

Subscribe to RSS
DOI: 10.1055/s-0045-1809967
Real-World Recanalization Outcomes of Mechanical Thrombectomy in India: A Systematic Review and Meta-Analysis of Observational Studies
Authors

Abstract
This systematic review and meta-analysis aimed to study the real-world recanalization rates of mechanical thrombectomy (MT) in Indian stroke patients. A comprehensive literature search of PubMed, Scopus, and Embase was conducted for Indian observational studies on MT published up to September 30, 2024. The studies assessing recanalization using the modified thrombolysis in cerebral infarction (mTICI) met the inclusion criteria for review. Besides, only the studies that defined successful recanalization as mTICI ≥2b were included in the meta-analysis. Data on MT techniques, recanalization rates, number of passes, and first-pass effect were extracted. Risk of bias assessment was done using the MINORS tool. Meta-analysis was performed with a random-effects model. Heterogeneity was measured with I 2 statistic, and publication bias was assessed via Egger's test. Subgroup and sensitivity analyses were also conducted to address heterogeneity and test the strength of our pooled estimates. Nineteen studies were included in our review out of which 15 retrospective studies entered the primary meta-analysis. The pooled recanalization rate was 80.7% (95% CI: 74.7–86.8%; I 2 = 88.76%). We performed a sensitivity analysis after excluding two outlier studies which reduced heterogeneity (I 2 = 71.99%) significantly and increased the pooled rate to 82.1%. In the stent retriever subgroup, the pooled recanalization rate after sensitivity analysis was 80.9%. The overall pooled first-pass recanalization rate was 46.8%, and the same was 46.0% for stent retriever-only cases. Due to methodological heterogeneity and scarce data, pooled analyses for aspiration and combined techniques, posterior circulation strokes, and tandem occlusions could not be performed. MT in Indian stroke patients results in successful recanalization rates comparable to global data. We need further well-designed prospective studies for standardized outcomes, especially for contact aspiration technique, which has a potential to be the cost-effective first-line strategy for developing countries such as India.
Introduction
Stroke is a leading cause of disability and death worldwide, with ischemic stroke constituting the majority of cases. Large vessel occlusion (LVO) in acute ischemic stroke (AIS) often results in significant morbidity and mortality and is associated with poor recanalization rates with intravenous thrombolysis (IVT).[1] Early recanalization is crucial for improved outcomes in LVO ischemic strokes.[2] Over the past decade, mechanical thrombectomy (MT) has evolved as the standard of care for LVO-associated AIS. It has demonstrated significant superiority in comparison to IVT alone for achieving recanalization in LVOs.[3] The effectiveness of MT has been established in major randomized controlled trials (RCTs) such as MR CLEAN, SWIFT PRIME, REVASCAT, and ESCAPE and EXTEND-IA. These trials observed significantly improved functional outcomes with successful recanalization.[4] The Thrombolysis in Cerebral Infarction (TICI) is a standardized grading system to assess the degree of reperfusion after MT.[5] It was modified by a consensus group in 2013, thus evolving into the currently most commonly used grading system, mTICI.[6] Most studies define successful reperfusion as an mTICI grade of ≥2b, which is defined as ≥ 50% antegrade reperfusion of the previously occluded arterial territory.[7] Higher rates of successful recanalization are associated with reduced mortality and a higher probability of reduced disability with modified Rankin's scale ≤ 2 at 90 days.[8] However, MT outcomes depend on several factors such as patient selection, procedural techniques, and operators' experience.
The burden of stroke in India is on the rise, with the current prevalence rates varying from 44.54 to 150/100,000.[9] Stroke is the second major cause of death and principal cause of disability.[10] In India, stroke is a major contributor to noncommunicable disease-related deaths (41%) and disability-adjusted life-years (72%), as per the data from the Indian Council of Medical Research (ICMR). In India, the average age of stroke patients is around 55 to 60 years, which is about 10 years younger than in the Western world. The younger age of incidence amounts to a higher post-stroke disability. Despite advancements in global stroke care, India faces unique challenges in implementing MT and falls vastly short in acute stroke treatment.[11]
Several studies from India have reported variable recanalization rates with MT. The results of some are in concordance with the western cohorts while others observed lower success rates. While the global MT trials established MT as the gold standard, regional real-world outcomes can vary significantly based on healthcare infrastructure and patient selection strategies. The factors contributing to this variability could be differences in procedural techniques, operator expertise, and the use of adjunctive therapies such as intra-arterial thrombolytics or balloon angioplasty. Furthermore, patient selection based on advanced imaging like perfusion studies, stroke subtypes categorized by etiopathogenesis, and region-specific LVO occlusion topography could also be contributory. Thus, understanding the real-world recanalization rates in the Indian context is crucial to bridge the gap between clinical trials and practical outcomes. This can further help in establishing standardized stroke pathways. Furthermore, identifying regional variations in recanalization rates can help tailor policies to improve stroke treatment in underserved areas. An Indian-specific database of MT outcomes can facilitate future research into predictors of successful recanalization and optimal functional outcomes.
This systematic review and meta-analysis aim to estimate the pooled recanalization rate and to assess heterogeneity among reported outcomes following MT in Indian studies. We also aim to explore variations across different subgroups, including procedural techniques and LVO patterns.
Materials and Methods
Study Design and Search Strategy
This study was conducted according to the methodological guidelines established for systematic reviews and meta-analyses. The PRISMA 2020 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were followed for the literature search, initial screening, and studies selection process. The included studies being observational in nature, we additionally adhered to the MOOSE (Meta-analysis Of Observational Studies in Epidemiology) guidelines for the stages of data extraction, quality assessment, quantitative synthesis, and meta-analyses. The study protocol aimed to systematically assess the real-world recanalization rates following MT in India. We performed a review of the published medical literature till September 30, 2024. PubMed, Scopus, and Embase databases were explored using a structured search strategy. A thorough literature search was conducted across these databases to identify studies concerning MT outcomes in India. The search strategy composed of relevant medical subject headings terms and keywords along with appropriate filters. [Table 1] shows the detailed search strategy followed in our study.
Inclusion Criteria
This systematic review included Indian prospective and retrospective observational studies on recanalization rates of MT in stroke. While the case series were included in the descriptive review, only the ones with more than 10 patients were considered for inclusion in the meta-analysis. The studies assessing recanalization using the modified thrombolysis in cerebral infarction (mTICI) met the inclusion criteria. Besides, only the studies that defined successful recanalization as mTICI ≥2b were included in the meta-analysis for pooled recanalization rates. Details on procedural techniques were recorded where available and considered for subgroup analyses. These, however, were not mandatory for inclusion in the study and primary meta-analysis. Only articles published in peer-reviewed journals in English were considered. The case reports, review articles, editorials, and conference abstracts were excluded.
Study Selection Process
We identified 1,037 studies across PubMed, Scopus, and Embase, from which 209 duplicate records were removed. The remaining 828 articles were screened for titles and abstracts by the two independent authors (A.P. and K.S.). Subsequently, further study selection was conducted according to our defined inclusion criteria as detailed in the PRISMA flowchart ([Fig. 1]). One of the authors performed the selection process within the free version of EPPI-Reviewer web-based application, while the other used Microsoft Excel. Ultimately, 19 studies met the inclusion criteria for our systematic review.

Data Extraction
Data were independently extracted by two authors (A.P. and K.S.) using a well-structured Excel-based sheet. The recorded variables included the study characteristics (author, year of publication, study design, selection criteria, and sample size); patient demographics (mean age and gender distribution); stroke characteristics (site of LVO, time from onset to groin puncture, and recanalization); procedural details (MT technique used—SR, aspiration, or combined approach); rescue strategy (the use of an alternative thrombectomy technique after failure of the initial approach); and primary outcome (successful recanalization rate defined using the TICI grading scale, first-pass recanalization, and number of passes). When available, recanalization rates stratified by thrombectomy technique or arterial territory were also noted. Any discrepancies were resolved through discussion and mutual agreement between the two authors ([Tables 2] and [3]).
|
Study |
Year of publication |
Duration |
Study design |
Details of comparison groups |
Quantitative synthesis |
Children (< 18 yrs) |
Sample size |
Inclusion criteria |
Exclusion criteria |
Mean/Median age (y) |
Gender (male) |
|---|---|---|---|---|---|---|---|---|---|---|---|
|
Athiyappan et al[12] |
2024 |
2019–2021 |
Retrospective comparative cohort |
Tirofiban vs. non-tirofiban |
Demographics and recanalization rates |
No |
Total patients = 82; tirofiban group = 36, non-tirofiban group = 46 |
Age ≥ 18, AIS due to LVO in anterior or posterior circulation |
Not defined |
56 |
53 (64.6%) |
|
Bhatti et al[13] |
2019 |
2013–2018 |
Retrospective cohort |
NA |
Not included |
Yes |
5 |
Age < 18 y, AIS due to LVO in anterior or posterior circulation |
Not defined |
11 |
5 (100%) |
|
Bhatti et al[14] |
2021 |
2010–2020 |
Retrospective comparative cohort |
MT only vs. MT plus rescue stenting/angioplasty |
Demographics and recanalization rates |
No |
Total = 181; MT = 142; MT plus = 39 |
AC AIS with endovascular intervention |
Posterior circulation stroke, lost to follow-up |
MT = 48.9 ± 16.1; MT plus = 57 ± 12.7 |
MT = 96 (67.6%); MT plus = 32 (82.1%) |
|
Charan et al[15] |
2024 |
2016–2019 |
Retrospective case–control |
Successful recanalization vs. unsuccessful recanalization |
Demographics and recanalization rates |
No |
104 |
>18-y-old patients with LVO in ICA, M1 or M2 or basilar artery |
Not defined |
50 |
56 (53.8%) |
|
Charan et al[16] |
2024 |
2018–2021 |
Retrospective cohort |
NA |
Demographics and recanalization rates |
No |
15 |
>18-y-old patients with M2 MCA occlusion in either superior or inferior division within 6 h of onset |
Concomitant M1 occlusion and ICAD were excluded |
50 |
8 (53.3%) |
|
Charan et al[17] |
2024 |
2016–2019 |
Retrospective cohort |
NA |
Demographics and recanalization rates |
No |
52 |
18–80-y-olds were included who underwent MT with SR only; ICA terminus, M1, M2, and basilar were included |
Aspiration or combined technique |
50 |
22 (42.3%) |
|
Dalai et al[18] |
2023 |
2017–2021 |
Retrospective cohort |
NA |
Not included |
Yes |
14 |
<18-y-old AIS patients within 6 h of onset who underwent endovascular treatment |
Stroke mimics were excluded |
11.6 |
9 (64.3%) |
|
Garg et al[19] |
2024 |
2015–2022 |
Retrospective cohort |
NA |
Demographics and recanalization rates |
No |
25 |
>18-y-old patients with LVO with a large core infarct with occlusion in ICA, M1 or M2 or both MCA and ICA within 24 h. Large infarcts were determined by APSECTS 3–5 based on initial NCCT or diffusion MRI |
Those lost to follow-up or for whom 3 mo of mRS was not available |
Median age = 53 y; early = 48 (38–59), late = 59 (47.75–67) |
13 (52%) |
|
Kamepalli et al[20] |
2024 |
2018–2021 |
Retrospective comparative cohort |
1st pass vs. >1 pass recanalization |
Demographics and recanalization rates |
No |
69, 1st pass = 32, >1 pass = 37 |
LVO patients of AIS who underwent Multiphase CTA before MT |
Nonavailability of multiphase CTA, motion artifacts and incomplete DSA runs |
60 |
39 (56%) |
|
Kannath et al[21] |
2018 |
2014–2016 |
Retrospective comparative cohort |
SR DT8 vs. 3–5 (DT3-5) min |
Demographics and recanalization rates |
No |
40, DT8 = 17, DT5 = 23 |
LVO (excluding cervical ICA and posterior circulation) within 6 h of onset with ASPECTS ≥6 |
Cervical ICA occlusions and posterior circulation stroke |
56.8 ± 12.4 |
26 (65%) |
|
Kovilapu et al[22] |
2021 |
2017–2020 |
Retrospective comparative cohort |
Hyperdense vessel sign positive (HVS + ) vs. HVS- |
Demographics and recanalization rates |
No |
52, HVS+ = 28, HVS = 24 |
>18-y-old patients with LVO who underwent MT with SR or aspiration |
Those who underwent MT with combined technique were excluded. M2, vertebrobasilar and tandem lesions were excluded |
NM |
NM |
|
Kuruttukulam et al[23] |
2023 |
2019–2020 |
Retrospective comparative cohort |
Tenecteplase vs. Alteplase before MT |
Demographics and recanalization rates |
No |
75 |
LVO patients who underwent MT |
Not defined |
59.69 (±15.4) |
49 (65.3%) |
|
Parthasarathy et al[24] |
2015 |
2011–2014 |
Prospective comparative cohort study |
Tandem ICA-M1 occlusion vs. terminal ICA occlusion |
Demographics only |
No |
14 |
Acute ischemic stroke with tandem or terminal ICA occlusion within 12 h |
Not defined |
Median 56 (33–70) |
6 (42.85%) |
|
Prajapati et al[25] |
2022 |
2016–2020 |
Retrospective comparative cohort |
Direct thrombectomy vs. bridging thrombolysis |
Demographics and recanalization rates |
No |
76; 47—direct thrombectomy; 29—bridging thrombolysis |
LVO within 4.5 h, or in-hospital stroke or those thrombolysed outside and referred for MT |
Unclear time of onset, wake-up stroke, recent stroke, and new-onset worsening |
50.5 y |
51 (67.1%) |
|
Rajan et al[26] |
2022 |
2012–2019 |
Retrospective cohort |
NA |
Demographics and recanalization rates |
No |
157 |
Anterior or posterior circulation LVO within 24 h with ASPECT ≥ 4 |
Not defined |
Median 60 (IQR: 51–68) |
101 (64.3%) |
|
Ramachandran et al[27] |
2021 |
2013–2020 |
Retrospective cohort |
NA |
Demographics and recanalization rates |
No |
102 |
Anterior circulation LVO who underwent MT within 24 h onset |
Patients with images having motion artifacts and excessive calcifications |
Mean 60.5 ± 1.8 |
60 (58.8%) |
|
Shavi et al[28] |
2024 |
2018–2021 |
Prospective comparative cohort study |
CA vs. Solitaire |
Demographics only |
No |
75, Solitaire = 36, CA = 39 |
AIS both anterior and posterior circulation, more than 18 y treated within 24 h with MT |
AIS post 24 h, pre-stroke MRS >3, ICH, NIHSS <6 without aphasia |
Solitaire = 56.4 ± 15.9, CA = 55.9 ± 17.4 |
Solitaire-15 (41.7%), CA = 17 (43.6%) |
|
Singh et al[29] |
2017 |
2014–2016 |
Retrospective cohort |
NA |
Demographics and recanalization rates |
No |
137, anterior circulation = 112, posterior circulation = 25 |
LVO patients of AIS who underwent MT with Solitaire FR |
Those with a low NIHSS score or spontaneous improvement in NIHSS (defined as a drop to ≤4) |
57 ± 11.96, AC-57.85 ± 12.52, PC = 56.4 ± 9.19 |
87 (63.5%), AC-71 (63.4%), PC-16 (64%) |
|
Sreedharan et al[30] |
2022 |
2012–2019 |
Retrospective cohort |
NA |
Demographics and recanalization rates |
No |
145 |
LVO patients who underwent MT |
Not defined |
58.57 (± 13.57) |
105 (72.4%) |
Abbreviations: AC, anterior circulation; AIS, acute ischemic stroke; ASPECT, Alberta Stroke Program Early CT score; CA, contact aspiration; CTA, computed tomography angiography; DSA, digital subtraction angiography; DT, dwell time; HVS, hyperdense vessel sign; ICA, internal carotid artery; ICAD, intracranial atherosclerotic disease; ICH, intracerebral hemorrhage; IQR, interquartile range; LVO, large vessel occlusion; MEVO, medium vessel occlusion; MRI, magnetic resonance imaging; MT, mechanical thrombectomy; NA, not applicable; NCCT, non-contrast computed tomography; NIHSS, National institute of Health Stroke scale; NM, not mentioned; PC, posterior circulation; SR, stent retriever.
|
Study |
Mechanical thrombectomy device used |
Number of passes |
Successful recanalization definition |
Successful recanalization rate |
First-pass effect |
MT technique |
|---|---|---|---|---|---|---|
|
Athiyappan et al[12] |
SR, aspiration, combined approach |
Median; tirofiban = 2, non-tirofiban = 1 |
mTICI >2a (mTICI ≥2b) |
Tirofiban = 31 (86.1%), Non-tirofiban = 41 (89.1%) |
Tirofiban = 15 (41.6%), non-tirofiban = 28 (60.8%) |
Tirofiban: combined technique (28), aspiration (2), SR (1), other hybrid/unspecified techniques[a] (5) Non-tirofiban: combined technique (24), aspiration (11), SR (0), other hybrid/unspecified techniques[a] (11) |
|
Bhatti et al[13] |
SR |
Median; 2 |
Not defined |
5 (100%); 4 patients TICI3, 1 patient 2b |
2/5 (40%) |
SR |
|
Bhatti et al[14] |
SR, aspiration, combined approach |
Not mentioned |
mTICI ≥2b |
MT = 114 (80.3%); MT plus = 35 (89.7%) |
Not mentioned |
SR: MT = 77 (54.2%), MT plus = 22 (56.4%); aspiration: MT = 11 (7.7%), MT plus = 6 (15.4%); combination: MT = 43 (30.3%), MT plus = 4 (10.3%) |
|
Charan et al[15] |
SR, aspiration, combined technique |
Not mentioned |
mTICI ≥2b |
SucR = 65 (62.5%), USucR = 39 (37.5%) |
Not mentioned |
SR: SucR = 23, USucR = 29; aspiration: SucR = 16, USucR = 3; combination: SucR = 26, USucR = 7 |
|
Charan et al[16] |
SR, aspiration, combined technique |
Not mentioned |
mTICI ≥2b |
11 (73.3%) |
Not mentioned |
SR: SucR = 8, USucR = 3; aspiration: SucR = 2, USucR = 1; combined technique: SucR = 1, USucR = 0 |
|
Charan et al[17] |
SR only |
Mean passes were 1.26 in those who were successfully recanalized, not considering the proportion of failed recanalization |
mTICI ≥2b |
23 (44.24%) |
15/52 (29%) |
SR = 23 SucR, 29 USucR |
|
Dalai et al[18] |
SR, aspiration, combined technique |
Not mentioned |
mTICI ≥2b (not explicitly defined but proportion of patients having mTICI ≥2b mentioned) |
12 (85.71%) |
Not mentioned |
SR = 7 (50%), aspiration = 4 (28.57%), combined technique = 3 (21.42%) |
|
Garg et al[19] |
SR, aspiration, combined approach |
Not mentioned |
mTICI ≥2b |
23 (92%); early 11 (84.6%), late 12 (100%) |
Not mentioned |
Not mentioned separately |
|
Kamepalli et al[20] |
SR |
Mean; 1.8 |
mTICI ≥2b |
58 (84.05%), 1 pass = 31, >1 pass = 27 |
32/69 (42.37%) |
All SR |
|
Kannath et al[21] |
SR |
Mean = 1.7, DT8 = 1.2, DT5 = 2.0 |
mTICI ≥2b |
34 (85%), DT8 = 16 (94.1%), 18 (78.3%) |
24 (60%), DT8 = 14 (82.4%), DT5 = 10 (43.5%) |
All SR |
|
Kovilapu et al[22] |
SR, aspiration |
Mean/Median not mentioned, rather frequency wise first-, second-, and third-pass recanalization is mentioned in HVS+ and HVS̶− |
mTICI ≥2b |
41 (78.8%), HVS+ = 23 (82.1%), HVS − = 18 (75%) |
19 (36.5%), HVS+ = 14 (50%), 5 (20.9%) |
SR: HVS+ = 18 (64%), HVS = 9 (37.5%) |
|
Kuruttukulam et al[23] |
SR, aspiration, combined technique |
Median; 2 |
mTICI ≥2b |
65 (86.7%) |
Not mentioned |
Combined technique = 28, SR = 22, aspiration = 25 |
|
Parthasarathy et al[24] |
Solitaire, penumbra |
Median; 2 |
Not explicitly defined, but in results mTICIs ≥2b were considered as successful recanalization |
Terminal = 3 (42.8%), tandem = 5 (71.4%) |
Not mentioned |
Terminal = Solitaire (6, 85.7%), penumbra (1, 14.2%); tandem = solitaire (6, 85.7%), penumbra (1, 14.2%) |
|
Prajapati et al[25] |
SR, aspiration, combined approach |
Median; bridging = 2 (1–3), direct = 2 (1–3) |
mTICI ≥2b |
Bridging = 27 (93.1%), 45 (95.7%) |
Not mentioned |
Not mentioned separately |
|
Rajan et al[26] |
SR, aspiration, combined approach |
Not mentioned |
Patients dichotomized for TICI 2b, although good clinical outcome explicitly not defined |
TICI ≥2b in 126 (80%) |
48% |
Solitaire = 136 (83.4%), penumbra aspiration = 7 (4.3%), both = 18 (12.3%) |
|
Ramachandran et al[27] |
SR, combined approach |
mTICI ≥2b |
84 (82.4%) |
44 (43.1%) |
SR = 73, combined = 25, not mentioned = 4 |
|
|
Shavi et al[28] |
SR (Solitaire), aspiration |
Not mentioned |
mTICI ≥2c |
Solitaire = 11 (30.6%), CA = 30 (76.9%) after the end of first-line strategy with 2 passes; after the end of all procedures or switching to alternate strategy = solitaire (26, 72.2%), CA (39, 100%) |
Not mentioned |
SOLITAIRE = 36, CA = 39 |
|
Singh et al[29] |
Solitaire FR |
Mean; AC = 1.54 ± 0.78, PC = 1.6 ± 0.65 |
mTICI ≥2b |
AC = 104 (92.9%), PC = 21 (84%) |
AC = 67 (59.8%), PC = 12 (48%) |
All solitaire cases only |
|
Sreedharan et al[30] |
Not mentioned |
Not mentioned |
mTICI ≥2b |
110/145 |
Not mentioned |
Not mentioned details of the MT technique |
Abbreviations: AC, anterior circulation; CA, contact aspiration; DT, dwell time; HVS, hyperdense vessel sign; LVO, large vessel occlusion; MEVO, medium vessel occlusion; MT, mechanical thrombectomy; PC, posterior circulation; SR, stent retriever; SucR, successful recanalization; TICI, thrombolysis in cerebral infarction; USucR, unsuccessful recanalization.
a Category reported as “Combination” in Athiyappan et al; device mix not specified in the publication.
Risk of Bias Assessment
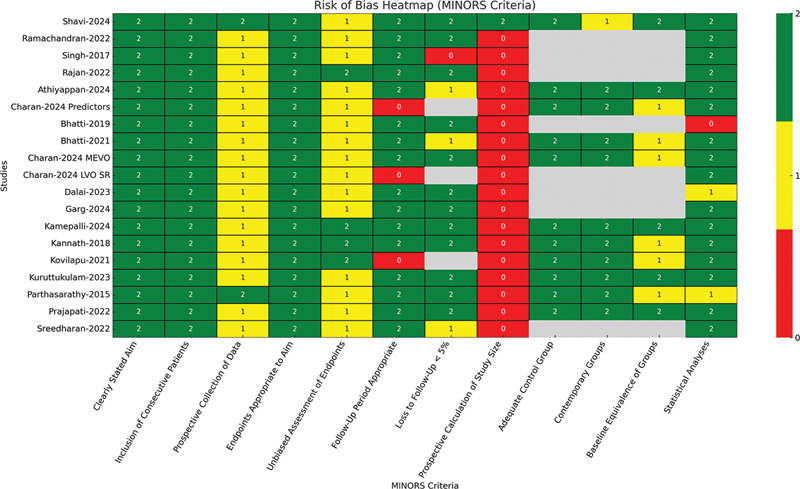
The risk of bias was assessed using the Methodological Index for Non-Randomized Studies (MINORS) criteria. This scoring system evaluates the quality of studies across multiple domains. It provides an ideal global score of 16 for noncomparative studies and 24 for comparative studies.[31] Each included study was independently scored by two authors (A.P. and K.S.), and any disagreement was resolved by mutual consensus. For noncomparative studies, scores of ≤8 were classified as poor quality, 9 to 14 as moderate quality, and 15 to 16 as good quality. For comparative studies, scores of ≤14 were considered poor, 15 to 22 moderate, and 23 to 24 good quality.[32] Most of the studies showed adequate quality in key domains, namely, clearly stated aims, inclusion of consecutive patients, and appropriate outcome assessment. However, significant limitations were noted in the following domains: prospective calculation of study size, baseline equivalence of groups, and inclusion of control groups—particularly among noncomparative studies. The risk of bias heat map ([Fig. 2]) displays these observations. Despite shortcomings, all the studies met the eligibility criteria for inclusion in the primary meta-analysis.
Statistical Analysis
Meta-analysis was performed using R open-source statistical software (version 4.3.2, R Foundation for Statistical Computing, Vienna, Austria). The pooled recanalization rate was calculated using a random-effects model due to expected heterogeneity across the studies. The weighted mean age of participants was calculated using study-level sample sizes as weights. For studies that did not report standard deviations (SDs), values were imputed based on available data from similar studies. A sensitivity analysis was conducted to test the strength of the weighted mean by excluding the studies with imputed SDs. Recanalization rates were analyzed as proportions. Meta-analysis of pooled recanalization rates was performed using a random-effects model; 95% confidence intervals were calculated for each pooled estimate; p-values <0.05 were considered significant.
Heterogeneity Assessment
I 2 statistic was used to quantify heterogeneity. I 2 >50% indicated substantial heterogeneity, for which further sensitivity and/or subgroup analysis was conducted. A leave-one-out methodology was used to perform the sensitivity analysis.
Results
The initial weighted mean age of patients across all the studies was 55.3 years, with a standard error of 1.09. SDs were missing for three studies and the values were therefore imputed.[16] [17] [25] Consequently, we conducted a sensitivity analysis by excluding these studies to test the strength of our results against potential biases from data imputation. The weighted mean age recalculated after these exclusions was 56 years, with a standard error of 1.01. The z-test for the difference in means yielded a p-value of 0.64, thus confirming that imputation had no significant impact on the overall estimate of mean age. These findings emphasize the stability of our age analysis across diverse methodological conditions. In three studies, age was reported as median instead of mean, and hence, these were not included in the summary-effect calculations. Garg et al reported a median age with interquartile range (IQR) of 53 (44–63) years, Parthasarathy et al reported a median age of 56 (range: 33–70) years and Rajan et al reported a median age with IQR of 60 (51–68) years.[19] [24] [26] Two studies focused on children aged under 18 years. Bhatti et al reported a mean age of 11 years and Dalai et al reported a mean age of 11.6 years.[13] [18]
Regarding gender, Kovilapu et al[22] did not mention about gender proportion. Aggregated data of the rest of the adult studies showed that 836 out of 1,349 total participants (61.97%) were male. Among the two studies in children, Bhatti et al[13] reported thrombectomies in five children all of who were males and Dalai et al[18] reported 64.3% males (9/14).
Recanalization Rates
Among the 19 studies reviewed, 15 retrospective studies were included in the primary meta-analysis. The remaining four studies comprised two prospective studies and two studies conducted in children. These were analyzed separately.
Using a random-effects model, the pooled recanalization rate from the 15 retrospective studies was 80.7% (95% CI: 74.7–86.8%) ([Fig. 3]). This analysis revealed a high heterogeneity across studies (I 2 = 88.76%, p < 0.001).[33] Further, sensitivity and subgroup analyses were performed to inspect the potential sources of this variability and strength of the results.

Publication Bias Assessment
Publication bias was evaluated using Egger's regression test. It showed significant funnel plot asymmetry (Z = − 2.133, p = 0.033), hence a potential publication bias influencing the pooled recanalization rates ([Fig. 4]).

Sensitivity Analyses
A sensitivity analysis was performed using the leave-one-out method to investigate sources of high heterogeneity. Each study was sequentially excluded to observe its impact on overall heterogeneity and pooled recanalization estimates. Two studies, namely, Charan et al[17] and Prajapati et al,[25] were identified as major contributors. While Prajapati et al reported a very high recanalization rate (95%), Charan et al[17] had an extremely low rate (44%). The rates of these studies significantly deviated from others. Thus, we removed these two studies from the analysis and as a result, heterogeneity decreased substantially, from the initial I 2 of 88.76 to 71.99%. The recalculated pooled recanalization rate slightly increased to 82.1% (95% CI: 77.9–86.4%) ([Fig. 3]). This indicated good recanalization across the remaining studies and stability of our pooled estimates even after addressing variability. Furthermore, publication bias post-sensitivity analysis showed no significant funnel plot asymmetry (Z = − 0.933, p = 0.351), suggesting negligible impact of publication bias postexclusion ([Fig. 4]).
Subgroup Analyses
Techniques of Thrombectomy—Stent Retrievers
A subgroup analysis was conducted for the studies that reported recanalization rates specifically associated with the use of stent retrievers (SRs). All these studies focused on LVOs, except one,[16] which included medium vessel occlusions (M2) alone. As Charan et al[16] had a recanalization rate comparable to LVO studies and had no significant contribution to heterogeneity, it was retained in the analysis.
The initial pooled recanalization rate for SR thrombectomy was 76.8% (95% CI: 63.8–89.7%; [Fig. 3]). Besides, it was associated with a high heterogeneity (I 2 = 92.54%, p < 0.001), which indicated extreme variability across the studies. The high heterogeneity could be due to differences in patient selection criteria, procedural techniques, and institutional variations in protocols. In order to address this variability, a sensitivity analysis was performed. Two studies were identified as potential outliers. Charan et al[17] reported considerably lower (44%) recanalization rates, while Singh et al[29] reported markedly higher (91%) recanalization rates. After excluding these two studies, heterogeneity was significantly reduced from I 2 = 92.54 to 74.11% (p = 0.009), while the pooled recanalization rate remained stable at 80.9% (95% CI: 71.1–90.6%; [Fig. 3]). The lack of significant publication bias postexclusion (Egger's regression test, p = 0.134) further supports the strength of these findings ([Fig. 4]). Sensitivity analysis also demonstrated that the retention of Charan et al's[16] study did not significantly alter the pooled estimates, thus justifying its inclusion in the subgroup analysis. Meta-regression was considered to examine the possible sources of heterogeneity (e.g., time to thrombectomy, site of occlusion, procedural techniques, and clot histology); however, it could not be performed meaningfully due to incomplete reporting of these variables across the studies.
Aspiration Thrombectomy or Contact Aspiration
Only a limited number of studies (n = 3) specifically reported recanalization rates for contact aspiration (CA) as a standalone technique. These studies had substantial methodological variability, which hindered a pooled analysis. In the study by Kovilapu et al, CA was used exclusively as a rescue strategy where SR thrombectomy failed, with a recanalization rate of 42.1% (8/19).[22] This lower rate likely reflects an intrinsic difficulty in clot removal after initial device failure. On the contrary, Charan et al observed CA to be a highly successful first-line strategy with a recanalization rate of 84.2% (16/19).[15] Another study reported the use of this technique in three patients with medium vessel occlusion (M2),[16] achieving recanalization in two (66.7%). These findings suggest that CA results in higher recanalization rates as a primary technique. However, it has a lower success rate when used as a rescue strategy after SR failure.
Combination Technique
A limited number of studies (n = 3) reported recanalization rates for the combined technique (a combination of SR and aspiration) separately. However, in most of these, it was used as a rescue measure after initial thrombectomy failure. Charan et al used this approach in 33 patients after initial failure, and achieved successful clot removal in 78.8% (26/33).[15] Ramachandran et al used a combined technique in 25 patients; however, it was not clearly mentioned whether they used it as a primary or rescue strategy.[27] Considering the high cost and usual practices in India, it is likely that a combined approach was used as a rescue treatment, resulting in a 64.0% (16/25) recanalization rate. Another study[16] reported its use in a single M2 patient with successful clot retrieval. Due to the small number of studies and diverse methodology (primary vs. rescue strategy), a pooled analysis was not performed. These findings suggest that this dual-modality approach may play a crucial role in achieving recanalization in cases where initial thrombectomy attempts fail.
There were only two prospective studies that provided recanalization outcomes for MT. Considering the small number, they could not be entered into a meta-analysis. Shavi et al prospectively compared CA and SR techniques in 75 patients and reported higher successful reperfusion rates (mTICI ≥ 2c/3) in the CA group (76.9 vs. 30.6%, p < 0.001).[28] In another study, Parthasarathy et al treated most of the patients with SRs (85.7%), while CA was used in 14.3% of cases.[24] However, recanalization rates were not stratified separately by thrombectomy technique.
Anterior versus Posterior Circulation
All 15 retrospective studies included in the meta-analysis predominantly comprised anterior circulation strokes. Eight studies mentioned the inclusion of posterior circulation strokes as well; however, only two studies categorically reported recanalization rates for this subgroup. Singh et al reported successful recanalization in 21 of 25 (84%) patients, whereas Charan et al in 7 of 13 (53.8%).[15] [29] The observed variation in recanalization success rates may be attributed to the differences in patient selection and thrombectomy techniques. With only two studies, a pooled meta-analysis was not conducted for this subgroup.
Among the two prospective studies, Shavi et al included patients with occlusions in both anterior (internal carotid artery [ICA], middle cerebral artery [MCA]) and posterior (vertebral, basilar, vertebrobasilar) circulations.[28] However, recanalization rates were not mentioned separately for these vascular territories. Parthasarathy et al included patients with tandem and terminal ICA occlusions only.
Tandem Lesions
Among the retrospective studies included in the meta-analysis, only one study classified recanalization rates for tandem occlusions separately.[15] In this study, tandem occlusions were treated with carotid angioplasty initially followed by intracranial SR thrombectomy. They observed a successful recanalization rate of 50% (7/14, mTICI ≥ 2b). Another eight studies mentioned the inclusion of tandem lesions but provided no separate recanalization rates for this subgroup. In view of limited data, a pooled analysis could not be conducted.
Among the two prospective studies, Parthasarathy et al evaluated recanalization outcomes in tandem and terminal ICA occlusions. They reported an overall recanalization rate of 71.4% in tandem ICA occlusions and 42.8% in terminal ICA occlusions.[24] Shavi et al did not mention the tandem lesions in their study.[28]
First-Pass Effect
A meta-analysis was conducted to study the first-pass recanalization (FPR) rates. FPR is defined as successful recanalization (mTICI ≥ 2b) in a single thrombectomy pass. The pooled FPR rate was 46.8% (95% CI: 40.0–53.6%); however, with a moderate heterogeneity (I 2 = 69.23%, p = 0.003; [Fig. 3]). Publication bias assessment using Egger's regression test did not show any significant funnel plot asymmetry (p = 0.64; [Fig. 4]).
A subgroup analysis was conducted to observe the FPR rates of SR thrombectomy alone. The pooled FPR rate was 46.0% (95% CI: 34.3–57.6%), which suggested that nearly half of the patients achieved recanalization in the first thrombectomy attempt ([Fig. 3]). These pooled effects were associated with a high heterogeneity (I 2 = 79.49%, p < 0.001). Besides, no significant funnel plot asymmetry was observed (Egger's test, p = 0.767), thus indicating the absence of a significant publication bias ([Fig. 4]).
Among the included studies, Athiyappan et al predominantly used a combined technique approach and reported a FPR of 52.4%.[12] This is apparently higher than that observed for SR alone (46.0%), which suggests that a combination approach as a primary technique is likely to offer higher first-pass success.
Among two prospective studies, Shavi et al and Parthasarathy et al did not mention the first-pass effect.[24] [28]
Stent Retriever Dwell Times
One study specifically observed the effect of SR dwell time (DT) on successful recanalization. Patients treated with an 8-minute DT (DT8 group) had significantly higher rates of FPR (mTICI ≥2b) compared to 3- and 5-minute DT (DT3–5 group) (82.4 vs. 43.5%, p = 0.013). Further, first-pass complete revascularization (TICI 3) was achieved in 52.9% of cases in the DT8 group, as compared with 8.7% in the DT3–5 group (p = 0.003).[21] The overall successful recanalization rate (TICI 2b or 3) was also higher in the DT8 group (94.1%) compared to the DT3–5 group (78.3%), although this difference could not reach statistical significance (p = 0.26). The mean number of thrombectomy attempts was lower in the DT8 group (1.2 vs. 2.0, p = 0.016). This probably suggests that longer stent deployment may result in better clot integration and retrieval efficiency.
Hyperdense Vessel Sign
One study specifically observed the influence of hyperdense vessel sign (HVS) on NCCT in predicting recanalization success with thrombectomy.[22] Among the 52 patients included, 28 were classified as HVS-positive (HVS + ), and 24 as HVS-negative (HVS–). The HVS+ group had significantly higher FPR as compared to HVS− (50.0 vs. 20.9%, p = 0.029). This suggests that a positive HVS is likely to result in a better clot retrieval efficiency.
Early recanalization (≤2 thrombectomy passes) was observed in 64.2% of HVS+ cases compared to 37.5% in HVS– cases, which nearly approached statistical significance (p = 0.054). Overall successful recanalization (TICI ≥ 2b/3) was slightly higher in the HVS+ group (82.1%) compared to the HVS– group (75.0%), but the difference was not statistically significant (p = 0.530).
The need for rescue therapy (defined as switching to CA after three failed SR attempts) was higher in the HVS– group (50.0 vs. 25.0%, p = 0.062). This indicates that HVS– patients are more likely to require additional interventions for successful recanalization.
Mechanical Thrombectomy in Children
Bhatti et al treated five children (aged 6–17 years) with SR thrombectomy. These included two basilar arteries, two MCAs, and one ICA. Complete recanalization (mTICI ≥ 2b/3) was attained in all cases, with no periprocedural complications.[13]
Dalai et al reported on 14 children (aged 6–17 years) who underwent thrombectomy with SRs, aspiration, or a combined technique.[18] The most common arteries involved were the ICA and MCA. Successful recanalization (mTICI ≥ 2b/3) was observed in 85.7% of cases (12/14). Among the remaining two patients, one had a TICI 2a recanalization and the other had recurrent occlusion despite initial recanalization. No major procedural complications were reported.
Discussion
This systematic review and meta-analysis validates the efficacy of MT in achieving good recanalization rates in Indian LVO stroke patients. The pooled effect of successful recanalization rates (mTICI ≥ 2b) was maintained in around 80% despite addressing the heterogeneity across the studies. These findings are in agreement with the international trials, namely, MR CLEAN, EXTEND-IA, SWIFT PRIME, and REVASCAT.[29] These trials reported recanalization rates ranging between 58 and 88% for SR thrombectomy.[29] It is noteworthy to see the results similar to the Western world, despite significant infrastructural constraints and ethnic variability. Recanalization rates similar to the Western world are also somewhat unexpected, considering the higher prevalence of intracranial atherosclerotic disease in the Asian population, which adds to procedural complexity and lowers the chances of recanalization.[34] Thus, it is indeed a possibility that with growing experience, better devices, and optimized protocols, higher rates of revascularization are achievable even with complex vascular pathology. Our systematic review of retrospective and prospective studies, in the absence of RCTs in India, allowed us to observe a real-world picture regarding the outcomes of MT. This data synthesis could serve as a valuable tool for developing evidence-based guidelines tailored to the Indian population, with a probable extrapolation to other Asian countries.
Subgroup analyses based on thrombectomy techniques provided valuable insights into the outcomes associated with the different techniques. In the SR-only subgroup, the pooled FPR rate was 46.0% (95% CI: 34.3–57.6%), indicating that just about half of the patients achieved successful recanalization on the first attempt. However, substantial heterogeneity (I 2 = 79.49%) across the studies calls for uniformly designed multicentric prospective studies in the near future so as to achieve more accurate estimates of the clinical efficacy of the SRs. Although only a few studies stratified their outcomes separately for aspiration thrombectomy, the limited available data provide a glimpse of evidence that suggests that CA possibly results in higher recanalization rates as compared to SRs. This trend was well demonstrated by the two studies included in our review. Charan et al observed successful recanalization in 84.2% of cases with CA.[15] Furthermore, Shavi et al directly compared CA with SRs in a well-designed prospective study and observed the former to have significantly higher reperfusion rates (76.9 vs. 30.6%, p < 0.001).[28] These observations emphasize the potential of CA as an effective first-line treatment option. Despite the growing role of CA in endovascular stroke therapy worldwide, the evidence base for the same as a standalone strategy remains scarce within the Indian context. There is a dire need for more high-quality observational studies in India focused on evaluating recanalization rates and outcomes with CA as a first-line strategy. If the efficacy of CA as a first-line strategy gets established, it holds the promise to be the primary modality of treatment in developing countries like India. This is due to the considerably lower cost of thrombectomy with CA in comparison to the SR technique.[35] The combined technique, which combines SR with aspiration, was primarily used as a rescue strategy in Indian studies rather than a first-line technique. This is likely driven by economic constraints, as the combination approach is costlier. We need well-designed prospective studies to evaluate the outcomes of a combined approach as a first-line strategy.
MT in the posterior circulation remains understudied in the Indian population. Only eight studies in our review included posterior circulation stroke, and only two provided separate recanalization rates for them. This highlights the pressing need for focused research in basilar artery occlusions. Likewise, tandem ICA occlusions require further well-powered research, as only one study in our review centered its outcomes on this subset of patients.[24]
We must acknowledge several limitations in this systematic review. One of the studies in our systematic review[30] mentioned recanalization rates but provided no details of procedural techniques and other crucial procedural data, such as the number of passes, the first-pass effect. So, this study was included in the primary meta-analysis for pooled recanalization rate calculation but could not be a part of the detailed subgroup analysis. Further, the predominance of retrospective studies in our review increases the chances of selection and reporting bias. We observed a marked heterogeneity across the studies, probably due to the differences in thrombectomy techniques, device selection, and operators' experience. This needs to be mitigated by well-designed, prospective studies in the future. Furthermore, while some studies reported FPR rates, others did not, making it difficult to assess the procedural efficiency, which actually translates into a better patient outcome. Standardized reporting of FPR should become the norm, as it is being increasingly recognized as a crucial outcome parameter. Effects of drugs such as tirofiban and thrombolytic agents on recanalization could not be studied, although these may have an influence on recanalization. Finally, the lack of sufficient data for meta-regression in our studies emphasizes the need for improved reporting of thrombectomy outcomes in future research to allow for a deeper stratified analysis.
With recanalization rates approaching 80%, our systematic review reinforced the role of MT as the gold-standard therapy for LVO ischemic strokes. However, access to MT remains highly restricted in India. Based on available data, over 270,000 patients annually in India may be eligible for MT; yet, only around “1,000 to 2,000” procedures are currently performed nationwide, based on a rough estimate.[11] Thus, the treatment gap remains enormous. To address this, we recommend the following suggestions for national health policy: (1) structured referral pathways to enable prompt transfer of eligible stroke patients from primary health centers and district hospitals to MT-capable centers; (2) expansion of comprehensive stroke centers with easy and fast access to the population in underserved and rural areas; (3) inclusion of stroke thrombectomy under the Ayushman Bharat—Pradhan Mantri Jan Arogya Yojana (AB PM-JAY) and other national insurance schemes with uniformity across all states, which will potentially ensure equitable access to stroke treatment for all eligible patients; (4) promote public awareness campaigns for early recognition of stroke symptoms, particularly in rural areas, and the importance of timely arrival at the stroke centers.
Conclusion
In this study, we observed the rates of MT in India comparable to the results of major RCTs. Preliminary data suggest that the CA technique, due to its cost-effectiveness, has the potential to be a first-line treatment strategy for resource-limited settings like India. However, this observation is based on a very small number of studies (n = 3) with significant heterogeneity. While the findings are encouraging, they should be interpreted with caution and confirmed through larger, multicentric prospective studies. Further well-designed research is needed to evaluate the effectiveness of CA as a primary modality for achieving successful FPR.
Conflict of Interest
None declared.
Authors' Contributions
A.P. contributed to the concept and design, analysis and interpretation of data, data collection, drafting the article, critical revision, final approval of the article, statistical analysis, and holds overall responsibility. K.S. contributed to the concept and design, analysis and interpretation of data, data collection, drafting the article, critical revision, and final approval of the article. U.R. contributed to the critical revision and final approval of the article. R.G. contributed to the critical revision of the article. G.V.K. contributed to the final approval of the article.
Ethical Approval
The manuscript is a systematic review and meta-analysis of the existing studies; therefore, ethics approval was not obtained.
-
References
- 1 Al Khathaami AM, Aldriweesh MA, Al Bdah BA. et al. Anterior circulation large vessel occlusion stroke in Saudi Arabia: prevalence, predictors, and outcome. J Stroke Cerebrovasc Dis 2020; 29 (09) 105080
- 2 Ospel JM, Singh N, Almekhlafi MA. et al. Early recanalization with alteplase in stroke because of large vessel occlusion in the ESCAPE trial. Stroke 2021; 52 (01) 304-307
- 3 Chandra PS, Doddamani R. Endovascular thrombectomy in acute ischemic stroke due to large vessel occlusion: current concepts and controversies. Neurol India 2023; 71 (02) 204-206
- 4 Parvathy G, Dey RC, Kutikuppala LVS. et al. Mechanical thrombectomy for AIS from large vessel occlusion - current trends and future perspectives. Ann Med Surg (Lond) 2023; 85 (12) 6021-6028
- 5 Tung EL, McTaggart RA, Baird GL. et al. Rethinking thrombolysis in cerebral infarction 2b: Which thrombolysis in cerebral infarction scales best define near complete recanalization in the modern thrombectomy era?. Stroke 2017; 48 (09) 2488-2493
- 6 Behme D, Tsogkas I, Colla R. et al. Validation of the extended thrombolysis in cerebral infarction score in a real world cohort. PLoS One 2019; 14 (01) e0210334
- 7 Jang KM, Nam TK, Ko MJ. et al. Thrombolysis in cerebral infarction Grade 2C or 3 represents a better outcome than 2B for endovascular thrombectomy in acute ischemic stroke: a network meta-analysis. World Neurosurg 2020; 136: e419-e439
- 8 Shafie M, Yu W. Recanalization therapy for acute ischemic stroke with large vessel occlusion: Where we are and what comes next?. Transl Stroke Res 2021; 12 (03) 369-381
- 9 Khurana S, Gourie-Devi M, Sharma S, Kushwaha S. Burden of stroke in India during 1960 to 2018: a systematic review and meta-analysis of community based surveys. Neurol India 2021; 69 (03) 547-559
- 10 Thayabaranathan T, Kim J, Cadilhac DA. et al. Global stroke statistics 2022. Int J Stroke 2022; 17 (09) 946-956
- 11 Sundar K, Panwar A, Yagaval DR, Huded V, Sylaja PN. Mission thrombectomy 2020 (MT2020)—India's biggest healthcare challenge yet. J Stroke Med 2020; 3 (02) 62-71
- 12 Athiyappan KM, Cherian M, Mehta P, Poyyamoli S, Reddy NH, Jayaraj A. et al. Safety profile of intra-arterial tirofiban as a rescue therapy during mechanical thrombectomy in acute ischemic stroke. Journal of Clinical Interventional Radiology ISVIR. 2024; 8 (01) 11-21
- 13 Bhatti A, Huded V, Vyas D. et al. Mechanical thrombectomy using retrievable stents in pediatric acute ischemic stroke. Indian Pediatr 2019; 56 (07) 571-575
- 14 Bhatti AA, Mahajan NP, Vyas DD, Shah MM, Huded V. Rescue strategies in anterior circulation stroke with failed mechanical thrombectomy—a retrospective observational study (RAFT). Ann Indian Acad Neurol 2021; 24 (06) 885-890
- 15 Charan BD, Gaikwad SB, Jain S. et al. Insights into angiographic recanalization of large arterial occlusion: institutional experience with mechanical thrombectomy for acute ischemic stroke. Asian J Neurosurg 2024; 19 (03) 462-471
- 16 Charan BD, Gaikwad SB, Jain S. et al. Mechanical thrombectomy in medium vessels occlusion (MeVOs): an institutional experience with M2 divisions of middle cerebral artery. Acta Med Litu 2024; 31 (01) 140-148
- 17 Charan BD, Gaikwad SB, Jain S. et al. An institutional perspective on the number of stent retriever pass and rate of recanalization in mechanical thrombectomy for acute ischemic stroke: When to stop?. Acta Med Litu 2024; 31 (01) 75-80
- 18 Dalai S, Limaye U, Kolli S, Maturu MVS, Narayana RV, Pati R. et al. Endovascular treatment of acute ischemic stroke in patients younger than 18 years. Journal of Clinical Interventional Radiology ISVIR. 2023; 7 (02) 75-80
- 19 Garg S, Ramachandran D, Mishra T. et al. Endovascular therapy in large core ischemic strokes: real-world Indian experience. Ann Indian Acad Neurol 2024; 27 (03) 244-249
- 20 Kamepalli HK, Kannath SK, Sylaja PN, Rajan JE, Chandrasekharan K. Thrombus attenuation gradient can predict successful first-pass recanalization following stentriever thrombectomy. World Neurosurg 2024; 181: e780-e788
- 21 Kannath SK, Rajan JE, Sylaja PN. et al. Dwell time of stentriever influences complete revascularization and first-pass TICI 3 revascularization in acute large vessel occlusive stroke. World Neurosurg 2018; 110: 169-173
- 22 Kovilapu UB, Jain N, Mishra A, Malik V. Selecting the appropriate first-line strategy based on hyperdense vessel sign in acute ischemic stroke increases first pass recanalization: a tertiary center experience. Indian J Radiol Imaging 2022; 31 (04) 830-836
- 23 Kuruttukulam G, Sundar K, Bhirud L, Panwar A, Alapatt PJ. Does tenecteplase before mechanical thrombectomy result in a faster revascularization as compared to alteplase? Observations from a comprehensive stroke care center in Southern India. Journal of Stroke Medicine. 2023; 6 (01) 40-5
- 24 Parthasarathy R, Goel G, Gupta V. et al. Acute ischemic stroke with tandem/terminal ICA occlusion - CT perfusion based case selection for mechanical recanalization. Neurol India 2015; 63 (03) 369-377
- 25 Prajapati C, Huded V, Mahajan N, Kulkarni A, Manual D. Comparing bridging thrombolysis with direct thrombectomy in stroke due to large vessel occlusion-Indian Experience (LVO-Direct). Ann Indian Acad Neurol 2022; 25 (05) 869-874
- 26 Rajan JE, Kannath SK, Sabarish S. et al. Mechanical thrombectomy in acute ischemic stroke: Angiographic predictors of outcome. Neurol India 2022; 70 (04) 1407-1411
- 27 Ramachandran H, Girdhar S, Sreedharan SE. et al. Does thrombus imaging characteristics predict the degree of recanalisation after endovascular thrombectomy in acute ischaemic stroke?. J Stroke Cerebrovasc Dis 2022; 31 (09) 106621
- 28 Shavi T, Pandey P, Acharya UV. A study of efficacy and outcomes of two techniques of mechanical thrombectomy in acute ischemic stroke. Indian Journal of Neurosurgery. 2024
- 29 Singh RK, Chafale VA, Lalla RS. et al. Acute ischemic stroke treatment using mechanical thrombectomy: a study of 137 patients. Ann Indian Acad Neurol 2017; 20 (03) 211-216
- 30 Sreedharan SE, Arun K, Kannath S, Jayadevan ER, Thulaseedharan JV, Sylaja PN. The impact of time to reperfusion on recanalization rates and outcome after mechanical thrombectomy: a single center experience. Ann Indian Acad Neurol 2022; 25 (02) 256-260
- 31 Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg 2003; 73 (09) 712-716
- 32 Schreve MA, Vos CG, Vahl AC. et al. Venous arterialisation for salvage of critically ischaemic limbs: a systematic review and meta-analysis. Eur J Vasc Endovasc Surg 2017; 53 (03) 387-402
- 33 Gandhi A, Shamim M, Padhi B. Steps in undertaking meta-analysis and addressing heterogeneity in meta-analysis. Evid. 2023; 1 (01) 44-59
- 34 Kim JS, Bonovich D. Research on intracranial atherosclerosis from the East and west: why are the results different?. J Stroke 2014; 16 (03) 105-113
- 35 Yang W, Lee RP, Hung AL. et al. Cost-effectiveness of a direct-aspiration first-pass technique versus stent retriever in mechanical thrombectomy. World Neurosurg 2024; 183: e495-e501
Address for correspondence
Publication History
Article published online:
02 July 2025
© 2025. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Al Khathaami AM, Aldriweesh MA, Al Bdah BA. et al. Anterior circulation large vessel occlusion stroke in Saudi Arabia: prevalence, predictors, and outcome. J Stroke Cerebrovasc Dis 2020; 29 (09) 105080
- 2 Ospel JM, Singh N, Almekhlafi MA. et al. Early recanalization with alteplase in stroke because of large vessel occlusion in the ESCAPE trial. Stroke 2021; 52 (01) 304-307
- 3 Chandra PS, Doddamani R. Endovascular thrombectomy in acute ischemic stroke due to large vessel occlusion: current concepts and controversies. Neurol India 2023; 71 (02) 204-206
- 4 Parvathy G, Dey RC, Kutikuppala LVS. et al. Mechanical thrombectomy for AIS from large vessel occlusion - current trends and future perspectives. Ann Med Surg (Lond) 2023; 85 (12) 6021-6028
- 5 Tung EL, McTaggart RA, Baird GL. et al. Rethinking thrombolysis in cerebral infarction 2b: Which thrombolysis in cerebral infarction scales best define near complete recanalization in the modern thrombectomy era?. Stroke 2017; 48 (09) 2488-2493
- 6 Behme D, Tsogkas I, Colla R. et al. Validation of the extended thrombolysis in cerebral infarction score in a real world cohort. PLoS One 2019; 14 (01) e0210334
- 7 Jang KM, Nam TK, Ko MJ. et al. Thrombolysis in cerebral infarction Grade 2C or 3 represents a better outcome than 2B for endovascular thrombectomy in acute ischemic stroke: a network meta-analysis. World Neurosurg 2020; 136: e419-e439
- 8 Shafie M, Yu W. Recanalization therapy for acute ischemic stroke with large vessel occlusion: Where we are and what comes next?. Transl Stroke Res 2021; 12 (03) 369-381
- 9 Khurana S, Gourie-Devi M, Sharma S, Kushwaha S. Burden of stroke in India during 1960 to 2018: a systematic review and meta-analysis of community based surveys. Neurol India 2021; 69 (03) 547-559
- 10 Thayabaranathan T, Kim J, Cadilhac DA. et al. Global stroke statistics 2022. Int J Stroke 2022; 17 (09) 946-956
- 11 Sundar K, Panwar A, Yagaval DR, Huded V, Sylaja PN. Mission thrombectomy 2020 (MT2020)—India's biggest healthcare challenge yet. J Stroke Med 2020; 3 (02) 62-71
- 12 Athiyappan KM, Cherian M, Mehta P, Poyyamoli S, Reddy NH, Jayaraj A. et al. Safety profile of intra-arterial tirofiban as a rescue therapy during mechanical thrombectomy in acute ischemic stroke. Journal of Clinical Interventional Radiology ISVIR. 2024; 8 (01) 11-21
- 13 Bhatti A, Huded V, Vyas D. et al. Mechanical thrombectomy using retrievable stents in pediatric acute ischemic stroke. Indian Pediatr 2019; 56 (07) 571-575
- 14 Bhatti AA, Mahajan NP, Vyas DD, Shah MM, Huded V. Rescue strategies in anterior circulation stroke with failed mechanical thrombectomy—a retrospective observational study (RAFT). Ann Indian Acad Neurol 2021; 24 (06) 885-890
- 15 Charan BD, Gaikwad SB, Jain S. et al. Insights into angiographic recanalization of large arterial occlusion: institutional experience with mechanical thrombectomy for acute ischemic stroke. Asian J Neurosurg 2024; 19 (03) 462-471
- 16 Charan BD, Gaikwad SB, Jain S. et al. Mechanical thrombectomy in medium vessels occlusion (MeVOs): an institutional experience with M2 divisions of middle cerebral artery. Acta Med Litu 2024; 31 (01) 140-148
- 17 Charan BD, Gaikwad SB, Jain S. et al. An institutional perspective on the number of stent retriever pass and rate of recanalization in mechanical thrombectomy for acute ischemic stroke: When to stop?. Acta Med Litu 2024; 31 (01) 75-80
- 18 Dalai S, Limaye U, Kolli S, Maturu MVS, Narayana RV, Pati R. et al. Endovascular treatment of acute ischemic stroke in patients younger than 18 years. Journal of Clinical Interventional Radiology ISVIR. 2023; 7 (02) 75-80
- 19 Garg S, Ramachandran D, Mishra T. et al. Endovascular therapy in large core ischemic strokes: real-world Indian experience. Ann Indian Acad Neurol 2024; 27 (03) 244-249
- 20 Kamepalli HK, Kannath SK, Sylaja PN, Rajan JE, Chandrasekharan K. Thrombus attenuation gradient can predict successful first-pass recanalization following stentriever thrombectomy. World Neurosurg 2024; 181: e780-e788
- 21 Kannath SK, Rajan JE, Sylaja PN. et al. Dwell time of stentriever influences complete revascularization and first-pass TICI 3 revascularization in acute large vessel occlusive stroke. World Neurosurg 2018; 110: 169-173
- 22 Kovilapu UB, Jain N, Mishra A, Malik V. Selecting the appropriate first-line strategy based on hyperdense vessel sign in acute ischemic stroke increases first pass recanalization: a tertiary center experience. Indian J Radiol Imaging 2022; 31 (04) 830-836
- 23 Kuruttukulam G, Sundar K, Bhirud L, Panwar A, Alapatt PJ. Does tenecteplase before mechanical thrombectomy result in a faster revascularization as compared to alteplase? Observations from a comprehensive stroke care center in Southern India. Journal of Stroke Medicine. 2023; 6 (01) 40-5
- 24 Parthasarathy R, Goel G, Gupta V. et al. Acute ischemic stroke with tandem/terminal ICA occlusion - CT perfusion based case selection for mechanical recanalization. Neurol India 2015; 63 (03) 369-377
- 25 Prajapati C, Huded V, Mahajan N, Kulkarni A, Manual D. Comparing bridging thrombolysis with direct thrombectomy in stroke due to large vessel occlusion-Indian Experience (LVO-Direct). Ann Indian Acad Neurol 2022; 25 (05) 869-874
- 26 Rajan JE, Kannath SK, Sabarish S. et al. Mechanical thrombectomy in acute ischemic stroke: Angiographic predictors of outcome. Neurol India 2022; 70 (04) 1407-1411
- 27 Ramachandran H, Girdhar S, Sreedharan SE. et al. Does thrombus imaging characteristics predict the degree of recanalisation after endovascular thrombectomy in acute ischaemic stroke?. J Stroke Cerebrovasc Dis 2022; 31 (09) 106621
- 28 Shavi T, Pandey P, Acharya UV. A study of efficacy and outcomes of two techniques of mechanical thrombectomy in acute ischemic stroke. Indian Journal of Neurosurgery. 2024
- 29 Singh RK, Chafale VA, Lalla RS. et al. Acute ischemic stroke treatment using mechanical thrombectomy: a study of 137 patients. Ann Indian Acad Neurol 2017; 20 (03) 211-216
- 30 Sreedharan SE, Arun K, Kannath S, Jayadevan ER, Thulaseedharan JV, Sylaja PN. The impact of time to reperfusion on recanalization rates and outcome after mechanical thrombectomy: a single center experience. Ann Indian Acad Neurol 2022; 25 (02) 256-260
- 31 Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg 2003; 73 (09) 712-716
- 32 Schreve MA, Vos CG, Vahl AC. et al. Venous arterialisation for salvage of critically ischaemic limbs: a systematic review and meta-analysis. Eur J Vasc Endovasc Surg 2017; 53 (03) 387-402
- 33 Gandhi A, Shamim M, Padhi B. Steps in undertaking meta-analysis and addressing heterogeneity in meta-analysis. Evid. 2023; 1 (01) 44-59
- 34 Kim JS, Bonovich D. Research on intracranial atherosclerosis from the East and west: why are the results different?. J Stroke 2014; 16 (03) 105-113
- 35 Yang W, Lee RP, Hung AL. et al. Cost-effectiveness of a direct-aspiration first-pass technique versus stent retriever in mechanical thrombectomy. World Neurosurg 2024; 183: e495-e501