
RSS-Feed abonnieren
DOI: 10.1055/s-0045-1809984
The Contribution of Regenerative Endodontics in the Management and Healing of Pathological Root Resorptions: A Systematic Review
Funding None.

- Abstract
- Introduction
- Methods
- Discussion
- Conclusion
- References
Abstract
Pathological root resorption is an irreversible condition that can compromise the tooth's prognosis. Despite the success of conventional root canal treatment, these methods have their limitations and cannot restore damaged dental tissue. Recently, regenerative techniques have been employed to treat pathological root resorption.
The aim of this systematic review is to evaluate the role of regenerative endodontics in managing pathological internal and external root resorptions in permanent teeth.
A literature search was conducted on the following databases: MEDLINE via PubMed, Web of Science, Cochrane, and Scopus, using the following Medical Subject Headings (MeSH) « root resorption », « regenerative endodontics », and keywords « tooth resorption » and « Platelet-Rich Fibrin ». A reading grid was established to extract data related to the research question. The methodological quality of each included study was assessed using Cochrane RoB and Newcastle–Ottawa scale. The review protocol was registered with PROSPERO (identification N° CRD420251023900).
After applying inclusion and exclusion criteria, nine articles were included in our review. These studies examined clinical data related to the type and location of root resorption, as well as data related to the regenerative endodontic technique employed, and the type of repair. The risk of bias was low in one study and moderate in eight studies.
The selected studies highlighted the effectiveness of regenerative endodontic techniques based on platelet-rich fibrin and revascularization in the treatment of internal and external resorptions, demonstrating their ability to repair resorption defects through the formation of newly calcified tissue.
Introduction
Pathological root resorption involves the loss of dentin, cementum, or bone triggered by inflammatory stimulation, activating osteoclasts or odontoclasts.[1] [2] This condition is permanent, irreversible, and, if untreated, progressively threatens the tooth's prognosis.
While conventional treatments, based on root canal shaping and cleaning, fail to restore vital tissue,[3] regenerative endodontic techniques have recently emerged as promising alternatives. The aim is to replace damaged pulp and tooth structures with vital tissue. However, the optimal therapeutic approach remains a subject of debate.[4] [5]
This systematic review examines the effectiveness of regenerative endodontic procedures (REPs) in managing pathological root resorption.
Methods
The review protocol was conducted a priori according to the PRISMA (Preferred Reporting Items for Systematic Review and Meta-analysis) guidelines, and registered following the implementation of the search strategy in PROSPERO (identification N° CRD420251023900) ([Supplementary Appendix 1]).
Search Strategy
An electronic search was conducted using four databases: Medline via PubMed, Web of Science, Cochrane, and Scopus. The search was limited to the last 11 years (from 2013 to 2024).
MESH terms and Key words were used as presented below, to formulate two Boolean equations, in the different databases:
-
Equation 1: (root resorption [MESH] AND regenerative endodontics [MESH]).
-
Equation 2: (tooth resorption AND Platelet-Rich Fibrin).
Additional literature was searched through hand search by reviewing the references of articles selected through the electronic search process. Two calibrated reviewers (K.B.H.S. and G.A.M.) independently conducted the search and screening process. When disagreements or discrepancies arose, a third examiner (S.J.) was consulted. All conflicts were discussed and resolved through consensus among the three reviewers.
Duplicates were removed, and all titles and abstracts for studies that met the eligibility criteria were screened. Questionable titles were discussed until consensus was reached. Upon completion of screening, the full texts were retrieved.
Eligibility Criteria
The eligibility criteria were as follows:[6] [7] [8]
-
Study design: randomized controlled trials, prospective clinical studies, case series, and case report.
-
Participants: patients presenting with pathological root resorptions in permanent teeth, regardless of age or sex.
-
Intervention: REPs, including revascularization, platelet-rich fibrin (PRF), and platelet-rich plasma as defined by the original studies.
-
Comparators: conventional nonsurgical root canal treatment.
-
Outcomes: resolution or arrest of resorption, clinical absence of symptoms, and radiographic healing or reduction of lesions.
The exclusion criteria were as follows:
In vitro or animal studies, studies without sufficient clinical data on treatment outcomes, and studies involving primary teeth or previously treated teeth. Articles with insufficient data or not meeting the objectives of this review were also excluded.
Hence, the research question used was “Does regenerative endodontic treatment contribute to the management and healing of pathological root resorptions in permanent teeth?''
Data Collection Process (Reading Grid)
Data extraction and methodological quality assessment were performed independently by the authors. Data extraction was carried out using a data extraction grid ([Supplementary Appendix 2]). The grid included the following information: study design; sample size; the resorption type; the type of PRF used; and the treatment provided.
The data extracted were then compiled into a summary table for result analysis.
Quality Assessment of Included Studies
The quality of the included studies was evaluated based on the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (v5.1.0).[9]
These criteria included patient randomization, blinding methods, reporting of withdrawals and dropouts, clarity of statistical analysis, sample size estimation, measurement of multiple variables, well-defined inclusion and exclusion criteria, tested and clearly reported examiner reliability, and comprehensive reporting of all anticipated outcomes. Each study was then assigned a risk of bias classification (low, medium, or high). Two independent reviewers conducted the article selection process to ensure a broad collection of studies. The reviewers assessed each article according to predefined inclusion criteria and carried out unbiased evaluations, resolving any disagreements through discussion or consultation with a third reviewer (S.J.).
Additionally, the Newcastle–Ottawa Scale (NOS) for case–control studies[10] was applied to further assess the included studies. The evaluation focused on three main quality domains: selection (including case and group definition and representativeness), comparability (assessing how case and control groups were compared and controlling for confounding variables), and exposure (including outcome assessment, such as evaluating the accuracy of measurements by different examiners, study outcomes related to clinical tooth measurements, and use of a consistent assessment method for both groups, along with patient dropout rates). A star rating system was used to grade each study, with a maximum of 1 star for selection and outcome categories and up to 2 stars for comparability if sufficiently reported. Total scores for each study ranged from 1 to 8 stars. Due to variability in outcomes and study variables, a meta-analysis was not conducted in this review.
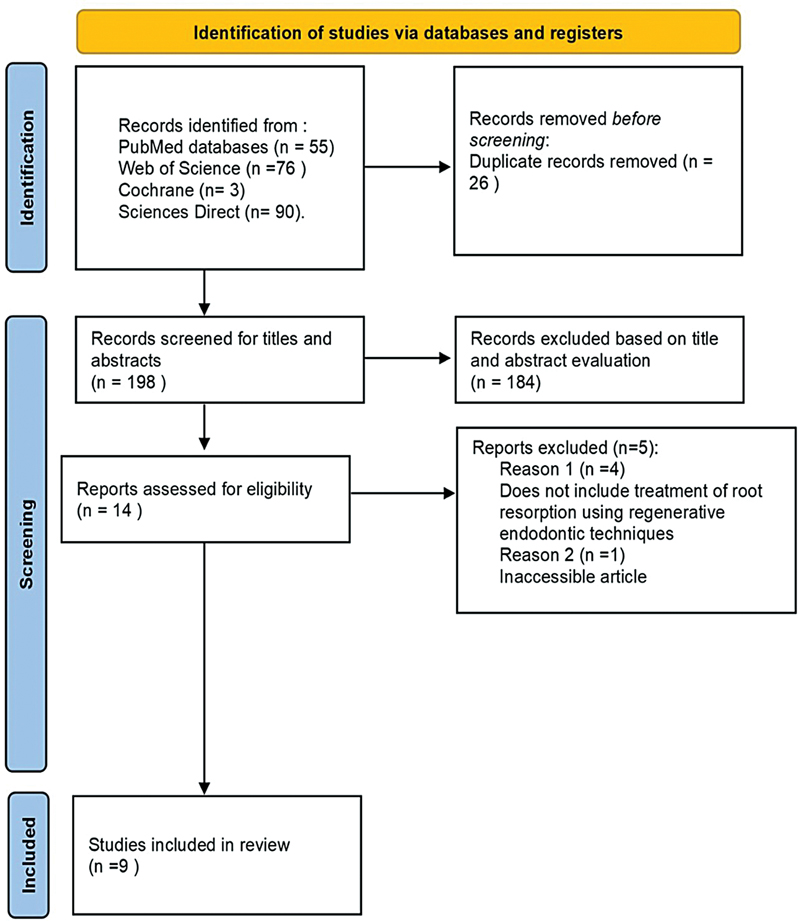
Search Results
A total of 224 articles were screened from all the databases. From those, 14 full-text articles were retrieved and 9 articles were finally included in the study ([Fig. 1]).
Data from studies included in this review are summarized and presented in [Tables 1] and [2].
|
Authors |
Gupta et al[11] |
Nageh et al[4] |
Yang et al[15] |
Arnold[16] |
Asgary et al[12] |
Kaval et al[17] |
Saoud et al[13] |
Santiago et al[5] |
Johns et al[14] |
|
|---|---|---|---|---|---|---|---|---|---|---|
|
Number of teeth |
1 |
13 |
1 |
1 |
6 |
1 |
1 |
3 |
1 |
|
|
Root resorption |
Internal |
Internal |
Internal |
Internal |
Cervical |
Internal |
Internal and external |
External |
Cervical |
|
|
Type of bioceramic |
MTA |
MTA |
MTA |
MTA |
CEM |
MTA |
MTA |
MTA |
– |
|
|
Type of PRF |
Not specified |
i-PRF |
L-PRF |
– |
– |
– |
– |
– |
Not specified |
|
|
Vascularization |
– |
– |
– |
Yes |
– |
Yes |
Yes |
Yes |
– |
|
|
Endodontic treatment specificity |
Shaping and cleaning NaOCl 5% Ca(OH)2 for 2 weeks Tri-ATB paste: for 2 weeks |
1) Shaping and cleaning NaOCl 1.5% + Ca(OH)2: 2–4 weeks 2) i-PRF injected until the cementoenamel junction, and the MTA was placed directly over the PRF |
Extraoral endodontic treatment MTA + L-PRF + reimplantation |
Disinfection of the infected portion of the root canal up to resorption Ca(OH)2 for 2 months |
Excavation of the resorption lacuna + pulpotomy or partial pulpectomy NaOCl 2.5% |
Shaping and cleaning of the root canal NaOCl 1% Ca(OH)2 4 months |
Shaping and cleaning of the root canal NaOCl 2.5% Ca(OH)2 2 weeks Tri-ATB paste: 2 weeks |
Shaping and cleaning of the root canal NaOCl 2.5–5.25% Tri-ATB paste 1 month |
Shaping and cleaning NaOCl 2.5% CHX 2% Ca(OH)2 Obturation with the reverse technique |
|
|
Follow-up |
Period (mo) |
24 |
12 |
24 |
36 |
12–36 |
24 |
19 |
15–30 |
24 |
|
Radiological exam |
Periapical X-ray |
CBCT |
CBCT |
CBCT |
Periapical X-ray |
CBCT |
Periapical X-ray |
Periapical X-ray |
Periapical X-ray |
|
Abbreviations: ATB, antibiotic; CBCT, cone-beam computed tomography; CEM, calcium-enriched mixture; MTA, mineral trioxide aggregate; PRF, platelet-rich fibrin.
|
Author |
Regenerative endodontic procedure |
Cicatrization |
Repair |
|---|---|---|---|
|
Gupta et al [11] |
Based on PRF |
• Stop the progression of root resorption. |
• Almost complete resolution of the periapical lesion. |
|
Nageh et al [4] |
Based on i-PRF |
• Stop the progression of root resorption. • Reduction in the volume of the resorption cavities. |
• Formation of mineralized tissue within the resorption defect. • Almost complete resolution of the periapical lesion. |
|
Yang et al [15] |
Based on L-PRF |
• Stop the progression of root resorption. |
• Resolution of the periapical lesion. |
|
Arnold [16] |
Revascularization |
• Stop the progression of root resorption. • Reduction in the volume of the resorption cavities. |
• Mild rebuilding of the root contour by mineralized bone-like tissue. |
|
Asgary et al [12] |
Revascularization |
• Stop the progression of root resorption. |
• Not specified. |
|
Kaval et al [17] |
Revascularization |
• Stop the progression of root resorption. |
• Root wall thickening by formation of mineralized tissue. • Remineralization within the resorption defect. |
|
Saoud et al [13] |
Basée sur la revascularisation |
• Stop the progression of root resorption. • Reduction in the volume of the resorption cavities. |
• Root wall thickening • Resolution of the periapical lesion. |
|
Santiago et al [5] |
Revascularization |
• Stop the progression of root resorption. |
• Root resorption lacunae replaced by mineralized tissue. |
|
Johns et al [14] |
Based on PRF |
• Stop the progression of root resorption. |
• Formation of bone-like mineralized tissue. |
Abbreviation: PRF, platelet-rich fibrin.
General Characteristics of Included Studies
From the 9 included articles, 5 were case studies, 3 were case series, and 1 was a clinical trial. The teeth described in the included studies represent a range of pathological resorption types, distributed as follows: 17 teeth with internal resorption, 3 with external resorption, 7 with external cervical resorption, and 1 with both internal and external resorption. Various treatment methods were employed for managing root resorption: 16 teeth were treated using PRF, while 12 teeth underwent revascularization ([Table 2]).
In this study, a range of radiological techniques was employed for both treatment and follow-up assessments, including retroalveolar radiography and cone-beam computed tomography (CBCT). Five articles utilized retroalveolar radiography,[5] [11] [12] [13] [14] while four articles used CBCT ([Table 2]).[4] [15] [16] [17]
General Outcomes of Included Studies
All the studies included in this work demonstrated clinical and radiological success, with a follow-up period of up to 36 months. In the clinical trial conducted by Nageh et al,[4] the clinical and radiological follow-up period was set at 12 months, at the end of which the authors prescribed a CBCT scan to assess the extent of tissue repair in areas of internal resorption ([Tables 1] and [2]).
Whether using two-dimensional radiographs[5] [11] [12] [13] [14] or three-dimensional CBCT images,[4] [15] [16] [17] all studies showed clinical success, with the pathological resorption process halted.
The results from the clinical trial on teeth exhibiting internal resorption, treated using a regenerative endodontic technique based on PRF, demonstrated a reduction in the volume of resorption cavities, with the formation of mineralized tissue in these defects.[4] Similarly, other studies focusing on the treatment of resorptions through revascularization also showed tissue repair and filling of the resorption areas with mineralized tissue.[5] [13] [16] [17]
Results of Quality Assessment
According to the standards described in the Cochrane Handbook for Systematic Reviews of Interventions (v5.1.0), the following findings were recorded in [Tables 3] and [4].
|
Author and year |
Randomization |
Blinding |
Withdrawal/dropout mentioned |
Variables measured many times |
Sample size estimation |
Inclusion/exclusion criteria clear |
Examiner reliability tested |
Expected outcomes prespecified |
Quality of study/bias risk |
|---|---|---|---|---|---|---|---|---|---|
|
Nageh et al [4] |
No |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Low |
Note: A study was graded to have a low risk of bias if it yielded 6 or more “yes” answers to the 9 questions, moderate risk if it yielded 3 to 5 “yes” answers, and high risk if it yielded 2 “yes” answers or less.
|
Author and year |
Selection |
Compatibility |
Exposure |
Newcastle–Ottawa quality (total) |
|---|---|---|---|---|
|
Gupta et al, 2022 [11] |
** |
** |
*** |
7 |
|
Yang et al, 2021 [15] |
** |
** |
*** |
7 |
|
Arnold, 2021 [16] |
** |
** |
*** |
7 |
|
Asgary et al, 2019 [12] |
∗∗∗ |
** |
*** |
8 |
|
Kaval et al, 2018 [17] |
∗ |
** |
*** |
6 |
|
Saoud et al, 2016 [13] |
** |
** |
*** |
7 |
|
Santiago et al, 2015 [5] |
** |
*** |
*** |
8 |
|
Johns et al, 2013 [14] |
** |
** |
** |
6 |
Note: A study can be awarded a maximum of 1 star (*) for each numbered item within the selection and exposure categories. A maximum of 2 stars can be given for comparability. Each study can be awarded a total of 9 stars. A study was rated to have a low risk of biasness if it received the maximum allowed number of 9 “stars” while moderate risk if it received 8, 7, or 6 “stars” and high risk if it received 5 “stars” or less.
The quality assessment of the clinical trial[4] indicates a low risk of bias ([Table 3] and [Fig. 2]).

Furthermore, “the quality assessment of selected studies on NOS was ranging from 4 to 8 stars.” A mean score of 7 was achieved for the included studies, as mentioned in [Table 4], all studies fall in the moderate bias category ([Table 4]).
Discussion
The Objective of this Systematic Review
The objective of this review is to evaluate the role of REPs in the management of pathological internal and external root resorptions in mature permanent teeth. The findings indicate that REPs are emerging as a viable alternative to conventional treatments, offering the potential for tooth preservation and regeneration.
Together with the damage of the pre-cement and the predentin, bacterial infection is one of the two main initiators of root resorption. Bacterial infiltration, whether of oral periodontal or traumatic origin, stimulates inflammation, resulting in activation of the clastic cells responsible for root resorption.[18]
The aim of conventional endodontic treatment is to recreate favorable conditions enabling resorption activity to be blocked by chemical, mechanical, or surgical treatment. So, the therapeutic success depends on the type of resorption, its location and severity, as well as the therapeutic technique used. In the best-case scenario, the root remains in its post-resorptive state and the periodontium can regenerate around it. The tooth maintained on the arch can then continue to provide function and aesthetics.[19]
Recently, pulpal revascularization or PRF has been used in the treatment of inflammatory pathological root resorption.
Regenerative Endodontics Based on Platelet-Rich Fibrin
The platelet concentrate has been developed by Choukroun et al.[20] This concentrate contains fibrin, growth factors, and immune mediator cells that influence healing. In 2004, they evaluated the effect of PRF on bone regeneration and demonstrated accelerated bone healing in the PRF group. Recently, they further refined this technique and proposed new preparation protocols called injected-PRF (i-PRF) and L-PRF.[21] [22]
A large number of in vitro studies have shown that PRF promotes the migration, the proliferation and the differentiation of epithelial, fibroblastic, osteoblastic, and mesenchymal stem cells. As a result, its potential applications have broadened and today PRF is widely used in endodontics. In this context, Gupta et al in 2022[11] used a PRF membrane in combination with MTA (mineral trioxide aggregate) to fill teeth with internal resorptions. They concluded that this technique was effective in stopping the progression of this pathological process.
As for Nageh et al,[4] they choose i-PRF in the treatment of internal resorptions as it can be easily injected into the canal and fill irregular resorption cavities. The technique used is based on chemo-mechanical canal preparation followed by inter-appointment medication with calcium hydroxide. Then, in the second appointment, the i-PRF was injected into the root canal until the cementoenamel junction, and the MTA was placed directly over the PRF. The authors assert, after a 12-month radiological control using CBCT, that all cases showed a decrease in the volume of resorption cavities by 21.88%.
In contrast, other studies choose the L-PRF to treat internal resorption. In fact, this type of PRF contains a higher quantity of leukocytes and platelets.[15]
According to the authors, L-PRF served as a scaffold material due to its osteogenic potential and antibacterial properties. After 18 months, this technique arrests the pathological resorption process without decreasing the volume of resorption cavities.
With regard to the management of cervical resorptions, Asgary et al[12] concluded that the complete or the partial removal of resorption lacunae, followed by partial pulpotomy or pulpectomy, and the placement of a bioactive cement can stop the resorption process within 12 months.
For the treatment of invasive cervical resorptions, the authors suggest starting with conventional endodontic treatment followed by surgical excavation of the granulation tissue, combined with periodontal regeneration based on allograft and PRF membrane.
This technique allowed significant bone fill after a 24-month follow-up period and no progression of resorption.
Regenerative Endodontics Based on Revascularization
Revascularization is a therapeutic approach within the framework of regenerative endodontics. It was initially indicated for the treatment of necrotic immature permanent teeth to restore root development and tissue regeneration. This protocol has proven effective in managing immature permanent teeth.[23] [24] [25]
Arnold[16] used the revascularization technique in the treatment of internal root resorption. He disinfected only the coronal portion of the canal relative to the resorption cavity. The author recommend a follow-up till 3 years and based on CBCT. According to him, neoformed bone tissue partially penetrated the area of the resorption without direct contact with the root dentin.
However, other authors[13] [17] used the classic revascularization technique with complete root canal system disinfection and concluded that this technique allows a thickening of the canal walls in the area of internal resorption associated with remineralization inside the resorption defect. They advise a follow-up of 14 months to 36 months based on a CBCT.
Indeed, thanks to the revascularization technique, the size of the internal root resorption was reduced due to thickening of the canal walls in the area of internal resorption, thereby reinforcing the tooth.
Concerning the contribution of this technique to the treatment of external root resorption, Santiago et al in 2015[5] employed for the first time, to our knowledge, the revascularization technique for the treatment of external root resorptions. According to the authors, this technique resulted in the cessation of the pathological process within 3 months, with resolution of radiolucent periapical areas and filling of the resorption areas with newly formed hard tissue.
Limitations
One of the notable limitations of this systematic review is the heterogeneity in follow-up periods reported across the included studies, which ranged from 6 to 36 months. This variation complicates direct comparisons of treatment outcomes and introduces potential bias in assessing the long-term effectiveness of REPs. Shorter follow-up durations may not fully capture delayed healing or recurrence of resorption, while longer periods may reflect more stable outcomes. As such, the variability in follow-up limits the ability to draw definitive conclusions regarding treatment predictability and success over time. Future studies should aim for more standardized and extended follow-up protocols to ensure more robust and comparable clinical data.
Clinical Implications
The clinical implications of adopting REPs for managing root resorptions are significant. By focusing on regenerative approaches, clinicians can potentially extend the lifespan of affected teeth and maintain patient quality of life. The American Association of Endodontists emphasizes the importance of minimally invasive strategies in contemporary endodontics, aligning with the principles of REPs that prioritize the conservation of tooth structure and vitality.[26]
Moreover, REPs may reduce the need for extraction and subsequent restorative procedures, thereby decreasing overall treatment costs and patient morbidity. As dental practitioners increasingly adopt evidence-based practices, the incorporation of REPs can enhance treatment paradigms in endodontics, especially for complex cases of root resorption.
Future Directions
Future research should focus on refining treatment protocols and establishing standardized outcome measures. Investigating the role of advanced biomaterials, such as hydrogels and synthetic scaffolds, may provide insights into enhancing regenerative potential (Zhang et al).[27] Furthermore, exploring innovative techniques, including gene therapy and enhanced stem cell sourcing, could push the boundaries of regenerative capabilities in endodontics.
Collaborative multicenter studies are crucial to developing comprehensive guidelines for the application of REPs. Such research initiatives would help gather robust data on patient outcomes, identify factors influencing success rates, and ultimately shape clinical best practices.
In conclusion, REPs represent a significant advancement in the management of pathological internal and external root resorptions in immature permanent teeth. The available literature suggests that REPs offer promising outcomes, particularly in promoting healing and preserving tooth vitality. However, continued research is essential to address current limitations, optimize treatment protocols, and ensure long-term success. By embracing these innovative strategies, clinicians have the opportunity to enhance patient outcomes and foster a new standard of care in endodontics.[27]
Conclusion
The present systematic review shows the effectiveness of regenerative procedures in the treatment of pathological resorptions and the reduction in the size of resorption cavities in the case of internal resorption.
Conflict of Interest
None declared.
Presentation at a Meeting
None.
Organization
None.
-
References
- 1 American Association of Endodontists. Glossary of Endodontic Terms. 10th ed.. Chicago, IL: American Association of Endodontists; 2020
- 2 Bartok RI, Văideanu T, Dimitriu B, Vârlan CM, Suciu I, Podoleanu D. External radicular resorption: selected cases and review of the literature. J Med Life 2012; 5 (02) 145-148
- 3 Haapasalo M, Endal U. Internal inflammatory root resorption: the unknown resorption of the tooth. Endod Top. Juill 2006; 14 (01) 60-79
- 4 Nageh M, Ibrahim LA, AbuNaeem FM, Salam E. Management of internal inflammatory root resorption using injectable platelet-rich fibrin revascularization technique: a clinical study with cone-beam computed tomography evaluation. Clin Oral Investig 2022; 26 (02) 1505-1516
- 5 Santiago CN, Pinto SS, Sassone LM, Hirata Jr R, Fidel SR. Revascularization technique for the treatment of external inflammatory root resorption: a report of 3 cases. J Endod 2015; 41 (09) 1560-1564
- 6 Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009; 6 (07) e1000097
- 7 Moher D, Shamseer L, Clarke M. et al; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 2015; 4 (01) 1
- 8 Shamseer L, Moher D, Clarke M. et al; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ 2015; 350: g7647
- 9 Higgins JP, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Vol. 4. Chichester (UK): John Wiley & Sons; 2011
- 10 Wells GA, Shea B, O'Connell D. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Ottawa, ON, Canada: Ottawa Hospital Research Institute; 2011
- 11 Gupta G, Agarwal A, Ansari AA, Singh RK. Non-surgical management of a large periapical lesion with internal resorption using PRF, hydroxyapatite and MTA. BMJ Case Rep 2022; 15 (09) e248907
- 12 Asgary S, Nourzadeh M, Verma P, Hicks ML, Nosrat A. Vital pulp therapy as a conservative approach for management of invasive cervical root resorption: a case series. J Endod 2019; 45 (09) 1161-1167
- 13 Saoud TMA, Mistry S, Kahler B, Sigurdsson A, Lin LM. Regenerative endodontic procedures for traumatized teeth after horizontal root fracture, avulsion, and perforating root resorption. J Endod 2016; 42 (10) 1476-1482
- 14 Johns DA, Shivashankar VY, Maroli RK, Joseph R. Invasive cervical root resorption: engineering the lost tissue by regeneration. Contemp Clin Dent 2013; 4 (04) 536-539
- 15 Yang Y, Zhang B, Huang C, Ye R. Intentional replantation of a second premolar with internal resorption and root fracture: a case report. J Contemp Dent Pract 2021; 22 (05) 562-567
- 16 Arnold M. Reparative endodontic treatment of a perforating internal inflammatory root resorption: a case report. J Endod 2021; 47 (01) 146-155
- 17 Kaval ME, Güneri P, Çalışkan MK. Regenerative endodontic treatment of perforated internal root resorption: a case report. Int Endod J 2018; 51 (01) 128-137
- 18 Fuss Z, Tsesis I, Lin S. Root resorption–diagnosis, classification and treatment choices based on stimulation factors. Dent Traumatol 2003; 19 (04) 175-182
- 19 Hegde N, Hegde MN. Internal and external root resorption management: a report of two cases. Int J Clin Pediatr Dent 2013; 6 (01) 44-47
- 20 Choukroun J, Adda F, Schoeffler C, Vervelle A. Une opportunité en paro-implantologie: le PRF [in French]. Implantodontie 2001; (42) 55-62
- 21 Mourão CF, Valiense H, Melo ER, Mourão NB, Maia MD. Obtention of injectable platelets rich-fibrin (i-PRF) and its polymerization with bone graft: technical note. Rev Col Bras Cir 2015; 42 (06) 421-423
- 22 Munoz F, Jiménez C, Espinoza D, Vervelle A, Beugnet J, Haidar Z. Use of leukocyte and platelet-rich fibrin (L-PRF) in periodontally accelerated osteogenic orthodontics (PAOO): clinical effects on edema and pain. J Clin Exp Dent 2016; 8 (02) e119-e124
- 23 Patel S, Saberi N, Pimental T, Teng PH. Present status and future directions: root resorption. Int Endod J 2022; 55 (Suppl. 04) 892-921
- 24 Pruthi PJ, Goel S, Yadav P, Nawal RR, Talwar S. Novel application of a calcium silicate‒based cement and platelet-rich fibrin in complex endodontic cases: a case series. Gen Dent 2020; 68 (03) 46-49
- 25 Priya M H, Tambakad PB, Naidu J. Pulp and periodontal regeneration of an avulsed permanent mature incisor using platelet-rich plasma after delayed replantation: a 12-month clinical case study. J Endod 2016; 42 (01) 66-71
- 26 American Association of Endodontists. AAE position statement on regenerative endodontics. J Endod 2022; 48 (04) 401-407
- 27 Zhang R, Li J, Chen H, Wang Y. Advanced biomaterials in regenerative endodontics: a review of current trends and futures directions. Clin Oral Investig 2024; 28 (01) 45-60
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
15. September 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 American Association of Endodontists. Glossary of Endodontic Terms. 10th ed.. Chicago, IL: American Association of Endodontists; 2020
- 2 Bartok RI, Văideanu T, Dimitriu B, Vârlan CM, Suciu I, Podoleanu D. External radicular resorption: selected cases and review of the literature. J Med Life 2012; 5 (02) 145-148
- 3 Haapasalo M, Endal U. Internal inflammatory root resorption: the unknown resorption of the tooth. Endod Top. Juill 2006; 14 (01) 60-79
- 4 Nageh M, Ibrahim LA, AbuNaeem FM, Salam E. Management of internal inflammatory root resorption using injectable platelet-rich fibrin revascularization technique: a clinical study with cone-beam computed tomography evaluation. Clin Oral Investig 2022; 26 (02) 1505-1516
- 5 Santiago CN, Pinto SS, Sassone LM, Hirata Jr R, Fidel SR. Revascularization technique for the treatment of external inflammatory root resorption: a report of 3 cases. J Endod 2015; 41 (09) 1560-1564
- 6 Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009; 6 (07) e1000097
- 7 Moher D, Shamseer L, Clarke M. et al; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 2015; 4 (01) 1
- 8 Shamseer L, Moher D, Clarke M. et al; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ 2015; 350: g7647
- 9 Higgins JP, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Vol. 4. Chichester (UK): John Wiley & Sons; 2011
- 10 Wells GA, Shea B, O'Connell D. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Ottawa, ON, Canada: Ottawa Hospital Research Institute; 2011
- 11 Gupta G, Agarwal A, Ansari AA, Singh RK. Non-surgical management of a large periapical lesion with internal resorption using PRF, hydroxyapatite and MTA. BMJ Case Rep 2022; 15 (09) e248907
- 12 Asgary S, Nourzadeh M, Verma P, Hicks ML, Nosrat A. Vital pulp therapy as a conservative approach for management of invasive cervical root resorption: a case series. J Endod 2019; 45 (09) 1161-1167
- 13 Saoud TMA, Mistry S, Kahler B, Sigurdsson A, Lin LM. Regenerative endodontic procedures for traumatized teeth after horizontal root fracture, avulsion, and perforating root resorption. J Endod 2016; 42 (10) 1476-1482
- 14 Johns DA, Shivashankar VY, Maroli RK, Joseph R. Invasive cervical root resorption: engineering the lost tissue by regeneration. Contemp Clin Dent 2013; 4 (04) 536-539
- 15 Yang Y, Zhang B, Huang C, Ye R. Intentional replantation of a second premolar with internal resorption and root fracture: a case report. J Contemp Dent Pract 2021; 22 (05) 562-567
- 16 Arnold M. Reparative endodontic treatment of a perforating internal inflammatory root resorption: a case report. J Endod 2021; 47 (01) 146-155
- 17 Kaval ME, Güneri P, Çalışkan MK. Regenerative endodontic treatment of perforated internal root resorption: a case report. Int Endod J 2018; 51 (01) 128-137
- 18 Fuss Z, Tsesis I, Lin S. Root resorption–diagnosis, classification and treatment choices based on stimulation factors. Dent Traumatol 2003; 19 (04) 175-182
- 19 Hegde N, Hegde MN. Internal and external root resorption management: a report of two cases. Int J Clin Pediatr Dent 2013; 6 (01) 44-47
- 20 Choukroun J, Adda F, Schoeffler C, Vervelle A. Une opportunité en paro-implantologie: le PRF [in French]. Implantodontie 2001; (42) 55-62
- 21 Mourão CF, Valiense H, Melo ER, Mourão NB, Maia MD. Obtention of injectable platelets rich-fibrin (i-PRF) and its polymerization with bone graft: technical note. Rev Col Bras Cir 2015; 42 (06) 421-423
- 22 Munoz F, Jiménez C, Espinoza D, Vervelle A, Beugnet J, Haidar Z. Use of leukocyte and platelet-rich fibrin (L-PRF) in periodontally accelerated osteogenic orthodontics (PAOO): clinical effects on edema and pain. J Clin Exp Dent 2016; 8 (02) e119-e124
- 23 Patel S, Saberi N, Pimental T, Teng PH. Present status and future directions: root resorption. Int Endod J 2022; 55 (Suppl. 04) 892-921
- 24 Pruthi PJ, Goel S, Yadav P, Nawal RR, Talwar S. Novel application of a calcium silicate‒based cement and platelet-rich fibrin in complex endodontic cases: a case series. Gen Dent 2020; 68 (03) 46-49
- 25 Priya M H, Tambakad PB, Naidu J. Pulp and periodontal regeneration of an avulsed permanent mature incisor using platelet-rich plasma after delayed replantation: a 12-month clinical case study. J Endod 2016; 42 (01) 66-71
- 26 American Association of Endodontists. AAE position statement on regenerative endodontics. J Endod 2022; 48 (04) 401-407
- 27 Zhang R, Li J, Chen H, Wang Y. Advanced biomaterials in regenerative endodontics: a review of current trends and futures directions. Clin Oral Investig 2024; 28 (01) 45-60