arbyn M, Weiderpass E, Bruni L. et al. Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis. Lancet Glob Health 2020; 8 (02) e191-e203
- 3 Bourgioti C, Chatoupis K, Moulopoulos LA. Current imaging strategies for the evaluation of uterine cervical cancer. World J Radiol 2016; 8 (04) 342-354
- 4 Zheng W, Xiong YH, Han J. et al. Contrast-enhanced ultrasonography of cervical carcinoma: perfusion pattern and relationship with tumour angiogenesis. Br J Radiol 2016; 89 (1065) 20150887
- 5 Pareja R, Rendón GJ, Vasquez M, Echeverri L, Sanz-Lomana CM, Ramirez PT. Immediate radical trachelectomy versus neoadjuvant chemotherapy followed by conservative surgery for patients with stage IB1 cervical cancer with tumors 2cm or larger: a literature review and analysis of oncological and obstetrical outcomes. Gynecol Oncol 2015; 137 (03) 574-580
- 6 Somoye G, Harry V, Semple S. et al. Early diffusion weighted magnetic resonance imaging can predict survival in women with locally advanced cancer of the cervix treated with combined chemo-radiation. Eur Radiol 2012; 22 (11) 2319-2327
- 7 Harry VN, Semple SI, Parkin DE, Gilbert FJ. Use of new imaging techniques to predict tumour response to therapy. Lancet Oncol 2010; 11 (01) 92-102
- 8 Yang W, Qiang JW, Tian HP, Chen B, Wang AJ, Zhao JG. Multi-parametric MRI in cervical cancer: early prediction of response to concurrent chemoradiotherapy in combination with clinical prognostic factors. Eur Radiol 2018; 28 (01) 437-445
- 9 Kuang F, Ren J, Zhong Q, Liyuan F, Huan Y, Chen Z. The value of apparent diffusion coefficient in the assessment of cervical cancer. Eur Radiol 2013; 23 (04) 1050-1058
- 10 Nakamura K, Joja I, Nagasaka T. et al. The mean apparent diffusion coefficient value (ADCmean) on primary cervical cancer is a predictive marker for disease recurrence. Gynecol Oncol 2012; 127 (03) 478-483
- 11 Katanyoo K, Sanguanrungsirikul S, Manusirivithaya S. Comparison of treatment outcomes between squamous cell carcinoma and adenocarcinoma in locally advanced cervical cancer. Gynecol Oncol 2012; 125 (02) 292-296
- 12 Liu Y, Bai R, Sun H, Liu H, Zhao X, Li Y. Diffusion-weighted imaging in predicting and monitoring the response of uterine cervical cancer to combined chemoradiation. Clin Radiol 2009; 64 (11) 1067-1074
- 13 He L, Wu L, Su G. et al. The efficacy of neoadjuvant chemotherapy in different histological types of cervical cancer. Gynecol Oncol 2014; 134 (02) 419-425
- 14 Padhani AR, Leach MO. Antivascular cancer treatments: functional assessments by dynamic contrast-enhanced magnetic resonance imaging. Abdom Imaging 2005; 30 (03) 324-341
- 15 Ruiz-Saurí A, García-Bustos V, Granero E. et al. Distribution of vascular patterns in different subtypes of renal cell carcinoma. A morphometric study in two distinct types of blood vessels. Pathol Oncol Res 2018; 24 (03) 515-524
- 16 Punwani S. Contrast enhanced MR imaging of female pelvic cancers: established methods and emerging applications. Eur J Radiol 2011; 78 (01) 2-11
- 17 Shukla-Dave A, Obuchowski NA, Chenevert TL. et al. Quantitative imaging biomarkers alliance (QIBA) recommendations for improved precision of DWI and DCE-MRI derived biomarkers in multicenter oncology trials. J Magn Reson Imaging 2019; 49 (07) e101-e121
- 18 Dappa E, Elger T, Hasenburg A, Düber C, Battista MJ, Hötker AM. The value of advanced MRI techniques in the assessment of cervical cancer: a review. Insights Imaging 2017; 8 (05) 471-481
- 19 Chen J, Zhang Y, Liang B, Yang Z. The utility of diffusion-weighted MR imaging in cervical cancer. Eur J Radiol 2010; 74 (03) e101-e106
- 20 Mayr NA, Wang JZ, Zhang D. et al. Longitudinal changes in tumor perfusion pattern during the radiation therapy course and its clinical impact in cervical cancer. Int J Radiat Oncol Biol Phys 2010; 77 (02) 502-508
- 21 Lu H, Wu Y, Liu X. et al. The role of dynamic contrast-enhanced magnetic resonance imaging in predicting treatment response for cervical cancer treated with concurrent chemoradiotherapy. Cancer Manag Res 2021; 13: 6065-6078
- 22 Liu B, Sun Z, Ma WL. et al. DCE-MRI quantitative parameters as predictors of treatment response in patients with locally advanced cervical squamous cell carcinoma underwent CCRT. Front Oncol 2020; 10: 585738
- 23 Feng Y, Liu H, Ding Y. et al. Combined dynamic DCE-MRI and diffusion-weighted imaging to evaluate the effect of neoadjuvant chemotherapy in cervical cancer. Tumori 2020; 106 (02) 155-164
- 24 Tao X, Wang L, Hui Z. et al. DCE-MRI perfusion and permeability parameters as predictors of tumor response to CCRT in patients with locally advanced NSCLC. Sci Rep 2016; 6: 35569
- 25 Kim S, Loevner LA, Quon H. et al. Prediction of response to chemoradiation therapy in squamous cell carcinomas of the head and neck using dynamic contrast-enhanced MR imaging. AJNR Am J Neuroradiol 2010; 31 (02) 262-268
- 26 Zahra MA, Tan LT, Priest AN. et al. Semiquantitative and quantitative dynamic contrast-enhanced magnetic resonance imaging measurements predict radiation response in cervix cancer. Int J Radiat Oncol Biol Phys 2009; 74 (03) 766-773
- 27 Zhu L, Zhu L, Shi H. et al. Evaluating early response of cervical cancer under concurrent chemo-radiotherapy by intravoxel incoherent motion MR imaging. BMC Cancer 2016; 16: 79
- 28 Gong QY, Brunt JN, Romaniuk CS. et al. Contrast enhanced dynamic MRI of cervical carcinoma during radiotherapy: early prediction of tumour regression rate. Br J Radiol 1999; 72 (864) 1177-1184
- 29 Jajodia A, Mahawar V, Chaturvedi AK. et al. Role of ADC values in assessing clinical response and identifying residual disease post-chemo radiation in uterine cervix cancer. Indian J Radiol Imaging 2019; 29 (04) 404-411
- 30 de Boer P, Mandija S, Werensteijn-Honingh AM, van den Berg CAT, de Leeuw AAC, Jürgenliemk-Schulz IM. Cervical cancer apparent diffusion coefficient values during external beam radiotherapy. Phys Imaging Radiat Oncol 2019; 9: 77-82
- 31 Meyer HJ, Wienke A, Surov A. Pre-treatment apparent diffusion coefficient does not predict therapy response to radiochemotherapy in cervical cancer: a systematic review and meta-analysis. Anticancer Res 2021; 41 (03) 1163-1170