

Subscribe to RSS
DOI: 10.1055/s-0045-1810063
Herbal Medicines: The Double-Edged Sword for Brain—A Narrative Update
Authors


Abstract
Phytochemicals or herbal medicines (HMs) with neuroprotective and nootropic properties are being increasingly utilized in various neurological conditions owing to their antioxidative, anti-inflammatory, and antiapoptotic properties, as well as their role in immune regulation, hormonal regulation, and modulation of neurotransmitters and ion channels. While HMs are often regarded as safe, they are not without risks. The aim of this review was to know the various neurological and non-neurological side effects of long-term consumption of neuroprotective and nootropic phytochemicals. An electronic search was conducted using the following databases from January 2000 to December 2023: PubMed, PubMed Central, Embase, Scopus, and Science Citation Index (Web of Science). Only studies published in the English language were considered. The search used key terms such as “Herbs,” “Phytochemicals,” “India,” “Asia,” “Neuroprotection,” “Neurological diseases,” and “Complications.” The sources included research articles, systematic reviews and meta-analyses, narrative reviews, and editorials. Letters to the editor, commentaries, abstracts only, and unpublished data were excluded. While HMs are increasingly being used therapeutically for various neurological and non-neurological conditions, they also carry the risk of adverse effects due to contamination, adulteration, direct effects of metabolites, herb–drug interactions, interindividual susceptibility, and other factors. In addition, widespread availability, over-the-counter sale, and unsupervised dosing are the key reasons for their unregulated prolonged use. As such, correct identification of HMs and consequent assessment of their toxicological profile are deemed extremely crucial. Neurotoxicity testing for HMs is challenging considering the limitations of traditional methods (morphological, microscopic, and chemical); nevertheless, in the recent years, several novel procedures have been developed. Large studies are warranted to establish the safety profile of consuming HMs either alone or in combination in humans.
Introduction
Herbal medicines (HMs), also called botanical medicine, phytomedicine, or phytotherapy, refer to herbs, herbal materials, herbal preparations, and finished herbal products that contain parts of plants or other materials as active ingredients. The plant components used in herbal therapy include roots, seeds, stems, berries, leaves, fruits, bark, flowers, or even the whole plants. Some HMs are also prepared from excretory plant products such as gum, resins, and latex.[1] Typically, HMs are available in different forms, such as capsules, powders, infusions, poultices, and essential oils. Archaeologically, the use of HMs dates back to the Paleolithic age, approximately 60,000 years ago. However, written records of their use are evinced for the past 5,000 years.[2] Chinese, Indian, and Arabic are the three most influential traditional medicine systems to improve public health problems.[1] [2]
The use of HMs or products, either by itself or in conjunction with other therapies, to treat medical ailments has achieved tremendous popularity in recent years. Consumer demand for HMs is rising exponentially. One of the prime reasons for increased consumption of HMs is due to their easy availability and cost-effectiveness. Other reasons for this resurgence can possibly be attributed to the side effects of allopathic drugs, lack of concrete curative therapy for several chronic diseases, snowballing antimicrobial resistance, as well as the hefty investment in pharmaceutical research and development.[3] A recent report by World Health Organization (WHO) stated that around 80% of the world's population is estimated to use traditional medicines encompassing ancient practices such as acupuncture, ayurvedic medicine and herbal mixtures, as well as modern medicines.[4]
HMs have been effectively experimented in laboratories for various neurological and non-neurological disease conditions, but with variable success rate in humans. While HMs are often regarded safe, they are not without risks. In this article, we have provided a narrative update on the current role of HMs in different neurological conditions, their mechanism of neuroprotection and neurorestoration, and the potential neurological and non-neurological side effects and complications.
Literature Search
An electronic search was conducted using the following databases from January 2000 to December 2023: PubMed, PubMed Central, Embase, Scopus, and Science Citation Index (Web of Science). Only studies published in the English language were considered. The search used key terms such as “Herbs,” “Phytochemicals,” “India,” “Asia,” “Neuroprotection,” “Neurological diseases,” and “Complications.” The sources included research articles, systematic reviews and meta-analyses, narrative reviews, and editorials. Letters to the editor, commentaries, abstracts only, and unpublished data were excluded.
Neurological Indications and Mechanisms
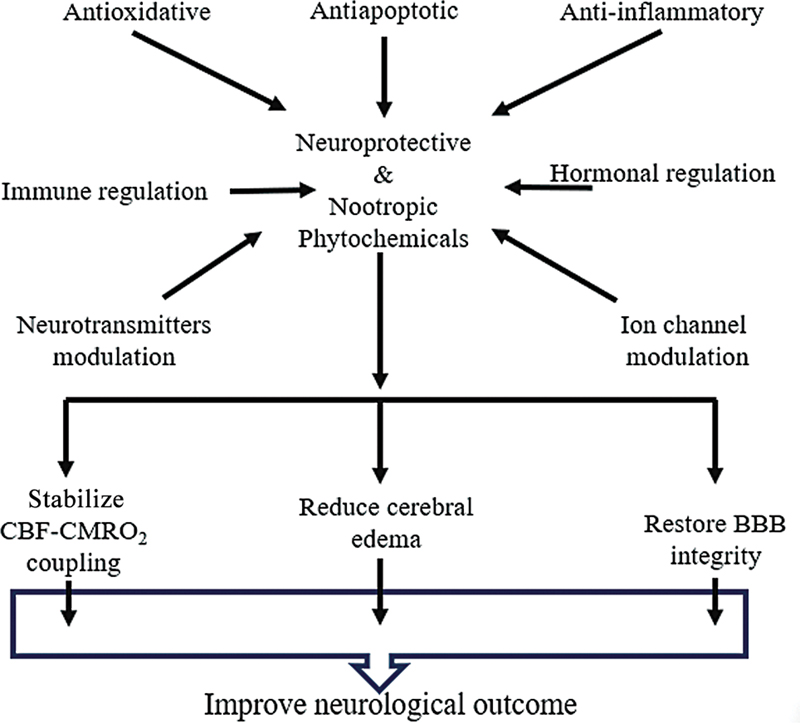
A good number of phytochemicals with neuroprotective and nootropic properties have been tried experimentally and clinically in various neurological conditions like ischemic brain injury,[5] [6] [7] traumatic brain injury (TBI),[8] [9] subarachnoid hemorrhage,[10] [11] Parkinson's disease,[12] [13] Huntington's disease,[14] [15] Alzheimer's disease,[16] [17] multiple sclerosis,[18] [19] brain tumors,[20] [21] seizure disorders,[22] [23] primary headache disorders,[24] [25] meningitis,[26] [27] neuropsychiatric conditions (anxiety, depression, stress, insomnia),[28] [29] [30] etc. ([Table 1]). Numerous mechanisms mediate their neuroprotective and neurorestorative roles, the prominent ones being antioxidative, anti-inflammatory, and antiapoptotic properties, and their role in immune regulation, hormonal regulation, and modulation of neurotransmitters and ion channels.[31] [32] [33] In addition, a few phytochemicals also possess antiproliferative, antiamyloidogenic, antiviral, and antidiabetic properties.[34] At the molecular level, different neuroprotective mechanisms of phytochemicals include signaling pathways such as hypoxia-inducible factor 1 (HIF-1), nuclear factor erythroid 2-related factor 2 (Nrf2), and heme oxygenase-1 (HO-1); free radical scavenging, reduction of nitric oxide (NO) toxicity and acetylcholine esterase (AChE) activity, decrease of phosphorylated AKT (pAkt) and its downstream targets, downregulation of the aquaporin-4 (AQP-4) and toll-like receptor 4 signal, reduction in malondialdehyde and NO levels, increasing neuronal density in the hippocampus, and inhibition of oxidative stress.[35] [36] It is claimed that these mechanisms stabilize the balance between cerebral blood flow (CBF) and cerebral metabolic rate (CMR) of oxygen consumption, reduce cerebral edema, and restore blood–brain barrier (BBB) integrity, thereby improving neurological outcome ([Fig. 1]).
|
Botanical name |
Corresponding common name in India |
Corresponding major constituents |
|---|---|---|
|
1. Acorus calamus 2. Allium sativum 3. Aloe barbadensis Miller 4. Bacopa monnieri 5. Cannabis sativa 6. Carthamus tinctorius L. 7. Carum carvi 8. Carum roxburghianum 9. Celastrus paniculatus 10. Centella asiatica 11. Cissampelos pareira 12. Claviceps purpurea 13. Clitoria ternatea 14. Convolvulus pluricaulis 15. Coriandrum sativum 16. Crocus sativus 17. Cuminum cyminum 18. Curcuma longa 19. Desmodium gangeticum 20. Eclipta alba 21. Ginkgo biloba 22. Hypericum perforatum (St. John's wort) 23. Juglans regia 24. Moringa oleifera 25. Mucuna pruriens 26. Nigella sativa 27. Passiflora incarnata 28. Piper longum 29. Piper methysticum 30. Piper nigrum 31. Valeriana jatamansi 32. Withania somnifera 33. Zingiber officinale 34. Artemisia dracunculus [a] 35. Resveratrol[a] |
1. Sweet flag/vacha 2. Garlic/lahsun 3. Aloe vera 4. Brahmi 5. Bhang/ganja/charas 6. Safflower/kusum 7. Krishna jeera/black cumin 8. Ajmoda/ajwain 9. Jyotismati 10. Mandukparni/jalbrahmi 11. Patha 12. Ergot 13. Aparajit/kakkattan 14. Shankhpushpi 15. Dhaniya 16. Saffron/kesar 17. Jeera 18. Circumin/turmeric/haldi 19. Shalparni 20. Bringharaj 21. Maidenhair tree 22. Basani/mongulu 23. Walnut 24. Drumstick 25. Kawaanch 26. Kalonji/kaala jeera 27. Krishna kamal 28. Pippali 29. Kava 30. Black pepper/kali mirch 31. Sugandhbala/tagar 32. Indian ginseng/ashwagandha 33 Fresh ginger (adrak)/dry ginger (sonth) |
1. β-asarone, α-asarone, eugenol, calamusonol 2. Allicin, flavonoids, terpenes 3. Aloe-emodin, aloin, aloesin, emodin, acemannan 4. Saponins, triterpenoids, betulinic acid, sterols 5. Cannabinoids, terpenoids, flavonoids 6. Quercetin, kaempferol, matairesinol, linoleic acid, sterols 7. Carvone, limonene, quercetin, kaempferol, linoleic acid 8. d-limonene, α-terpinene, and d-piperitone, d-linalool 9. Celastrine, paniculatine, celapagine, celapanine paniculatus, oleic acid 10. Asiaticoside, centelloside, asiatic acid 11. Berberine, hayatine, quercetin, kaempferol, saponins 12. Ergotamine, ergovaline, ergocristine, ergometrine 13. Quercetin, kaempferol, ternatins 14. Triterpenoids, flavonol, glycosides, steroids 15. Linalool (terpene alcohol), neryl acetate, γ-terpinene, α-pinene 16. Crocin, picrocrocin and safranal 17. Cuminaldehyde, cymene, terpenoids, apigenin, luteolin, ferulic acid, linolenic acid 18. Circumin, turmerone, zingiberene 19. Desmodin, gangetin, quercetin, kaempferol, triterpenoids, saponins 20. Coumestans (wedololactone, demethylwedelolactone), flavonoids, triterpenes 21. Ginkgolides, bilobalide, lactones 22. Hypericin, hyperforin, flavonoids, tannins 23. Alpha-linolenic acid, ellagic acid, quercetin, kaempferol, tannins 24. Flavonoids, alkaloids, phenols, vitamins 25. L-dopa, mucunine, mucunadine, tannins, flavonoids, saponins 26. Thymoquinone, nigellone, α-hederin, carvacrol 27. Apigenin, luteolin, vitexin, passiflorine, saponins, coumarins 28. Piperine, piperlongumine, piperic acid, flavonoids, saponins 29. Kavalactones (kavain, dihydrokavain, yangonin, methysticin), flavokawains, kavapyrones 30. Piperine, piperlongumine, piperic acid, flavonoids, saponins 31. Valerenic acid, isovaleric acid, β-caryophyllene, flavonoids, saponins 32. Withanolides (withanolide A, withanolide D), withanine, withaferins, saponins 33. Gingerol, shogaol, zingerone 34. Estragole, eucalyptol, α-pinene, flavonoids, tannins 35. Piceatannol, pterostilbene |
a Name commonly used in India for these phytochemicals could not be found in the literature.
Factors Contributing to Adverse Health Outcomes with HMs
HMs are often perceived as safe due to their natural origin, but they can have various side effects and complications. Mild to moderate adverse effects include allergic reaction, rash, dermatitis, asthma, dry mouth, headache, dizziness, agitation, seizure, fatigue, sinus arrythmia, gastrointestinal upset, muscle spasm, muscle weakness, sleep disorder, dyselectrolytemia, nausea, vomiting, loss of appetite, etc. Severe side effects like life-threatening anaphylactic reaction, coagulopathy, life-threatening arrythmia, organ toxicity (hepatotoxicity, nephrotoxicity, cardiotoxicity, neurotoxicity, etc.), carcinoma, cardiac arrest, and even death have been reported.[36] [37] [38] [39] The causes of HM-induced side effects can be multifactorial and can occur during the preparation phase or consumption phase or both.[40] [41] [42] [43] [44] [45]
-
Preparation phase: Inappropriate process of extract preparation, unsuitable storage conditions, contamination with heavy metals, microbial contamination, radioactive contamination, cross-contamination, product substitution, adulteration, inconsistent quality testing and control, etc.
-
Consumption phase: Direct toxic effects of active constituents or metabolites, unregulated administration, imprecise dosing, herb–drug interactions, interindividual variability (age, diet, preexisting clinical status, genetic polymorphism, polypharmacy), etc.
Neurological Adverse Effects
Numerous neurological adverse effects of HMs, such as cerebral edema, cerebral arteritis, convulsions, delirium, encephalopathy, mood disturbances, hallucinations, psychosis, paresthesia, and cerebrovascular accidents, have been described in the literature. These neurological adverse effects can result from several mechanisms (as described above); however, the predominant ones include direct neurotoxicity, interaction with neurotransmitter systems, and herb–drug interactions.[37] [38] [39] [40] [46] Also, there is growing evidence that few HMs contain potentially harmful levels of heavy metals like mercury, arsenic, and lead, all of which contribute to neurotoxicity.[47] [48] Illegal drug usage for recreational purposes could be another factor for HM-induced neurotoxicity ([Table 2]). These effects can vary based on the dosage, duration of use, route of exposure, individual susceptibility, and the specific herbal preparation used.[42] [43] [44] [45] Damage to the central nervous system (CNS) or peripheral nervous system (PNS) may be subtle initially and may not be detected unless specific behavioral tests for coordination, memory, and learning are performed. This enigmatic type of toxicity is a feature of many types of HMs, where low doses of herbal toxins may be ingested over a long period of time.[49]
Abbreviations: CCBs, calcium channel blockers; CNS, central nervous system; HIV, human immunodeficiency virus; MAOIs, monoamine oxidase inhibitors; NNRTIs, non-nucleoside reverse transcriptase inhibitors; PIs, protease inhibitors; SNRIs, serotonin and norepinephrine reuptake inhibitors; SSRIs, selective serotonin reuptake inhibitors; TCAs, tricyclic antidepressants.
Safety Evaluation
The major hurdle in using HMs either alone or in combination for prophylactic and/or therapeutic purposes is the lack of concrete scientific evidence with regard to their pharmacokinetic and pharmacodynamic profile, human equivalent dose, potential side effects, herb–herb and herb–drug interactions, and possible antidotes. However, the biggest challenge is the accurate identification and authentication of the raw herbal material and also the final marketed products. Traditional methods of authentication include morphological, microscopic, and chemical characterization; nevertheless, in the recent years, several novel and inventive procedures have gained traction. While DNA sequencing may be effectively used to detect pollutants and adulteration, omics has emerged as a useful research tool for prediction and toxicity evaluation.[44] [45] Further, computational models and in silico predictions based on the chemical structure of herbal compounds can further predict toxicity potential.[50] [51] [52] Integrating data from these various approaches ensure a thorough evaluation of the toxicological profile associated with HMs.
Precautionary Measures during Consumption
HMs should be prescribed by a physician and should not be consumed unmonitored (especially by pregnant and lactating mothers). Over-the-counter sale of HMs should be prohibited. Before consuming, the label (dosage, potential side effects, interactions, and contraindications, etc.) and expiry date should be checked for the seal of the regulatory authority. HMs containing heavy metals like mercury, arsenic, and lead should not be used. If an HM is consumed with any other herbal preparation or allopathic medicine, it should be informed to the treating physician. Any noticeable adverse effect should be immediately notified to the physician.[53] [54] [55]
Conclusion
While certain HMs demonstrate potential neuroprotective effects, they are also associated with a range of neurological and non-neurological adverse effects. The diverse phytochemicals present in HMs may exert additive or synergistic actions in vivo, which can enhance or, in some cases, inhibit their therapeutic efficacy. Therefore, it is essential to use HMs cautiously, adhering to recommended dosages and under the supervision of a qualified health care professional. Although evaluating their toxicological potential remains a complex task, ongoing research into species authentication, identification of toxic phytochemicals, elucidation of toxicity mechanisms, and quantification of environmental contaminants in HMs is commendable. Large-scale clinical studies are needed to comprehensively establish the safety profile of HMs, whether used individually or in combination.
Conflict of Interest
None declared.
-
References
- 1 Pan SY, Litscher G, Gao SH. et al. Historical perspective of traditional indigenous medical practices: the current renaissance and conservation of herbal resources. Evid Based Complement Alternat Med 2014; 2014: 525340
- 2 Kurhekar JV. Ancient and modern practices in phytomedicine. In: Egbuna C, Prakash Mishra A, Goyal MG. eds. Preparation of Phytopharmaceuticals for the Management of Disorders. Cambridge, MA: Academic Press; 2021: 55-75
- 3 Pan SY, Pan S, Yu ZL. et al. New perspectives on innovative drug discovery: an overview. J Pharm Sci 2010; 13 (03) 450-471
- 4 Halder S, Anand U, Nandy S. et al. Herbal drugs and natural bioactive products as potential therapeutics: a review on pro-cognitives and brain boosters perspectives. Saudi Pharm J 2021; 29 (08) 879-907
- 5 Fan F, Lei M. Mechanisms underlying curcumin-induced neuroprotection in cerebral ischemia. Front Pharmacol 2022; 13: 893118
- 6 Feng Z, Sun Q, Chen W, Bai Y, Hu D, Xie X. The neuroprotective mechanisms of ginkgolides and bilobalide in cerebral ischemic injury: a literature review. Mol Med 2019; 25 (01) 57
- 7 Xue R, Gao S, Zhang Y. et al. A meta-analysis of resveratrol protects against cerebral ischemia/reperfusion injury: evidence from rats studies and insight into molecular mechanisms. Front Pharmacol 2022; 13: 988836
- 8 Keshavarzi Z, Shakeri F, Barreto GE, Bibak B, Sathyapalan T, Sahebkar A. Medicinal plants in traumatic brain injury: neuroprotective mechanisms revisited. Biofactors 2019; 45 (04) 517-535
- 9 Lee B, Leem J, Kim H, Jo HG, Kwon CY. Herbal medicine for traumatic brain injury: a systematic review and meta-analysis of randomized controlled trials and limitations. Front Neurol 2020; 11: 772
- 10 Wakade C, King MD, Laird MD, Alleyne Jr CH, Dhandapani KM. Curcumin attenuates vascular inflammation and cerebral vasospasm after subarachnoid hemorrhage in mice. Antioxid Redox Signal 2009; 11 (01) 35-45
- 11 Tan J, Song R, Luo S. et al. Efficacy of resveratrol in experimental subarachnoid hemorrhage animal models: a stratified meta-analysis. Front Pharmacol 2022; 13: 905208
- 12 Amro MS, Teoh SL, Norzana AG, Srijit D. The potential role of herbal products in the treatment of Parkinson's disease. Clin Ter 2018; 169 (01) e23-e33
- 13 Yin R, Xue J, Tan Y. et al. The positive role and mechanism of herbal medicine in Parkinson's disease. Oxid Med Cell Longev 2021; 2021: 9923331
- 14 Lum PT, Sekar M, Gan SH, Bonam SR, Shaikh MF. Protective effect of natural products against Huntington's disease: an overview of scientific evidence and understanding their mechanism of action. ACS Chem Neurosci 2021; 12 (03) 391-418
- 15 Vishwas S, Gulati M, Kapoor B. et al. Expanding the arsenal against Huntington's disease-herbal drugs and their nanoformulations. Curr Neuropharmacol 2021; 19 (07) 957-989
- 16 Gregory J, Vengalasetti YV, Bredesen DE, Rao RV. Neuroprotective herbs for the management of Alzheimer's disease. Biomolecules 2021; 11 (04) 543
- 17 Mehla J, Gupta P, Pahuja M, Diwan D, Diksha D. Indian medicinal herbs and formulations for Alzheimer's disease, from traditional knowledge to scientific assessment. Brain Sci 2020; 10 (12) 964
- 18 Mojaverrostami S, Bojnordi MN, Ghasemi-Kasman M, Ebrahimzadeh MA, Hamidabadi HG. A review of herbal therapy in multiple sclerosis. Adv Pharm Bull 2018; 8 (04) 575-590
- 19 Costantini E, Masciarelli E, Casorri L, Di Luigi M, Reale M. Medicinal herbs and multiple sclerosis: overview on the hard balance between new therapeutic strategy and occupational health risk. Front Cell Neurosci 2022; 16: 985943
- 20 Trogrlić I, Trogrlić D, Trogrlić D, Trogrlić AK. Treatment of glioblastoma with herbal medicines. World J Surg Oncol 2018; 16 (01) 28
- 21 Mian SY, Nambiar A, Kaliaperumal C. Phytotherapy for the treatment of glioblastoma: a review. Front Surg 2022; 9: 844993
- 22 Aghdash SN. Herbal medicine in the treatment of epilepsy. Curr Drug Targets 2021; 22 (03) 356-367
- 23 Liu W, Ge T, Pan Z, Leng Y, Lv J, Li B. The effects of herbal medicine on epilepsy. Oncotarget 2017; 8 (29) 48385-48397
- 24 Levin M. Herbal treatment of headache. Headache 2012; 52 (2, Suppl 2): 76-80
- 25 Lyu S, Zhang CS, Guo X. et al. Efficacy and safety of oral Chinese herbal medicine for migraine: a systematic review and meta-analyses using robust variance estimation model. Front Neurol 2022; 13: 889336
- 26 Priya CS, Venkataswamy M, Harshini G, Pravalika P, Mandadi S, Bandla J. Medicinal plants used for the treatment of bacterial meningitis. Res J Pharm Dos Forms Technol 2019; 11: 239-244
- 27 Ushir K, Rishipathak D, Bhosale P, Raut M. Ayurvedic remedies of bacterial meningitis. Int J Pharm Sci 2021; 1: 12-20
- 28 Zhang W, Yan Y, Wu Y. et al. Medicinal herbs for the treatment of anxiety: a systematic review and network meta-analysis. Pharmacol Res 2022; 179: 106204
- 29 Liu L, Liu C, Wang Y, Wang P, Li Y, Li B. Herbal medicine for anxiety, depression and insomnia. Curr Neuropharmacol 2015; 13 (04) 481-493
- 30 Kenda M, Kočevar Glavač N, Nagy M, Sollner Dolenc M. Medicinal plants used for anxiety, depression, or stress treatment: an update. Molecules 2022; 27 (18) 6021
- 31 Parvez MK. Natural or plant products for the treatment of neurological disorders: current knowledge. Curr Drug Metab 2018; 19 (05) 424-428
- 32 Luthra R, Roy A. Role of medicinal plants against neurodegenerative diseases. Curr Pharm Biotechnol 2022; 23 (01) 123-139
- 33 Karim N, Abdelhalim H, Gavande N, Khan I, Khan H. Natural products as an emerging therapeutic alternative in the treatment of neurological disorders. Evid Based Complement Alternat Med 2018; 2018: 3056847
- 34 Iriti M, Vitalini S, Fico G, Faoro F. Neuroprotective herbs and foods from different traditional medicines and diets. Molecules 2010; 15 (05) 3517-3555
- 35 Safdari MR, Shakeri F, Mohammadi A. et al. Role of herbal medicines in the management of brain injury. Adv Exp Med Biol 2021; 1328: 287-305
- 36 Ghosh S, Singha PS, Ghosh D. Neuroprotective compounds from three common medicinal plants of West Bengal, India: a mini review. Explor Neurosci 2023; 2: 307-317
- 37 Wongkrajang Y, Kitphati W, Kongsaktrakoon B, Temsiririrkkul R. Potential risks and hazards from herbal uses. JAASP 2014; 3: 280-289
- 38 Ekor M. The growing use of herbal medicines: issues relating to adverse reactions and challenges in monitoring safety. Front Pharmacol 2014; 4: 177
- 39 Başaran N, Paslı D, Başaran AA. Unpredictable adverse effects of herbal products. Food Chem Toxicol 2022; 159: 112762
- 40 Ernst E. Serious psychiatric and neurological adverse effects of herbal medicines: a systematic review. Acta Psychiatr Scand 2003; 108 (02) 83-91
- 41 Kahraman C, Arituluk ZC, Cankaya IIT. The clinical importance of herb-drug interactions and toxicological risks of plants and herbal products. In: Medical Toxicology. London: IntechOpen; 2021
- 42 Wilson V, Maulik SK. Herb-drug interactions in neurological disorders: a critical appraisal. Curr Drug Metab 2018; 19 (05) 443-453
- 43 Opuni KFM, Kretchy JP, Agyabeng K. et al. Contamination of herbal medicinal products in low-and-middle-income countries: a systematic review. Heliyon 2023; 9 (09) e19370
- 44 Fatima N, Nayeem N. Toxic effects as a result of herbal medicine intake. In: Toxicology: New Aspects to This Scientific Conundrum. London: IntechOpen; 2016
- 45 Jităreanu A, Trifan A, Vieriu M, Caba I-C, Mârțu I, Agoroaei L. Current trends in toxicity assessment of herbal medicines: a narrative review. Processes (Basel) 2023; 11: 83
- 46 Posadzki P, Watson LK, Ernst E. Adverse effects of herbal medicines: an overview of systematic reviews. Clin Med (Lond) 2013; 13 (01) 7-12
- 47 Bhalla A, Pannu AK. Are ayurvedic medications store house of heavy metals?. Toxicol Res (Camb) 2022; 11 (01) 179-183
- 48 Bisht VK, Uniyal RC, Sharma SM. Assessment of heavy metal content in herbal raw materials traded in India. S Afr J Bot 2022; 148: 154-161
- 49 Williamson EM. Herbal neurotoxicity: an introduction to its occurrence and causes. In: Pelkonen O, Duez P, Vuorela P, Vuorela H. eds. Toxicology of Herbal Products. Cham: Springer; 2017
- 50 Bal-Price AK, Hogberg HT, Buzanska L, Lenas P, van Vliet E, Hartung T. In vitro developmental neurotoxicity (DNT) testing: relevant models and endpoints. Neurotoxicology 2010; 31 (05) 545-554
- 51 Sahu R, Gupta PK, Mishra A, Kumar A. Ayurveda and in silico approach: a challenging proficient confluence for better development of effective traditional medicine spotlighting network pharmacology. Chin J Integr Med 2023; 29 (05) 470-480
- 52 Durán-Iturbide NA, Díaz-Eufracio BI, Medina-Franco JL. In silico ADME/Tox profiling of natural products: a focus on BIOFACQUIM. ACS Omega 2020; 5 (26) 16076-16084
- 53 Neergheen-Bhujun VS. Underestimating the toxicological challenges associated with the use of herbal medicinal products in developing countries. BioMed Res Int 2013; 2013: 804086
- 54 Zhang J, Onakpoya IJ, Posadzki P, Eddouks M. The safety of herbal medicine: from prejudice to evidence. Evid Based Complement Alternat Med 2015; 2015: 316706
- 55 Wang H, Chen Y, Wang L, Liu Q, Yang S, Wang C. Advancing herbal medicine: enhancing product quality and safety through robust quality control practices. Front Pharmacol 2023; 14: 1265178
Address for correspondence
Publication History
Article published online:
01 August 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Pan SY, Litscher G, Gao SH. et al. Historical perspective of traditional indigenous medical practices: the current renaissance and conservation of herbal resources. Evid Based Complement Alternat Med 2014; 2014: 525340
- 2 Kurhekar JV. Ancient and modern practices in phytomedicine. In: Egbuna C, Prakash Mishra A, Goyal MG. eds. Preparation of Phytopharmaceuticals for the Management of Disorders. Cambridge, MA: Academic Press; 2021: 55-75
- 3 Pan SY, Pan S, Yu ZL. et al. New perspectives on innovative drug discovery: an overview. J Pharm Sci 2010; 13 (03) 450-471
- 4 Halder S, Anand U, Nandy S. et al. Herbal drugs and natural bioactive products as potential therapeutics: a review on pro-cognitives and brain boosters perspectives. Saudi Pharm J 2021; 29 (08) 879-907
- 5 Fan F, Lei M. Mechanisms underlying curcumin-induced neuroprotection in cerebral ischemia. Front Pharmacol 2022; 13: 893118
- 6 Feng Z, Sun Q, Chen W, Bai Y, Hu D, Xie X. The neuroprotective mechanisms of ginkgolides and bilobalide in cerebral ischemic injury: a literature review. Mol Med 2019; 25 (01) 57
- 7 Xue R, Gao S, Zhang Y. et al. A meta-analysis of resveratrol protects against cerebral ischemia/reperfusion injury: evidence from rats studies and insight into molecular mechanisms. Front Pharmacol 2022; 13: 988836
- 8 Keshavarzi Z, Shakeri F, Barreto GE, Bibak B, Sathyapalan T, Sahebkar A. Medicinal plants in traumatic brain injury: neuroprotective mechanisms revisited. Biofactors 2019; 45 (04) 517-535
- 9 Lee B, Leem J, Kim H, Jo HG, Kwon CY. Herbal medicine for traumatic brain injury: a systematic review and meta-analysis of randomized controlled trials and limitations. Front Neurol 2020; 11: 772
- 10 Wakade C, King MD, Laird MD, Alleyne Jr CH, Dhandapani KM. Curcumin attenuates vascular inflammation and cerebral vasospasm after subarachnoid hemorrhage in mice. Antioxid Redox Signal 2009; 11 (01) 35-45
- 11 Tan J, Song R, Luo S. et al. Efficacy of resveratrol in experimental subarachnoid hemorrhage animal models: a stratified meta-analysis. Front Pharmacol 2022; 13: 905208
- 12 Amro MS, Teoh SL, Norzana AG, Srijit D. The potential role of herbal products in the treatment of Parkinson's disease. Clin Ter 2018; 169 (01) e23-e33
- 13 Yin R, Xue J, Tan Y. et al. The positive role and mechanism of herbal medicine in Parkinson's disease. Oxid Med Cell Longev 2021; 2021: 9923331
- 14 Lum PT, Sekar M, Gan SH, Bonam SR, Shaikh MF. Protective effect of natural products against Huntington's disease: an overview of scientific evidence and understanding their mechanism of action. ACS Chem Neurosci 2021; 12 (03) 391-418
- 15 Vishwas S, Gulati M, Kapoor B. et al. Expanding the arsenal against Huntington's disease-herbal drugs and their nanoformulations. Curr Neuropharmacol 2021; 19 (07) 957-989
- 16 Gregory J, Vengalasetti YV, Bredesen DE, Rao RV. Neuroprotective herbs for the management of Alzheimer's disease. Biomolecules 2021; 11 (04) 543
- 17 Mehla J, Gupta P, Pahuja M, Diwan D, Diksha D. Indian medicinal herbs and formulations for Alzheimer's disease, from traditional knowledge to scientific assessment. Brain Sci 2020; 10 (12) 964
- 18 Mojaverrostami S, Bojnordi MN, Ghasemi-Kasman M, Ebrahimzadeh MA, Hamidabadi HG. A review of herbal therapy in multiple sclerosis. Adv Pharm Bull 2018; 8 (04) 575-590
- 19 Costantini E, Masciarelli E, Casorri L, Di Luigi M, Reale M. Medicinal herbs and multiple sclerosis: overview on the hard balance between new therapeutic strategy and occupational health risk. Front Cell Neurosci 2022; 16: 985943
- 20 Trogrlić I, Trogrlić D, Trogrlić D, Trogrlić AK. Treatment of glioblastoma with herbal medicines. World J Surg Oncol 2018; 16 (01) 28
- 21 Mian SY, Nambiar A, Kaliaperumal C. Phytotherapy for the treatment of glioblastoma: a review. Front Surg 2022; 9: 844993
- 22 Aghdash SN. Herbal medicine in the treatment of epilepsy. Curr Drug Targets 2021; 22 (03) 356-367
- 23 Liu W, Ge T, Pan Z, Leng Y, Lv J, Li B. The effects of herbal medicine on epilepsy. Oncotarget 2017; 8 (29) 48385-48397
- 24 Levin M. Herbal treatment of headache. Headache 2012; 52 (2, Suppl 2): 76-80
- 25 Lyu S, Zhang CS, Guo X. et al. Efficacy and safety of oral Chinese herbal medicine for migraine: a systematic review and meta-analyses using robust variance estimation model. Front Neurol 2022; 13: 889336
- 26 Priya CS, Venkataswamy M, Harshini G, Pravalika P, Mandadi S, Bandla J. Medicinal plants used for the treatment of bacterial meningitis. Res J Pharm Dos Forms Technol 2019; 11: 239-244
- 27 Ushir K, Rishipathak D, Bhosale P, Raut M. Ayurvedic remedies of bacterial meningitis. Int J Pharm Sci 2021; 1: 12-20
- 28 Zhang W, Yan Y, Wu Y. et al. Medicinal herbs for the treatment of anxiety: a systematic review and network meta-analysis. Pharmacol Res 2022; 179: 106204
- 29 Liu L, Liu C, Wang Y, Wang P, Li Y, Li B. Herbal medicine for anxiety, depression and insomnia. Curr Neuropharmacol 2015; 13 (04) 481-493
- 30 Kenda M, Kočevar Glavač N, Nagy M, Sollner Dolenc M. Medicinal plants used for anxiety, depression, or stress treatment: an update. Molecules 2022; 27 (18) 6021
- 31 Parvez MK. Natural or plant products for the treatment of neurological disorders: current knowledge. Curr Drug Metab 2018; 19 (05) 424-428
- 32 Luthra R, Roy A. Role of medicinal plants against neurodegenerative diseases. Curr Pharm Biotechnol 2022; 23 (01) 123-139
- 33 Karim N, Abdelhalim H, Gavande N, Khan I, Khan H. Natural products as an emerging therapeutic alternative in the treatment of neurological disorders. Evid Based Complement Alternat Med 2018; 2018: 3056847
- 34 Iriti M, Vitalini S, Fico G, Faoro F. Neuroprotective herbs and foods from different traditional medicines and diets. Molecules 2010; 15 (05) 3517-3555
- 35 Safdari MR, Shakeri F, Mohammadi A. et al. Role of herbal medicines in the management of brain injury. Adv Exp Med Biol 2021; 1328: 287-305
- 36 Ghosh S, Singha PS, Ghosh D. Neuroprotective compounds from three common medicinal plants of West Bengal, India: a mini review. Explor Neurosci 2023; 2: 307-317
- 37 Wongkrajang Y, Kitphati W, Kongsaktrakoon B, Temsiririrkkul R. Potential risks and hazards from herbal uses. JAASP 2014; 3: 280-289
- 38 Ekor M. The growing use of herbal medicines: issues relating to adverse reactions and challenges in monitoring safety. Front Pharmacol 2014; 4: 177
- 39 Başaran N, Paslı D, Başaran AA. Unpredictable adverse effects of herbal products. Food Chem Toxicol 2022; 159: 112762
- 40 Ernst E. Serious psychiatric and neurological adverse effects of herbal medicines: a systematic review. Acta Psychiatr Scand 2003; 108 (02) 83-91
- 41 Kahraman C, Arituluk ZC, Cankaya IIT. The clinical importance of herb-drug interactions and toxicological risks of plants and herbal products. In: Medical Toxicology. London: IntechOpen; 2021
- 42 Wilson V, Maulik SK. Herb-drug interactions in neurological disorders: a critical appraisal. Curr Drug Metab 2018; 19 (05) 443-453
- 43 Opuni KFM, Kretchy JP, Agyabeng K. et al. Contamination of herbal medicinal products in low-and-middle-income countries: a systematic review. Heliyon 2023; 9 (09) e19370
- 44 Fatima N, Nayeem N. Toxic effects as a result of herbal medicine intake. In: Toxicology: New Aspects to This Scientific Conundrum. London: IntechOpen; 2016
- 45 Jităreanu A, Trifan A, Vieriu M, Caba I-C, Mârțu I, Agoroaei L. Current trends in toxicity assessment of herbal medicines: a narrative review. Processes (Basel) 2023; 11: 83
- 46 Posadzki P, Watson LK, Ernst E. Adverse effects of herbal medicines: an overview of systematic reviews. Clin Med (Lond) 2013; 13 (01) 7-12
- 47 Bhalla A, Pannu AK. Are ayurvedic medications store house of heavy metals?. Toxicol Res (Camb) 2022; 11 (01) 179-183
- 48 Bisht VK, Uniyal RC, Sharma SM. Assessment of heavy metal content in herbal raw materials traded in India. S Afr J Bot 2022; 148: 154-161
- 49 Williamson EM. Herbal neurotoxicity: an introduction to its occurrence and causes. In: Pelkonen O, Duez P, Vuorela P, Vuorela H. eds. Toxicology of Herbal Products. Cham: Springer; 2017
- 50 Bal-Price AK, Hogberg HT, Buzanska L, Lenas P, van Vliet E, Hartung T. In vitro developmental neurotoxicity (DNT) testing: relevant models and endpoints. Neurotoxicology 2010; 31 (05) 545-554
- 51 Sahu R, Gupta PK, Mishra A, Kumar A. Ayurveda and in silico approach: a challenging proficient confluence for better development of effective traditional medicine spotlighting network pharmacology. Chin J Integr Med 2023; 29 (05) 470-480
- 52 Durán-Iturbide NA, Díaz-Eufracio BI, Medina-Franco JL. In silico ADME/Tox profiling of natural products: a focus on BIOFACQUIM. ACS Omega 2020; 5 (26) 16076-16084
- 53 Neergheen-Bhujun VS. Underestimating the toxicological challenges associated with the use of herbal medicinal products in developing countries. BioMed Res Int 2013; 2013: 804086
- 54 Zhang J, Onakpoya IJ, Posadzki P, Eddouks M. The safety of herbal medicine: from prejudice to evidence. Evid Based Complement Alternat Med 2015; 2015: 316706
- 55 Wang H, Chen Y, Wang L, Liu Q, Yang S, Wang C. Advancing herbal medicine: enhancing product quality and safety through robust quality control practices. Front Pharmacol 2023; 14: 1265178