

RSS-Feed abonnieren
DOI: 10.1055/s-0045-1812015
A Novel Cut-out Syringe Scalp Retractor for Endoscopic Strip Craniectomy for Craniosynostosis—A Cost-effective and Durable Alternative
Autoren

Abstract
Aim
Unilateral coronal craniosynostosis is the second most common subtype of nonsyndromic craniosynostosis. Endoscopic repair requires a scalp and dural retractor for adequate visualization and performing strip craniectomy. We describe the application of a novel cut-out syringe scalp retractor for endoscopic repair of unilateral coronal craniosynostosis.
Background
A 3-month-old female child presented with a progressive abnormal head shape. Three-dimensional reconstruction of brain CT showed a right fused coronal suture with ipsilateral temporal and contralateral frontal prominence. A diagnosis of unilateral coronal synostosis was made. The patient underwent endoscopic strip craniectomy using a novel cut-out syringe scalp retractor. The craniectomy extended from the right squamosal suture to the anterior fontanelle. The postoperative recovery was uneventful.
Discussion and Conclusion
The main aim of endoscopic surgery is to swiftly address the progression of calvarial and facial dysmorphism. The timings of endoscopic repair are crucial and usually performed before 3 months of age. It has a distinct advantage over open repair owing to shorter hospital stays, less bleeding, lower operative times, comparable aesthetic outcomes, and being minimally invasive. For endoscopic repair, various retractors have been described in the literature but these retractors are difficult to procure in resource-constrained setup. We advocate the usage of a cost-effective, durable, reusable, and malleable scalp retractor whose cost is nominal. It can be safely sterilized or can be newly made for every case. We found this retractor to be extremely useful in the case of endoscopic strip craniectomy.
Keywords
coronal craniosynostosis - endoscopic repair - syringe retractor - novel technique - strip craniectomyIntroduction
Craniosynostosis is a rare condition affecting 1 in 2,000 to 2,500 live births.[1] It involves premature fusion of one or more cranial sutures, which results in uneven growth at the other suture sites and abnormal enlargement of the head. Nearly 85% of craniosynostosis patients are nonsyndromic due to underlying de novo genetic mutation or single nucleotide alteration.[2] [3] The remainder are syndromic, which include but are not limited to Apert, Down's, Muenke, Crouzon, and Pfeiffer etc. The unilateral coronal synostosis (anterior plagiocephaly) is the second most common subtype after sagittal synostosis. It accounts for almost one-third of cases of nonsyndromic craniosynostosis. The incidence of unilateral coronal craniosynostosis is 1 in 10,000 live births and it is more common in females.[4] [5] The most common mutations involved in nonsyndromic unilateral coronal craniosynostosis are FGFR3, TWIST1, and TCF12.[2]
The primary treatment for craniosynostosis involves surgical intervention. There are multiple surgical options available, ranging from complex cranial vault reconstruction to minimally invasive endoscopic suturectomy/strip craniectomy. The principle of endoscopic surgery relies on the undercutting of the fused suture followed by helmet therapy to allow remodeling over time. It is being readily picked up by surgeons across the world owing to shorter hospital stays, minimal blood loss, less scarring and blood loss, better aesthetics, and being minimally invasive.
For endoscopic repair, although various retractors have been described in the literature such as the J&B Dural-Scalp retractor,[6] Lighted retractor[7] etc., herein we describe endoscopic repair of unilateral coronal craniosynostosis using a novel cut-out syringe scalp retractor. It is durable, cost-effective, and readily available in resource-constrained setups.
Case Discussion
A 3-month-old female child came with complaints of abnormal head shape, which was gradually progressing with time ([Fig. 1]). Clinical, neurological, and fundus examinations were within normal limits. Ultrasound of abdomen, echocardiography, and ophthalmological examination were normal. There were no clinical signs of intracranial hypertension and no evidence of hydrocephalus in the CT of brain. The brain parenchyma was normal.

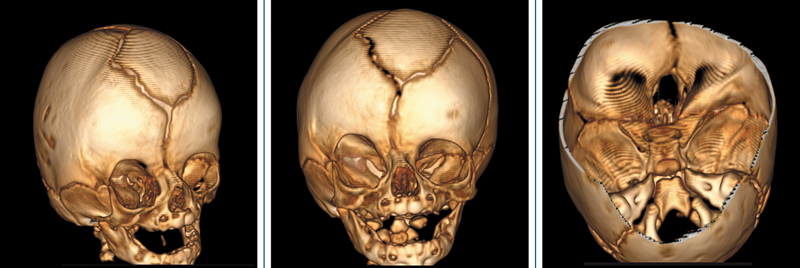
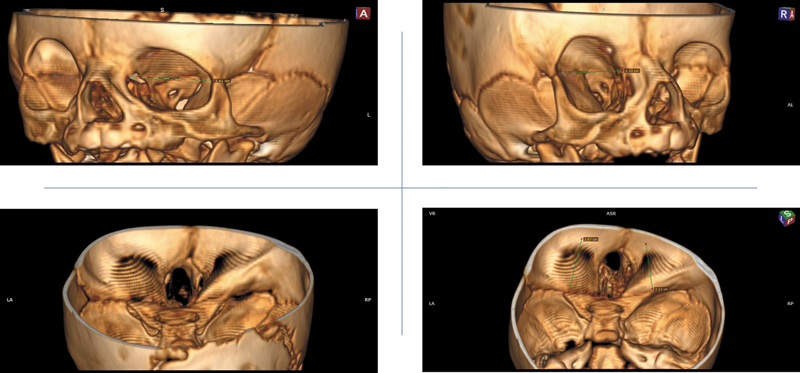
Three-dimensional reconstruction of brain CT bone window showed flattening of the right frontal bone at the site of fused coronal suture with ipsilateral enlargement of the right temporal bone and contralateral bossing of the left frontal bone ([Fig. 2]). In addition, there is an elevation of the right greater wing of the sphenoid bone and foreshortened anterior skull base ([Fig. 3]). A diagnosis of right unilateral coronal craniosynostosis was made. The patient was planned for endoscopic strip craniectomy followed by 12 months of helmet therapy.
The patient was placed in the supine position and a curvilinear incision was made overlying the fused suture at the level of stephanion ([Fig. 4]). After opening the galea, a soft, malleable, cut-out syringe scalp retractor was placed beneath the galea. A subgaleal plane is created with the help of the retractor. Subsequently, a burr hole is made with the help of a cutting drill (40 mm), and the dura is separated from the underlying fused suture with the help of a Penfield dissector. The burr hole osteotomy is then enlarged with the help of a Kerrison rongeur. Any bleeding from the diploe is controlled using bone wax as illustrated ([Fig. 5]).


With the self-retaining, malleable cut-out syringe scalp retractor beneath the galea aponeurotica and the Penfield dissector separating the dura from the fused suture site, a diamond drill is introduced as shown in the pictorial illustration ([Fig. 6]). The osteotomy is enlarged medially to reach the anterior fontanelle and laterally up to the squamosal suture using the diamond drill. The hemostasis is achieved using bone wax from the bony diploe. The postoperative scan shows adequate suturectomy. At 12 months, after helmet therapy, slight prominence was observed in the right frontal area along with rounding of the occipital bone below the vertex, and bilateral symmetry of greater wing of sphenoid bone was noted ([Fig. 7]).


Discussion
Cranial sutures are fibrous joints that serve as growth plates and as a site of osteogenesis.[8] [9] The growth of the cranial vault is genetically regulated and any disturbance in these pathways leads to premature fusion of these fibrous joints.[8] Recent consensus demonstrates that fusion of the fibrous joints at the cranial vault is pathognomonic for craniosynostosis.[10] The diagnosis is by clinical observation. Radiological imaging (skull X-ray, three-dimensional CT reconstruction) is essential for surgical planning, as an adjunct when diagnosis is doubtful, and as a baseline reference for future evaluation.[11]
In cases of unilateral coronal craniosynostosis, there is flattening at the site of fused joints, ipsilateral bulging of the squamosal temporal bone, and prominence of the contralateral frontal bone ([Fig. 2]). The elevation of the ipsilateral greater wing of the sphenoid along with the reduced anteroposterior dimension of the anterior cranial fossa is considered pathognomonic for unilateral coronal craniosynostosis. Our case exhibits similar findings (as shown in [Fig. 3]). The treatment for craniosynostosis remains surgical. The surgical armamentarium includes distraction osteogenesis, fronto-orbital advancement (FOA), strip craniectomy, and endoscopic suturectomy. Distraction osteogenesis has its disadvantages, including multiple revision surgeries, the risk of intracranial migration of metallic implants, incomplete remodeling of the cranial vault, and surgical site infections, which add to surgical morbidity.[12] Reconstruction of the cranial vault involves complex craniofacial alignment that is time-consuming and associated with significant blood loss and longer postoperative stays.
Owing to these limitations, there was a preference toward less invasive procedures. The concept of strip craniectomies was first described in 1890.[13] However, the endoscopic strip craniectomies were first introduced in late 1900 by Vicari, and Jimenez and Barone.[14] [15] For endoscopic craniosynostosis repair, it is advisable to perform strip craniectomy before 3 months of age.[14] The rapid brain growth thereafter corrects the pre-surgical calvarial deformities after the removal of the fused fibrous joints. The postoperative helmet therapy ensures adequate remodeling and correction of the skull deformity over time.
The main aim of endoscopic surgery is to swiftly address the progression of calvarial and facial dysmorphism. It is imperative to ensure that the cranial base sutures remain unaffected before considering endoscopic repair for a patient.[16] The width of strip craniectomy for coronal craniosynostosis should be at least 1 cm. Endoscopic repair is gaining popularity among neurosurgeons and the parents owing to shorter hospital stays, early recovery, less scarring and blood loss, and being minimally invasive. A systematic review and meta-analysis have confirmed these findings in cases with sagittal and non-sagittal synostosis.[17] [18] The endoscopic repair offers equivocal/comparable outcomes with respect to cranial vault reconstruction, which has been validated by multiple studies.[19] [20] [21] [22] It is more cost-effective as compared to cranial vault remodeling.[23] [24] [25]
The endoscopic strip craniectomy does not require any special instruments for the procedure. The standard endoscopic trolley comprises of zero-degree rod-lens scope, a camera unit, a cold light source, and a high-definition monitor, which are available at the majority of the institutes performing routine cranial and spinal neurosurgery cases. For craniosynostosis cases, there are specifically designed retractors, viz, J&B Scalp-Dural retractor,[6] lighted speculum[7] etc. However, procurement of these could be difficult in a resource-constrained setup. We advocate the use of a cost-effective, durable, reusable, and malleable scalp retractor whose cost is one-fifth of 1 US dollar. The retractor is made from a 10-cc to 20-cc syringe and features a semi-circular plastic sheet with thread holes for easy removal post-surgery. The device can be sterilized using plasma sterilization or freshly made for each procedure, ensuring sterility. We found this scalp retractor to be extremely useful in the case of endoscopic strip craniectomy ([Fig. 5]). After initial incision and dissection, the retractor can be inserted into the subgaleal plane and further dissection can be done with the help of this novel retractor. The shape of the scalp retractor conforms to the galea, preventing the blood from seeping in from superior and lateral direction. Hence, it helps in maintaining a bloodless surgical field, which aids in appropriate visualization using an endoscope. The usage of this disposable self-retaining scalp retractor is extremely cost-effective and has not been described in the literature previously. The novel retractor is designed to improve surgical precision, visualization, and adaptability, while being affordable, disposable, and widely available, particularly in resource-constrained settings.
Although endoscopic surgery has its benefits, few studies have doubted the efficacy of this procedure. The reasons cited include a lack of adequate skull molding in the follow-up period, failure to achieve hemostasis far lateral to the strip craniectomy site, and comparable vault expansion to open surgery.[18] [20] [26] In addition, more favorable neurological outcomes have been reported for whole vault cranioplasty when performed before 6 months of age as compared to the endoscopic/open strip craniectomy.[27] However, we believe that endoscopic surgery since its inception in the late 1900s has evolved significantly and more neurosurgeons are adopting endoscopic repair. Future prospective studies will better elucidate the impact of endoscopic repair on cosmetic outcomes.
Conclusion
Endoscopic strip craniectomy is safe, causes less scarring and blood loss, is associated with fewer complications, and recovery is swift. The long-term outcomes of endoscopic repair are comparable to the open cranial vault reconstruction in the appropriate patient population. Our novel cut-out syringe scalp retractor should be considered for endoscopic repair cases in resource-constrained setups, particularly in developing countries.
Conflict of Interest
None declared.
Acknowledgements
Dr. Sonia Baral for contributing toward the artwork. Dr. Abhishek Shetty and Dr. Kaustav Saha for contributing toward the manuscript and collecting the patient data.
Authors' Contributions
A.S. and A.M. contributed to the conception and design of the work. A.M., H.P., and R.C. were responsible for data collection, while R.M., H.P., and R.C. carried out data editing and analysis. H.P., A.M., and R.C. drafted the article, and A.S. and R.M. performed the critical revision. The final version was reviewed by A.S.
Patient's Consent
Full and detailed consent from the patient/guardian has been taken. The patient's identity has been adequately anonymized. If anything related to the patient's identity is shown, adequate consent has been taken from the patient/relative/guardian. The journal will not be responsible for any medico-legal issues arising out of issues related to the patient's identity or any other issues arising from the public display of the images/video.
-
References
- 1 Poot M. Structural genome variations related to craniosynostosis. Mol Syndromol 2019; 10 (1-2): 24-39
- 2 Timberlake AT, Persing JA. Genetics of nonsyndromic craniosynostosis. Plast Reconstr Surg 2018; 141 (06) 1508-1516
- 3 Cohen MM, MacLean RE. eds Craniosynostosis: Diagnosis, Evaluation, and Management. 2nd ed.. New York: Oxford University Press; 2000
- 4 Boyadjiev SA. International Craniosynostosis Consortium. Genetic analysis of non-syndromic craniosynostosis. Orthod Craniofac Res 2007; 10 (03) 129-137
- 5 Kalantar-Hormozi H, Abbaszadeh-Kasbi A, Sharifi G, Davai NR, Kalantar-Hormozi A. Incidence of familial craniosynostosis among patients with nonsyndromic craniosynostosis. J Craniofac Surg 2019; 30 (06) e514-e517
- 6 Jimenez DF, Barone CM. Minimally invasive craniosynostosis Surgery. In: Pediatric Neurosurgery: Tricks of the Trade. Stuttgart: Thieme; 2016: 151-157
- 7 Hersh DS, Lambert WA, Bookland MJ, Martin JE. Minimally invasive strip craniectomy for metopic craniosynostosis using a lighted retractor. Neurosurg Focus Video 2021; 4 (02) V5
- 8 Lenton KA, Nacamuli RP, Wan DC, Helms JA, Longaker MT. Cranial suture biology. In: Current Topics in Developmental Biology. Elsevier; 2005: 287-328
- 9 Senarath-Yapa K, Chung MT, McArdle A. et al. Craniosynostosis: molecular pathways and future pharmacologic therapy. Organogenesis 2012; 8 (04) 103-113
- 10 Delashaw JB, Persing JA, Broaddus WC, Jane JA. Cranial vault growth in craniosynostosis. J Neurosurg 1989; 70 (02) 159-165
- 11 Fearon JA, Singh DJ, Beals SP, Yu JC. The diagnosis and treatment of single-sutural synostoses: are computed tomographic scans necessary?. Plast Reconstr Surg 2007; 120 (05) 1327-1331
- 12 Taylor JA, Derderian CA, Bartlett SP, Fiadjoe JE, Sussman EM, Stricker PA. Perioperative morbidity in posterior cranial vault expansion: distraction osteogenesis versus conventional osteotomy. Plast Reconstr Surg 2012; 129 (04) 674e-680e
- 13 Lannelongue M. De la craniectomie dans la microcephalie. C R Acad Sci 1890; 110: 1382-1385
- 14 Jimenez DF, Barone CM. Endoscopic craniectomy for early surgical correction of sagittal craniosynostosis. J Neurosurg 1998; 88 (01) 77-81
- 15 Vicari F. . Endoscopic Correction of Sagittal Synostosis. Am Soc Plast Reconstr Surg Presymposium San Diego CA; 1994
- 16 Jimenez DF, Barone CM. Endoscopic treatment of craniosynostosis. In: Youmans & Winn Neurological Surgery Elsevier; 2023. 1691. e1-e13
- 17 Yan H, Abel TJ, Alotaibi NM. et al. A systematic review and meta-analysis of endoscopic versus open treatment of craniosynostosis. Part 1: the sagittal suture. J Neurosurg Pediatr 2018; 22 (04) 352-360
- 18 Yan H, Abel TJ, Alotaibi NM. et al. A systematic review of endoscopic versus open treatment of craniosynostosis. Part 2: the nonsagittal single sutures. J Neurosurg Pediatr 2018; 22 (04) 361-368
- 19 Masserano B, Woo AS, Skolnick GB. et al. The temporal region in unilateral coronal craniosynostosis: fronto-orbital advancement versus endoscopy-assisted strip craniectomy. Cleft Palate Craniofac J 2018; 55 (03) 423-429
- 20 Isaac KV, MacKinnon S, Dagi LR, Rogers GF, Meara JG, Proctor MR. Nonsyndromic unilateral coronal synostosis: a comparison of fronto-orbital advancement and endoscopic suturectomy. Plast Reconstr Surg 2019; 143 (03) 838-848
- 21 Varagur K, Skolnick GB, Naidoo SD, Smyth MD, Patel KB. School-age outcomes in patients with unilateral coronal synostosis: comparison of fronto-orbital advancement and endoscopic strip craniectomy. J Neurosurg Pediatr 2022; 29 (05) 560-567
- 22 Williams CT, Segar DJ, Naidoo SD. et al. Evaluation of endoscopic strip craniectomy and orthotic therapy for bilateral coronal craniosynostosis. J Craniofac Surg 2019; 30 (02) 453-457
- 23 Garber ST, Karsy M, Kestle JRW, Siddiqi F, Spanos SP, Riva-Cambrin J. Comparing outcomes and cost of 3 surgical treatments for sagittal synostosis: a retrospective study including procedure-related cost analysis. Neurosurgery 2017; 81 (04) 680-687
- 24 Liles C, Dallas J, Hale AT. et al. The economic impact of open versus endoscope-assisted craniosynostosis surgery. J Neurosurg Pediatr 2019; 24 (02) 145-152
- 25 Stanbouly D, Ascherman JA, Chuang S-K. Open repair versus closed repair: a cost-analysis of the two surgical approaches for the treatment of craniosynostoses. J Oral Maxillofac Surg 2022; 80 (03) 465-470
- 26 Proctor MR. Endoscopic cranial suture release for the treatment of craniosynostosis—is it the future?. J Craniofac Surg 2012; 23 (01) 225-228
- 27 Hashim PW, Patel A, Yang JF. et al. The effects of whole-vault cranioplasty versus strip craniectomy on long-term neuropsychological outcomes in sagittal craniosynostosis. Plast Reconstr Surg 2014; 134 (03) 491-501
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
25. September 2025
© 2025. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Poot M. Structural genome variations related to craniosynostosis. Mol Syndromol 2019; 10 (1-2): 24-39
- 2 Timberlake AT, Persing JA. Genetics of nonsyndromic craniosynostosis. Plast Reconstr Surg 2018; 141 (06) 1508-1516
- 3 Cohen MM, MacLean RE. eds Craniosynostosis: Diagnosis, Evaluation, and Management. 2nd ed.. New York: Oxford University Press; 2000
- 4 Boyadjiev SA. International Craniosynostosis Consortium. Genetic analysis of non-syndromic craniosynostosis. Orthod Craniofac Res 2007; 10 (03) 129-137
- 5 Kalantar-Hormozi H, Abbaszadeh-Kasbi A, Sharifi G, Davai NR, Kalantar-Hormozi A. Incidence of familial craniosynostosis among patients with nonsyndromic craniosynostosis. J Craniofac Surg 2019; 30 (06) e514-e517
- 6 Jimenez DF, Barone CM. Minimally invasive craniosynostosis Surgery. In: Pediatric Neurosurgery: Tricks of the Trade. Stuttgart: Thieme; 2016: 151-157
- 7 Hersh DS, Lambert WA, Bookland MJ, Martin JE. Minimally invasive strip craniectomy for metopic craniosynostosis using a lighted retractor. Neurosurg Focus Video 2021; 4 (02) V5
- 8 Lenton KA, Nacamuli RP, Wan DC, Helms JA, Longaker MT. Cranial suture biology. In: Current Topics in Developmental Biology. Elsevier; 2005: 287-328
- 9 Senarath-Yapa K, Chung MT, McArdle A. et al. Craniosynostosis: molecular pathways and future pharmacologic therapy. Organogenesis 2012; 8 (04) 103-113
- 10 Delashaw JB, Persing JA, Broaddus WC, Jane JA. Cranial vault growth in craniosynostosis. J Neurosurg 1989; 70 (02) 159-165
- 11 Fearon JA, Singh DJ, Beals SP, Yu JC. The diagnosis and treatment of single-sutural synostoses: are computed tomographic scans necessary?. Plast Reconstr Surg 2007; 120 (05) 1327-1331
- 12 Taylor JA, Derderian CA, Bartlett SP, Fiadjoe JE, Sussman EM, Stricker PA. Perioperative morbidity in posterior cranial vault expansion: distraction osteogenesis versus conventional osteotomy. Plast Reconstr Surg 2012; 129 (04) 674e-680e
- 13 Lannelongue M. De la craniectomie dans la microcephalie. C R Acad Sci 1890; 110: 1382-1385
- 14 Jimenez DF, Barone CM. Endoscopic craniectomy for early surgical correction of sagittal craniosynostosis. J Neurosurg 1998; 88 (01) 77-81
- 15 Vicari F. . Endoscopic Correction of Sagittal Synostosis. Am Soc Plast Reconstr Surg Presymposium San Diego CA; 1994
- 16 Jimenez DF, Barone CM. Endoscopic treatment of craniosynostosis. In: Youmans & Winn Neurological Surgery Elsevier; 2023. 1691. e1-e13
- 17 Yan H, Abel TJ, Alotaibi NM. et al. A systematic review and meta-analysis of endoscopic versus open treatment of craniosynostosis. Part 1: the sagittal suture. J Neurosurg Pediatr 2018; 22 (04) 352-360
- 18 Yan H, Abel TJ, Alotaibi NM. et al. A systematic review of endoscopic versus open treatment of craniosynostosis. Part 2: the nonsagittal single sutures. J Neurosurg Pediatr 2018; 22 (04) 361-368
- 19 Masserano B, Woo AS, Skolnick GB. et al. The temporal region in unilateral coronal craniosynostosis: fronto-orbital advancement versus endoscopy-assisted strip craniectomy. Cleft Palate Craniofac J 2018; 55 (03) 423-429
- 20 Isaac KV, MacKinnon S, Dagi LR, Rogers GF, Meara JG, Proctor MR. Nonsyndromic unilateral coronal synostosis: a comparison of fronto-orbital advancement and endoscopic suturectomy. Plast Reconstr Surg 2019; 143 (03) 838-848
- 21 Varagur K, Skolnick GB, Naidoo SD, Smyth MD, Patel KB. School-age outcomes in patients with unilateral coronal synostosis: comparison of fronto-orbital advancement and endoscopic strip craniectomy. J Neurosurg Pediatr 2022; 29 (05) 560-567
- 22 Williams CT, Segar DJ, Naidoo SD. et al. Evaluation of endoscopic strip craniectomy and orthotic therapy for bilateral coronal craniosynostosis. J Craniofac Surg 2019; 30 (02) 453-457
- 23 Garber ST, Karsy M, Kestle JRW, Siddiqi F, Spanos SP, Riva-Cambrin J. Comparing outcomes and cost of 3 surgical treatments for sagittal synostosis: a retrospective study including procedure-related cost analysis. Neurosurgery 2017; 81 (04) 680-687
- 24 Liles C, Dallas J, Hale AT. et al. The economic impact of open versus endoscope-assisted craniosynostosis surgery. J Neurosurg Pediatr 2019; 24 (02) 145-152
- 25 Stanbouly D, Ascherman JA, Chuang S-K. Open repair versus closed repair: a cost-analysis of the two surgical approaches for the treatment of craniosynostoses. J Oral Maxillofac Surg 2022; 80 (03) 465-470
- 26 Proctor MR. Endoscopic cranial suture release for the treatment of craniosynostosis—is it the future?. J Craniofac Surg 2012; 23 (01) 225-228
- 27 Hashim PW, Patel A, Yang JF. et al. The effects of whole-vault cranioplasty versus strip craniectomy on long-term neuropsychological outcomes in sagittal craniosynostosis. Plast Reconstr Surg 2014; 134 (03) 491-501