Subscribe to RSS
DOI: 10.1055/s-0045-1812501
Capitellum Fractures: Diagnosis and Treatment Options
Article in several languages: español | EnglishAuthors

Abstract
The capitellum fractures are a rare and challenging group of distal humerus fractures with diverse patterns, going from simple uniplanar fractures to complex, comminuted, and ligament-involving fractures. Proper identification and management are crucial to prevent complications such as elbow stiffness, pain, and post-traumatic arthritis. This review provides a comprehensive overview of current approaches to managing these fractures, emphasizing anatomical considerations, epidemiology, clinical assessment, classification systems, and surgical techniques. This article further highlights the effectiveness and limitations of fixation methods, including Kirschner wires, screws, plates, arthroscopic-assisted reduction, and elbow arthroplasty according to the fracture pattern. Despite a better understanding of the fracture pattern, complications such as avascular necrosis and osteoarthritis continue to cause significant challenges, particularly in complex fracture configurations. This review aims to enhance the understanding of treatment strategies to improve the management and outcomes of this uncommon fracture.
Introduction
Capitellum fractures are a unique and challenging group of distal humerus fractures.[1] These injuries span a spectrum of severity, ranging from simple, uniplanar, noncomminuted fractures to complex, comminuted, multiplanar fractures with associated ligament involvement.[2] Proper identification of these fractures and pattern-specific management are critical to prevent potential complications and sequelae such as stiffness, pain, and elbow osteoarthritis.[1] [3] [4]
This review provides a comprehensive overview of current approaches to the surgical treatment of these fractures, emphasizing anatomical considerations, epidemiology, clinical evaluation, classification systems, and various surgical techniques.
Relevant Anatomy
The elbow is composed of three main joints: the radiocapitellar, the ulnohumeral, and the proximal radioulnar. The humeral condyles have an anterior flexion of 30° in relation to the axis of the humerus, 6-8° of valgus inclination, and 5° of internal rotation in relation to the transepicondylar axis.[5] Lateral to the capitellum is the lateral epicondyle, into which the extensor-supinator muscle mass is inserted, as well as the insertion of the lateral ulnar and radial collateral ligaments, and the joint capsule.
The capitellum is supplied primarily by posterior vessels originating from the distal humeral artery. These vessels enter the posterior surface of the humerus and course toward the capitellum. Although there are secondary contributions from the musculature and joint capsule, the capitellum's blood supply is limited, making it highly susceptible to avascular necrosis secondary to trauma or the surgical procedure. For this reason, planning, soft tissue protection, and proper manipulation of the fragments are crucial to prevent complications.
Epidemiology
Capitellum fractures account for 6% of distal humerus fractures and 1% of all fractures around the elbow,[1] and are relatively uncommon. They can occur in adults or children, with a greater tendency toward comminuted fractures in older patients.[3] More than 80% of fractures occur in the female population, secondary to greater cubitus valgus, recurvatum, and osteoporosis.[4] [6] [7] Associated injuries, both bone and soft tissue, are common and should always be suspected. Among these, radial head fractures occur in approximately 25% of cases, while lateral collateral ligament (LCL) injuries are even more common, accounting for between 30 and 60%.[2] [4] [8] [9]
Clinical
Most capitellum fractures result from low-energy injuries, with varying degrees of elbow flexion.[4] There are two theories of mechanisms that could result in this type of fracture.[2] [10] In the first, the fracture can occur by a direct transfer of energy to the capitellum through an axial load on the radius.[2] The second could be after an elbow instability event with or without LCL injury, and both the trochlea and the capitellum could be fractured at the time of dislocation or reduction of the elbow.[2] These fracture mechanisms explain the high incidence of associated injuries that can be found with radial head fractures, LCL tears, and coronoid fractures.[10]
A thorough physical examination is necessary to rule out the most common associated injuries. Upon inspection, generalized edema at the elbow may be found, with ecchymosis on the lateral aspect. Palpation should be careful of bony prominences, with possible tenderness at the lateral or medial epicondyle or radial head, which should increase our suspicion of ligament injuries or radial head fractures. Range of motion or mobility blocks in elbow flexion and extension, and forearm pronation and supination relative to the contralateral side should be documented, if possible. Always examine the ipsilateral shoulder and wrist for concomitant injuries and perform a detailed distal neurological and vascular examination.
Radiography is the initial study of choice in these patients, including anteroposterior, lateral, and oblique projections of the elbow. These projections provide an initial approximation of the capitellum fracture, as well as other concomitant injuries. The lateral radiograph typically shows the "double arc sign," which represents the subchondral arc of the capitellum along with the lateral trochlea displaced superiorly, creating an overlap between the cortex of both bone structures.[11] Computed tomography (CT) is the option of choice to better assess fracture features, mediolateral extension, and comminution.[12] The use of CT has been shown to improve intra- and interobserver reliability in evaluating distal humerus fractures,[12] which may affect surgical planning and the final management strategy.
Classification
There are three classifications described in the literature for capitellum fractures. The first is the Bryan and Morrey classification,[1] which divides them into three types: Type 1 (Hahn-Steinthal) involves an isolated fracture of the capitellum with the subchondral bone attached; Type 2 (Kocher-Lorenz) primarily involves the articular cartilage over the capitellum; Type 3 (Brober-Morrey) is defined as comminuted capitellum fractures. A fourth type was added by McKee[11] and includes fractures that extend into the medial area of the trochlea.
Ring and Jupiter[13] propose another classification system: Type 1, with coronal feature shear fractures with a single articular fragment composed of the capitellum and lateral trochlea; Type 2, involving the lateral epicondyle; Type 3, characterized by impaction of the metaphyseal bone behind the capitellum on the distal and posterior aspect of the lateral column of the distal humerus; Type 4, involving the posterior aspect of the trochlea; and Type 5, involving the medial epicondyle.
More recently, Dubberley et al. described a classification system that incorporates information on the fracture pattern, the number of fragments, and the extent of posterior comminution, affecting surgical decision-making and injury prognosis.[4] Type 1 fractures involve the capitellum, with or without involvement of the lateral trochlea; type 2 fractures involve the capitellum in continuity with a longer fragment extending into the trochlea; and type 3 fractures describe a fracture with separate capitellar and trochlear fragments. Each of these fracture types is divided into subtype A (without posterior comminution) and subtype B (posterior comminution) ([Fig. 1]). Watson et al.[14] They propose a fourth fracture type in the classification, representing type 3 fractures associated with fracture lines in the sagittal and axial planes, creating multiple small fragments of the capitellum and trochlea. The modified Dubberley classification has proven useful for decision-making, recommending plate and screw fixation for type B fractures and arthroplasty for type 4 cases.[15] For this reason, this is our usual classification system for this type of fracture.

Management
Non-surgical management
There are some reports of conservative management of these injuries. In 1996, Ochner et al.,[16] described orthopedic management of non-comminuted capitellum fractures with a reduction maneuver with extension and supination, followed by elbow traction and varus stress to reduce the fragment with flexion and pronation ([Fig. 2]). On the other hand, Cutbush et al[17] reported conservative management of these fractures in 7 patients with no signs of displacement, osteoarthritis, or avascular necrosis, and good functionality at an average of 41 months. However, this study only included 7 patients and type 1 Bryan and Morrey fractures, which represent only 40% of these fractures.[17] There are some clinical case reports of conservative management of these injuries with good results;[18] [19] however, there is no good quality evidence regarding orthopedic management for this type of fracture. Therefore, conservative management of these fractures should be considered in older patients with low functional demands or comorbidities that contraindicate or prevent surgery.

Surgical management
Positioning and preoperative considerations
The positioning and approach of the patient depend on the type of fracture and the surgeon's preferences. In the case of performing an open reduction and internal fixation, our preference is to do it in supine position, with a lateral hand table. We usually add an arm support over the patient's chest, which allows for a greater variety of positions and improves circumferential visualization of the joint. Once positioned and anesthetized, the stability of the elbow must always be evaluated with varus, valgus, and posterolateral maneuvers, both clinically and under fluoroscopy, as mentioned in the publication by Carroll et al.[2]
There are different approaches described that can be used depending on the type of fracture, associated injuries, and the surgeon's preference. The anterolateral approach, described by Imatini et al.[20] describes an intermuscular plane between the brachialis and brachioradialis, providing a frontal view of the capitellum. The theoretical advantage of this approach is to avoid devascularizing the posterior region of the capitellum to prevent potential complications. Its disadvantage is that it cannot be extended, requires dissection and retraction of the radial nerve, and does not allow visualization of the posterior wall of the capitellum, limiting its indication to patients with posterior comminution. The lateral approach to the elbow is an option for an anterior and posterior view of the lateral side and can also treat certain associated injuries. Different muscle intervals have been described, and their use depends on the integrity of the lateral ligaments. In the case of a lateral ligament injury, the approach described by Kocher[21] is an alternative that allows us to properly evaluate the fracture, fix it and at the same time fix the ligament injury. If the ligament complex is intact, a Kaplan approach[22] can be performed between the extensor carpi radialis brevis (ECRB) and the extensor digitorum communis (EDC) or a split of the extensor digitorum communis ([Fig. 3]). Some disadvantages of the lateral approach include the difficulty in assessing and reducing trochlear fractures when they are not in continuity. In these cases, a medial elbow approach can be added to achieve adequate reduction and fixation of the trochlea through an over-the-top Hotchkiss approach.[23] Although rarely necessary, in cases of extensive joint compromise and comminution, an olecranon osteotomy with wide exposure of most of the articular surface may be required.[14]

Fixation techniques
Excision of the fragment
Fragment excision is an alternative for small osteochondral fragments, and it can even be performed arthroscopically.[24] Fowles et al[25] described 6 patients managed with fragment excision, 3 acutely within 24 hours and 3 delayed by several months due to persistent symptoms, with better results in those where excision was performed acutely. Despite resection of the capitellum, stability is preserved by the integrity of the ligaments, which must be evaluated prior to fragment excision.[26] However, outcomes are worse when there is more extensive involvement of the lateral region of the capitellum, leading to instability and secondary osteoarthritis.[27] Therefore, capitellum excision can be a treatment option as long as the elbow is stable and the bone fragment is small in size without compromising the most lateral edge of the capitellum.
Kirschner wires
The use of Kirschner wires (KW), either threaded or smooth, is used as a solitary or adjunctive fixation method in the management of these fractures, especially small fragments.[8] [28] The use of threaded KWs is preferred to reduce the risk of migration. Their advantages are minimal cartilage damage and ease of placement, while their disadvantages are possible migration and the need for subsequent removal. One of the few case series reported in the literature is that of He et al.,[29] which presented 20 patients treated with KWs associated with an articulated elbow external fixator with good results and low complication rates. However, in our practice, the use of KWs for the fixation of capitellum fractures is anecdotal.
Insulated screws
One of the most used techniques as a method of fixation of capitellum fractures is screws, as seen in [Fig. 4]. Its main use is in fractures of simpler patterns, without subsequent comminution or bone loss (Dubberley 1A and 2A).[30] [31] [32] [33]

Multiple biomechanical studies have been performed to evaluate the best screw configuration and direction for the fixation of these fractures. On the one hand, screw direction is relevant; Elkowitz et al. demonstrated that fixation with 4.0 mm partial thread posteroanterior (PA) screws provides more stable fixation than anteroposterior (AP) screws, with the benefit of not violating the articular surface.[34] [35] On the other hand, the type of screw is also relevant when fixing these fractures, with improved fixation demonstrated with some specific screw designs. In our practice, these fractures are typically fixed in the PA direction to avoid violating the articular cartilage, except in very small fragments where AP fixation is more predictable and stable. Furthermore, it is common to use cannulated screws to predict the direction and position of our screws with a guide wire, preferably using compression screws to increase the stability of the fragment. In the absence of cannulated or headless screws, the use of locked screws buried in the articular cartilage has been described to prevent osteoarthritis.[14] [36]
Plates
The use of a plate is recommended in fractures with posterior comminution in order to provide support for the fixation of the capitellum, as seen in [Fig. 5].[4] [37] When comminution is present, the anatomical plate can help create a posterior cortex to support the articular fragments, allowing for stable anatomical reduction and early mobility.[38] However, despite obtaining stable anatomical fixation, patterns with posterior comminution are associated with worse clinical results compared to fractures with this intact cortex.[39] In some specific patterns where there is a lateral epicondyle fracture, the use of lateral buttress plates may be helpful to support this fragment and ensure elbow stability as seen in [Fig. 6]. On the other hand, Song et al described the use of anterior anti-slip plates, mini fragment, or third tube, contoured and molded at the articular level, only with fixation of this towards the proximal, with good to excellent results.[40]


Arthroplasty
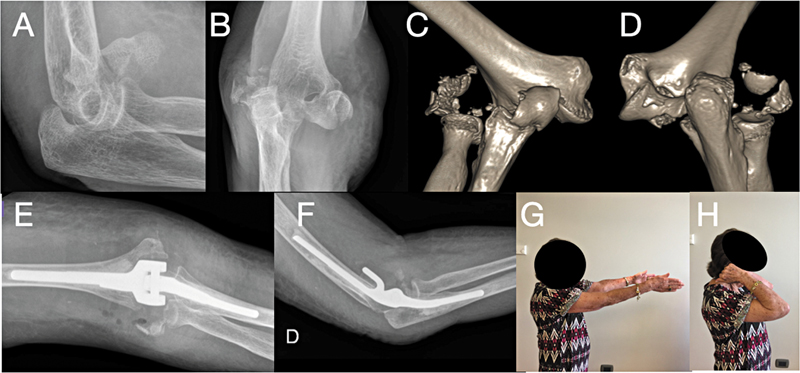
Primary total elbow arthroplasty is an alternative in older patients with Dubberley type III or IV fractures with poor bone stock, as seen in [Fig. 7] [41] due to its high association with loss of reduction, osteosynthesis failure, avascular necrosis, and stiffness.[3] [4] [9] [41] Total elbow arthroplasty is an alternative that has been used in active older patients with these fracture patterns with good short-term functional results.[42] Although there are reports of good results from elbow hemiarthroplasties for distal humerus fractures, they are not available in Chile, and we must remember the functional limitations generated by the use of linked total elbow prostheses. In a multicenter, prospective, randomized clinical trial, McKee et al[41] compared surgical management with reduction and internal fixation versus total elbow arthroplasty in older patients with intra-articular distal humerus fractures. They concluded that patients managed with total arthroplasty had better short-term functional scores, with a tendency toward equal results after one year of evolution on the DASH score. A possible explanation for this is that older patients adapted to their perceived disability, even though their objective physical limitations had not changed. On the other hand, in another study by De Simeone et al., the use of elbow arthroplasty provided faster recovery and more predictable short-term results in older patients with distal humerus fractures.[43] Although these studies do not focus exclusively on isolated fractures of the capitellum and trochlea, we believe that for complex fractures (Dubberley types III and IV) in elderly patients, total elbow arthroplasty represents a valid therapeutic option.

Hemiarthroplasty is an alternative that could eliminate complications related to the ulnar component and a connected (linked) joint, potentially reducing loosening rates and making it easier to revise with a total arthroplasty. Phadnis et al. report good short- and medium-term results, with potential problems with native articular cartilage wear and instability. However, there are no long-term or comparative studies with total arthroplasty.
Arthroscopy
Arthroscopic management is an alternative treatment in fracture patterns without posterior comminution, as seen in [Fig. 8]. Its benefits are minimal dissection, no compromise of dynamic stabilizers, lower risk of infection, removal of loose bodies, and a more accurate assessment of joint reduction.[44] [45] It is primarily recommended for fractures without posterior comminution (Dubberley Subtype A) and with a single capitellum fragment or capitellum + trochlea fragment.[45] There are good results reported in the literature, such as those presented by Zhang et al.,[46] with satisfactory reduction and minimal soft tissue dissection. The disadvantages of this technique are that it is technically demanding and can only be performed in certain fracture patterns.[47]

Complications
Due to the limited reporting and conservative management of these injuries, most complications are secondary to surgical treatment. The complication rate is higher in fractures with posterior comminution (Dubberley subtype B) compared to those with an intact posterior wall.[37] On the other hand, advanced age and a fracture pattern with greater articular comminution present higher complication rates.[46] The complication rate of these fractures reaches approximately 20%, with reoperation due to symptomatic osteosynthesis being the most frequent at 10.4%, followed by elbow stiffness (6%).[48] Other reported complications include neurological injury (2%), nonunion (1.5%), and infection (1.2%).[48] One of the keys to reducing these complications is achieving a stable anatomic reduction of the distal humerus that allows for early mobilization of the elbow, as recently demonstrated by Nagashree et al.[49] However, occasionally, even after an anatomic reduction, post-traumatic osteoarthritis occurs in 0 to 32% of cases, affecting both flexion–extension and functional scores.[40] [50] Avascular necrosis is rare, with a reported incidence between 0 and 6%[8] [51] [52] [53] and usually asymptomatic.[33] [50] [51] Infection is an uncommon complication and usually superficial; however, it should always be suspected in cases of nonunion.[9] [54]
Nonunion has been described more frequently in patients with conservative management of this type of fracture. In a series of 18 patients, Brouwer et al.,[9] described a 44% rate of nonunions, all in subtype 3B fracture patterns. They concluded that there is a higher risk in fractures with posterior comminution and multiple articular fragments.
Conclusions
The management of capitellum fractures remains a clinical challenge due to their diverse patterns and severity, as well as their high incidence of postoperative complications. The Dubberley classification, along with a detailed preoperative assessment, remains essential for surgical planning and prognostication. Surgical approaches have shown favorable results depending on the type of fracture, with most of these injuries managed with open reduction and internal screw fixation, with a plate associated in cases of posterior comminution. The use of arthroscopy has improved visualization of these fractures, achieving anatomical reduction in a less invasive manner. Finally, elbow arthroplasty is an alternative for elderly patients with comminuted fractures.
Conflicto de Intereses
Ninguno declarado.
-
Referencias
- 1 Bryan RS, Morrey BF. Fractures of the distal humerus. In: Morrey BF. ed. The elbow and its disorders. Philadelphia: WB Saunders; 1985: 302-399
- 2 Carroll MJ, Athwal GS, King GJ, Faber KJ. Capitellar and Trochlear Fractures. Hand Clin 2015; 31 (04) 615-630
- 3 Durakbasa MO, Gumussuyu G, Gungor M, Ermis MN. Distal humeral coronal plane fractures: management, complications and outcome. J Shoulder Elbow Surg 2013; 22 (04) 560-566
- 4 Dubberley JH, Faber KJ, Macdermid JC, Patterson SD, King GJW. Outcome after open reduction and internal fixation of capitellar and trochlear fractures. J Bone Joint Surg Am 2006; 88 (01) 46-54
- 5 DeLude JA, Bicknell RT, MacKenzie GA. et al. An anthropometric study of the bilateral anatomy of the humerus. J Shoulder Elbow Surg 2007; 16 (04) 477-483
- 6 Spiegel PG. Orthopaedic Trauma Association Committee for Coding and Classification. Fracture and dislocation compendium. J Orthop Trauma 1996; 10 (Suppl. 01) v-ix , 1–154
- 7 Stamatis E, Paxinos O. The treatment and functional outcome of type IV coronal shear fractures of the distal humerus: a retrospective review of five cases. J Orthop Trauma 2003; 17 (04) 279-284
- 8 Heck S, Zilleken C, Pennig D, Koslowsky TC. Reconstruction of radial capitellar fractures using fine-threaded implants (FFS). Injury 2012; 43 (02) 164-168
- 9 Brouwer KM, Jupiter JB, Ring D. Nonunion of operatively treated capitellum and trochlear fractures. J Hand Surg Am 2011; 36 (05) 804-807
- 10 O'Driscoll SW, Jupiter JB, King GJ, Hotchkiss RN, Morrey BF. The unstable elbow. Instr Course Lect 2001; 50: 89-102
- 11 McKee MD, Jupiter JB, Bamberger HB. Coronal shear fractures of the distal end of the humerus. J Bone Joint Surg Am 1996; 78 (01) 49-54
- 12 Doornberg J, Lindenhovius A, Kloen P, van Dijk CN, Zurakowski D, Ring D. Two and three-dimensional computed tomography for the classification and management of distal humeral fractures. Evaluation of reliability and diagnostic accuracy. J Bone Joint Surg Am 2006; 88 (08) 1795-1801
- 13 Ring D, Jupiter JB, Gulotta L. Articular fractures of the distal part of the humerus. J Bone Joint Surg Am 2003; 85 (02) 232-238
- 14 Watson JJ, Bellringer S, Phadnis J. Coronal shear fractures of the distal humerus: Current concepts and surgical techniques. Shoulder Elbow 2020; 12 (02) 124-135
- 15 Shergold S, Derias M, Moverley R, Murphy RJ, Guryel E, Phadnis J. Coronal shear fractures of the distal humerus managed according to the Modified Dubberley Classification System. J Shoulder Elbow Surg 2022; 31 (01) 133-142
- 16 Ochner RS, Bloom H, Palumbo RC, Coyle MP. Closed reduction of coronal fractures of the capitellum. J Trauma 1996; 40 (02) 199-203
- 17 Cutbush K, Andrews S, Siddiqui N, Brown LM, Ross M. Capitellar fractures-is open reduction and internal fixation necessary?. J Orthop Trauma 2015; 29 (01) 50-53
- 18 Ogawa T, Shirasawa S. Conservative treatment in displaced fractures of the humeral capitellum: a reduction technique under local anaesthesia. BMJ Case Rep 2018; 2018: bcr2017223820
- 19 Nakamura Y, Tsubo K, Sasaki N. et al. Conservative treatment for coronal shear fracture of the distal humerus: a case report. JSES Rev Rep Tech 2022; 2 (04) 580-583
- 20 Imatani J, Morito Y, Hashizume H, Inoue H. Internal fixation for coronal shear fracture of the distal end of the humerus by the anterolateral approach. J Shoulder Elbow Surg 2001; 10 (06) 554-556
- 21 Kocher T. Textbook of Operative Surgery, ed 3. London, United Kingdom: Adam and Charles Black; 1911
- 22 Kaplan EB. Surgical approaches to the proximal end of the radius and its use in fractures of the head and neck of the radius. J Bone Joint Surg 1941; 23: 86
- 23 Kasparyan NG, Hotchkiss RN. Dynamic skeletal fixation in the upper extremity. Hand Clin 1997; 13 (04) 643-663
- 24 Feldman MD. Arthroscopic excision of type II capitellar fractures. Arthroscopy 1997; 13 (06) 743-748
- 25 Fowles JV, Kassab MT. Fracture of the capitulum humeri. Treatment by excision. J Bone Joint Surg Am 1974; 56 (04) 794-798
- 26 Sabo MT, Fay K, McDonald CP, Ferreira LM, Johnson JA, King GJ. Effect of coronal shear fractures of the distal humerus on elbow kinematics and stability. J Shoulder Elbow Surg 2010; 19 (05) 670-680
- 27 Mancini GB, Fiacca C, Picuti G. Resection of the radial capitellum. Long-term results. Ital J Orthop Traumatol 1989; 15 (03) 295-302
- 28 Koslowsky TC, Mader K, Kirchner S, Gausepohl T, Pennig D. Treatment of medial malleolar fractures using fine-threaded K-wires: a new operative technique. J Trauma 2007; 62 (01) 258-261
- 29 He S-K, Zhao S-C, Guo J-H, Qin T-W, Huang F-G. Combined use of Kirschner wires and hinged external fixator for capitellar and trochlear fractures: a minimum 24-month follow-up. ANZ J Surg 2019; 89 (03) 196-200
- 30 Lopiz Y, Rodríguez-González A, García-Fernández C, Marco F. Open reduction and internal fixation of coronal fractures of the capitellum in patients older than 65 years. J Shoulder Elbow Surg 2016; 25 (03) 369-375
- 31 Ruchelsman DE, Tejwani NC, Kwon YW, Egol KA. Open reduction and internal fixation of capitellar fractures with headless screws. Surgical technique. J Bone Joint Surg Am 2009; 91 (Suppl 2 Pt 1): 38-49
- 32 Mahirogullari M, Kiral A, Solakoglu C, Pehlivan O, Akmaz I, Rodop O. Treatment of fractures of the humeral capitellum using herbert screws. J Hand Surg [Br] 2006; 31 (03) 320-325
- 33 Mighell M, Virani NA, Shannon R, Echols Jr EL, Badman BL, Keating CJ. Large coronal shear fractures of the capitellum and trochlea treated with headless compression screws. J Shoulder Elbow Surg 2010; 19 (01) 38-45
- 34 Elkowitz SJ, Polatsch DB, Egol KA, Kummer FJ, Koval KJ. Capitellum fractures: a biomechanical evaluation of three fixation methods. J Orthop Trauma 2002; 16 (07) 503-506
- 35 Elkowitz SJ, Kubiak EN, Polatsch D, Cooper J, Kummer FJ, Koval KJ. Comparison of two headless screw designs for fixation of capitellum fractures. Bull Hosp Jt Dis 2003; 61 (3-4): 123-126
- 36 Watts AC, Morris A, Robinson CM. Fractures of the distal humeral articular surface. J Bone Joint Surg Br 2007; 89 (04) 510-515
- 37 Marinelli A, Cavallo M, Guerra E, Ritali A, Bettelli G, Rotini R. Does the presence of posterior comminution modify the treatment and prognosis in capitellar and trochlear fractures? Study performed on 45 consecutive patients. Injury 2018; 49 (Suppl. 03) S84-S93
- 38 Wang P, Kandemir U, Zhang K. et al. Treatment of capitellar and trochlear fractures with posterior comminution: minimum 2-year follow-up. J Shoulder Elbow Surg 2019; 28 (05) 931-938
- 39 Yoshida S, Sakai K, Nakama K. et al. Treatment of Capitellum and Trochlea Fractures Using Headless Compression Screws and a Combination of Dorsolateral Locking Plates. Cureus 2021; 13 (03) e13740
- 40 Song Z, Wang Q, Ma T. et al. Anti-sliding plate technique for coronal shear fractures of the distal humerus. J Orthop Surg Res 2020; 15 (01) 18
- 41 McKee MD, Veillette CJH, Hall JA. et al. A multicenter, prospective, randomized, controlled trial of open reduction–internal fixation versus total elbow arthroplasty for displaced intra-articular distal humeral fractures in elderly patients. J Shoulder Elbow Surg 2009; 18 (01) 3-12
- 42 Kepler CK, Kummer JL, Lorich DG, Weiland AJ. Radiocapitellar prosthetic arthroplasty for capitellar nonunion. J Shoulder Elbow Surg 2010; 19 (02) e13-e17
- 43 DeSimone LJ, Sanchez-Sotelo J. Total elbow arthroplasty for distal humerus fractures. Orthop Clin North Am 2013; 44 (03) 381-387 , ix–x
- 44 Phadnis J, Watts AC, Bain GI. Elbow hemiarthroplasty for the management of distal humeral fractures: current technique, indications and results. Shoulder Elbow 2016; 8 (03) 171-183
- 45 Van Nguyen T, Kholinne E, AlSomali K, Cho CH, Koh KH, Jeon IH. Technique for Arthroscopic-Assisted Reduction and Cannulated Screw Fixation for Coronal Shear Fractures of the Distal Humerus. Arthrosc Tech 2021; 10 (04) e949-e955
- 46 Mukohara S, Mifune Y, Inui A. et al. Effects of trochlear fragmentation on functional outcome in coronal shear fractures: a retrospective comparative study. JSES Int 2021; 5 (03) 571-577
- 47 Matache BA, Culliton K, Chang Y, Cron GO, Louati H, Pollock JW. Lateral Trochlear Ridge: A Non-Articulating Zone for Anterior-to-Posterior Screw Placement in Fractures Involving the Capitellum and Trochlea. J Bone Joint Surg Am 2019; 101 (15) e75
- 48 Lari A, Alrumaidhi Y, Martinez D. et al. Clinical Outcomes and Management Strategies for Capitellum and Trochlea Fractures: A Systematic Review. Orthop Res Rev 2024; 16: 179-197
- 49 Nagashree V, Dheenadhayalan J, Sundaram VP. et al. Outcome determinants for coronal shear fractures of the distal humerus. Int Orthop 2024; 48 (05) 1295-1302
- 50 Demir MT, Ertan Birsel S, Salih M, Pirinçci Y, Birsel O, Kesmezacar H. Outcome after the surgical treatment of the Dubberley type B distal humeral capitellar and trochlear fractures with a buttress plate. Acta Orthop Traumatol Turc 2020; 54 (04) 364-371
- 51 Ravishankar MR, Kumar MN, Raut R. Choice of surgical approach for capitellar fractures based on pathoanatomy of fractures: outcomes of surgical management. Eur J Orthop Surg Traumatol 2017; 27 (02) 233-242
- 52 Rausch V, Königshausen M, Schildhauer TA, Gessmann J, Seybold D. Fractures of the capitellum humeri and their associated injuries. Obere Extrem 2018; 13 (01) 33-37
- 53 Cottalorda J, Bourelle S. The often-missed Kocher-Lorenz elbow fracture. Orthop Traumatol Surg Res 2009; 95 (07) 547-550
- 54 Ashwood N, Verma M, Hamlet M, Garlapati A, Fogg Q. Transarticular shear fractures of the distal humerus. J Shoulder Elbow Surg 2010; 19 (01) 46-52
Address for correspondence
Publication History
Received: 20 March 2025
Accepted: 04 August 2025
Article published online:
22 December 2025
© 2025. Sociedad Chilena de Ortopedia y Traumatologia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua Rego Freitas, 175, loja 1, República, São Paulo, SP, CEP 01220-010, Brazil
-
Referencias
- 1 Bryan RS, Morrey BF. Fractures of the distal humerus. In: Morrey BF. ed. The elbow and its disorders. Philadelphia: WB Saunders; 1985: 302-399
- 2 Carroll MJ, Athwal GS, King GJ, Faber KJ. Capitellar and Trochlear Fractures. Hand Clin 2015; 31 (04) 615-630
- 3 Durakbasa MO, Gumussuyu G, Gungor M, Ermis MN. Distal humeral coronal plane fractures: management, complications and outcome. J Shoulder Elbow Surg 2013; 22 (04) 560-566
- 4 Dubberley JH, Faber KJ, Macdermid JC, Patterson SD, King GJW. Outcome after open reduction and internal fixation of capitellar and trochlear fractures. J Bone Joint Surg Am 2006; 88 (01) 46-54
- 5 DeLude JA, Bicknell RT, MacKenzie GA. et al. An anthropometric study of the bilateral anatomy of the humerus. J Shoulder Elbow Surg 2007; 16 (04) 477-483
- 6 Spiegel PG. Orthopaedic Trauma Association Committee for Coding and Classification. Fracture and dislocation compendium. J Orthop Trauma 1996; 10 (Suppl. 01) v-ix , 1–154
- 7 Stamatis E, Paxinos O. The treatment and functional outcome of type IV coronal shear fractures of the distal humerus: a retrospective review of five cases. J Orthop Trauma 2003; 17 (04) 279-284
- 8 Heck S, Zilleken C, Pennig D, Koslowsky TC. Reconstruction of radial capitellar fractures using fine-threaded implants (FFS). Injury 2012; 43 (02) 164-168
- 9 Brouwer KM, Jupiter JB, Ring D. Nonunion of operatively treated capitellum and trochlear fractures. J Hand Surg Am 2011; 36 (05) 804-807
- 10 O'Driscoll SW, Jupiter JB, King GJ, Hotchkiss RN, Morrey BF. The unstable elbow. Instr Course Lect 2001; 50: 89-102
- 11 McKee MD, Jupiter JB, Bamberger HB. Coronal shear fractures of the distal end of the humerus. J Bone Joint Surg Am 1996; 78 (01) 49-54
- 12 Doornberg J, Lindenhovius A, Kloen P, van Dijk CN, Zurakowski D, Ring D. Two and three-dimensional computed tomography for the classification and management of distal humeral fractures. Evaluation of reliability and diagnostic accuracy. J Bone Joint Surg Am 2006; 88 (08) 1795-1801
- 13 Ring D, Jupiter JB, Gulotta L. Articular fractures of the distal part of the humerus. J Bone Joint Surg Am 2003; 85 (02) 232-238
- 14 Watson JJ, Bellringer S, Phadnis J. Coronal shear fractures of the distal humerus: Current concepts and surgical techniques. Shoulder Elbow 2020; 12 (02) 124-135
- 15 Shergold S, Derias M, Moverley R, Murphy RJ, Guryel E, Phadnis J. Coronal shear fractures of the distal humerus managed according to the Modified Dubberley Classification System. J Shoulder Elbow Surg 2022; 31 (01) 133-142
- 16 Ochner RS, Bloom H, Palumbo RC, Coyle MP. Closed reduction of coronal fractures of the capitellum. J Trauma 1996; 40 (02) 199-203
- 17 Cutbush K, Andrews S, Siddiqui N, Brown LM, Ross M. Capitellar fractures-is open reduction and internal fixation necessary?. J Orthop Trauma 2015; 29 (01) 50-53
- 18 Ogawa T, Shirasawa S. Conservative treatment in displaced fractures of the humeral capitellum: a reduction technique under local anaesthesia. BMJ Case Rep 2018; 2018: bcr2017223820
- 19 Nakamura Y, Tsubo K, Sasaki N. et al. Conservative treatment for coronal shear fracture of the distal humerus: a case report. JSES Rev Rep Tech 2022; 2 (04) 580-583
- 20 Imatani J, Morito Y, Hashizume H, Inoue H. Internal fixation for coronal shear fracture of the distal end of the humerus by the anterolateral approach. J Shoulder Elbow Surg 2001; 10 (06) 554-556
- 21 Kocher T. Textbook of Operative Surgery, ed 3. London, United Kingdom: Adam and Charles Black; 1911
- 22 Kaplan EB. Surgical approaches to the proximal end of the radius and its use in fractures of the head and neck of the radius. J Bone Joint Surg 1941; 23: 86
- 23 Kasparyan NG, Hotchkiss RN. Dynamic skeletal fixation in the upper extremity. Hand Clin 1997; 13 (04) 643-663
- 24 Feldman MD. Arthroscopic excision of type II capitellar fractures. Arthroscopy 1997; 13 (06) 743-748
- 25 Fowles JV, Kassab MT. Fracture of the capitulum humeri. Treatment by excision. J Bone Joint Surg Am 1974; 56 (04) 794-798
- 26 Sabo MT, Fay K, McDonald CP, Ferreira LM, Johnson JA, King GJ. Effect of coronal shear fractures of the distal humerus on elbow kinematics and stability. J Shoulder Elbow Surg 2010; 19 (05) 670-680
- 27 Mancini GB, Fiacca C, Picuti G. Resection of the radial capitellum. Long-term results. Ital J Orthop Traumatol 1989; 15 (03) 295-302
- 28 Koslowsky TC, Mader K, Kirchner S, Gausepohl T, Pennig D. Treatment of medial malleolar fractures using fine-threaded K-wires: a new operative technique. J Trauma 2007; 62 (01) 258-261
- 29 He S-K, Zhao S-C, Guo J-H, Qin T-W, Huang F-G. Combined use of Kirschner wires and hinged external fixator for capitellar and trochlear fractures: a minimum 24-month follow-up. ANZ J Surg 2019; 89 (03) 196-200
- 30 Lopiz Y, Rodríguez-González A, García-Fernández C, Marco F. Open reduction and internal fixation of coronal fractures of the capitellum in patients older than 65 years. J Shoulder Elbow Surg 2016; 25 (03) 369-375
- 31 Ruchelsman DE, Tejwani NC, Kwon YW, Egol KA. Open reduction and internal fixation of capitellar fractures with headless screws. Surgical technique. J Bone Joint Surg Am 2009; 91 (Suppl 2 Pt 1): 38-49
- 32 Mahirogullari M, Kiral A, Solakoglu C, Pehlivan O, Akmaz I, Rodop O. Treatment of fractures of the humeral capitellum using herbert screws. J Hand Surg [Br] 2006; 31 (03) 320-325
- 33 Mighell M, Virani NA, Shannon R, Echols Jr EL, Badman BL, Keating CJ. Large coronal shear fractures of the capitellum and trochlea treated with headless compression screws. J Shoulder Elbow Surg 2010; 19 (01) 38-45
- 34 Elkowitz SJ, Polatsch DB, Egol KA, Kummer FJ, Koval KJ. Capitellum fractures: a biomechanical evaluation of three fixation methods. J Orthop Trauma 2002; 16 (07) 503-506
- 35 Elkowitz SJ, Kubiak EN, Polatsch D, Cooper J, Kummer FJ, Koval KJ. Comparison of two headless screw designs for fixation of capitellum fractures. Bull Hosp Jt Dis 2003; 61 (3-4): 123-126
- 36 Watts AC, Morris A, Robinson CM. Fractures of the distal humeral articular surface. J Bone Joint Surg Br 2007; 89 (04) 510-515
- 37 Marinelli A, Cavallo M, Guerra E, Ritali A, Bettelli G, Rotini R. Does the presence of posterior comminution modify the treatment and prognosis in capitellar and trochlear fractures? Study performed on 45 consecutive patients. Injury 2018; 49 (Suppl. 03) S84-S93
- 38 Wang P, Kandemir U, Zhang K. et al. Treatment of capitellar and trochlear fractures with posterior comminution: minimum 2-year follow-up. J Shoulder Elbow Surg 2019; 28 (05) 931-938
- 39 Yoshida S, Sakai K, Nakama K. et al. Treatment of Capitellum and Trochlea Fractures Using Headless Compression Screws and a Combination of Dorsolateral Locking Plates. Cureus 2021; 13 (03) e13740
- 40 Song Z, Wang Q, Ma T. et al. Anti-sliding plate technique for coronal shear fractures of the distal humerus. J Orthop Surg Res 2020; 15 (01) 18
- 41 McKee MD, Veillette CJH, Hall JA. et al. A multicenter, prospective, randomized, controlled trial of open reduction–internal fixation versus total elbow arthroplasty for displaced intra-articular distal humeral fractures in elderly patients. J Shoulder Elbow Surg 2009; 18 (01) 3-12
- 42 Kepler CK, Kummer JL, Lorich DG, Weiland AJ. Radiocapitellar prosthetic arthroplasty for capitellar nonunion. J Shoulder Elbow Surg 2010; 19 (02) e13-e17
- 43 DeSimone LJ, Sanchez-Sotelo J. Total elbow arthroplasty for distal humerus fractures. Orthop Clin North Am 2013; 44 (03) 381-387 , ix–x
- 44 Phadnis J, Watts AC, Bain GI. Elbow hemiarthroplasty for the management of distal humeral fractures: current technique, indications and results. Shoulder Elbow 2016; 8 (03) 171-183
- 45 Van Nguyen T, Kholinne E, AlSomali K, Cho CH, Koh KH, Jeon IH. Technique for Arthroscopic-Assisted Reduction and Cannulated Screw Fixation for Coronal Shear Fractures of the Distal Humerus. Arthrosc Tech 2021; 10 (04) e949-e955
- 46 Mukohara S, Mifune Y, Inui A. et al. Effects of trochlear fragmentation on functional outcome in coronal shear fractures: a retrospective comparative study. JSES Int 2021; 5 (03) 571-577
- 47 Matache BA, Culliton K, Chang Y, Cron GO, Louati H, Pollock JW. Lateral Trochlear Ridge: A Non-Articulating Zone for Anterior-to-Posterior Screw Placement in Fractures Involving the Capitellum and Trochlea. J Bone Joint Surg Am 2019; 101 (15) e75
- 48 Lari A, Alrumaidhi Y, Martinez D. et al. Clinical Outcomes and Management Strategies for Capitellum and Trochlea Fractures: A Systematic Review. Orthop Res Rev 2024; 16: 179-197
- 49 Nagashree V, Dheenadhayalan J, Sundaram VP. et al. Outcome determinants for coronal shear fractures of the distal humerus. Int Orthop 2024; 48 (05) 1295-1302
- 50 Demir MT, Ertan Birsel S, Salih M, Pirinçci Y, Birsel O, Kesmezacar H. Outcome after the surgical treatment of the Dubberley type B distal humeral capitellar and trochlear fractures with a buttress plate. Acta Orthop Traumatol Turc 2020; 54 (04) 364-371
- 51 Ravishankar MR, Kumar MN, Raut R. Choice of surgical approach for capitellar fractures based on pathoanatomy of fractures: outcomes of surgical management. Eur J Orthop Surg Traumatol 2017; 27 (02) 233-242
- 52 Rausch V, Königshausen M, Schildhauer TA, Gessmann J, Seybold D. Fractures of the capitellum humeri and their associated injuries. Obere Extrem 2018; 13 (01) 33-37
- 53 Cottalorda J, Bourelle S. The often-missed Kocher-Lorenz elbow fracture. Orthop Traumatol Surg Res 2009; 95 (07) 547-550
- 54 Ashwood N, Verma M, Hamlet M, Garlapati A, Fogg Q. Transarticular shear fractures of the distal humerus. J Shoulder Elbow Surg 2010; 19 (01) 46-52