

Subscribe to RSS
DOI: 10.1055/s-0045-1813261
Vein of Galen Malformation with Pial Arteriovenous Fistula in a 12-month-old Child
Authors

Abstract
Pial arteriovenous fistulas are extremely rare vascular malformations of the brain (accounting for approximately 1.6% of vascular malformations of the brain) and are classified as Galenic and non-Galenic pial fistulas. We present a rare association of a mural-type vein of Galen malformation with a pial fistula involving the precentral branch of the right middle cerebral artery (MCA) in a 12-month-old infant. A 12-month-old preterm male infant, born vaginally with a delayed cry (birth weight 1.2 kg), presented with progressive macrocephaly, recurrent upper respiratory tract infections, developmental delay, and a history of seizures. Neurologically, the child was intact with no focal deficits. He was the firstborn child of a non-consanguineous marriage; maternal antenatal history was notable for polyhydramnios and fetal cardiomegaly detected on antenatal ultrasound. Antenatal scans at 26 and 28 weeks revealed aneurysmal dilation of the vein of Galen. Postnatal transfontanelle ultrasound showed enlarged lateral and third ventricles with a midline cystic lesion exhibiting turbulent flow, suggestive of a high-flow arteriovenous shunt. At 12 months of age, multidetector computed tomography (MDCT)) identified a 37 × 15 mm lobulated soft tissue density in the perimesencephalic/suprasellar region with ventriculomegaly. MRI of the brain confirmed a 35 × 19 × 21 mm flow void in the region of the vein of Galen associated with hydrocephalus, periventricular ooze, and cerebral atrophy. Digital subtraction angiography revealed a mural-type vein of Galen malformation fed by the right posterior choroidal artery, draining into the torcula. Additionally, a separate pial arteriovenous fistula was identified, supplied by the precentral branch of the right MCA, with cortical venous drainage into the superior sagittal sinus. Left sigmoid sinus hypoplasia with redirected venous outflow into the left superior petrosal sinus and cavernous system was noted. Mural-type vein of Galen malformation with concurrent pial arteriovenous fistula. The child was taken up for endovascular embolization. The vein of Galen malformation was embolized using 70% N N-butyl cyanoacrylate (NBCA). Subsequently, transarterial embolization of the right MCA pial fistula was done using coils and Onyx liquid embolic agent in the same sitting. Post-embolization, complete closure of both fistulas was noted. Post-treatment, CT revealed closure of fistulas with no fresh parenchymal abnormality. The child was discharged on postoperative day 6 without any focal deficit. At 3-month follow-up, the patient remained neurologically stable without new deficits, and follow-up MRI was planned.
Keywords
vein of Galen malformation - pial arteriovenous fistula - concurrent vascular malformations - mural-type VOGM - middle cerebral artery - endovascular embolization - infant cerebrovascular anomalyIntroduction
Vein of Galen malformation (VOGM) and pial arteriovenous fistula (PAVF) represent relatively uncommon pediatric neurovascular malformations. A VOGM is characterized by an arteriovenous fistula involving the embryonic precursor of the vein of Galen, the median prosencephalic vein of Markowski. It accounts for about 1% of all pediatric congenital vascular anomalies.[1] [2] Meanwhile, pial arteriovenous malformations, which are characterized by arteriovenous fistula without an intervening nidus, account for about 1.6% of all intracranial vascular malformations.[3] Although both conditions involve abnormal arteriovenous shunting, the presentation of these two malformations in a single patient, particularly in infancy, is exceedingly rare. The high flow shunting in VOGMs can overwhelm the infant's cardiovascular system, leading to cardiac decompensation in both of these malformations. The combined presence of these two malformations can lead to overlapping and sometimes atypical features, making the initial clinical differentiation challenging. Digital subtraction angiography (DSA) plays a vital role because it allows accurate delineation of the individual angioarchitecture of the vascular malformations.[4] To our knowledge, this is the first report of mural-type VOGM with a separate high-flow MCA pial fistula, which may represent a novel association, highlighting diagnostic and therapeutic challenges in complex pediatric shunts.
Case Study
A 12-month-old child was admitted to our hospital with a history of progressive increase in head size ([Fig. 1B]) since birth, along with developmental delay, with recent onset of seizures. History was also significant for recurrent episodes of respiratory tract infections. Clinical examination revealed no neurological deficit. He was the first child of a non-consanguineous marriage, delivered preterm via spontaneous vaginal delivery. The birth was complicated with delayed cry, and the birth weight was 1.2 kg. The mother, aged 21 years, had received regular iron and folic acid supplementation during pregnancy.

Antenatal Scan
Antenatal scan ([Fig. 1A]) of the mother at 26 weeks 5 days and 28 weeks revealed aneurysmal dilation of the vein of Galen, along with polyhydramnios and cardiomegaly.
Post-admission Imaging
-
Transfontanelle sonography: Revealed enlarged bilateral lateral ventricles and the third ventricle, along with a cystic lesion with turbulent flow, and aliasing seen in the floor of the third ventricle, which likely suggested vein of Galen malformation with dilated vertebral arteries and superior sagittal sinus.
-
MDCT ([Fig. 2]): A lobulated soft tissue density of size 37 × 15 mm was noted in the right perimesencephalic cistern, with moderate hydrocephalus and cerebral atrophy.
-
MRI of the brain ([Fig. 2]): Revealed a 35 × 19 × 21 mm large flow void noted in the T2 sequence, with moderate hydrocephalus and cerebral atrophy.

Angiographic Evaluation ([Fig. 3])

Mural-type vein of Galen malformation was noted with a single-hole fistula from the right posterior choroidal artery into the venous sac, which was draining into the torcula. Another pial fistula was noted with an arterial feeder from the precentral branch of the right MCA and venous drainage through the cortical vein into the superior sagittal sinus. Left sigmoid sinus hypoplasia was noted, with venous drainage directed into cavernous sinuses through the left superior petrosal sinus.
Diagnosis
Concurrent presentation of a mural VOGM (single fistula from the right posterior medial choroidal artery) and a high-flow PAVF (right MCA precentral branch).
Procedure
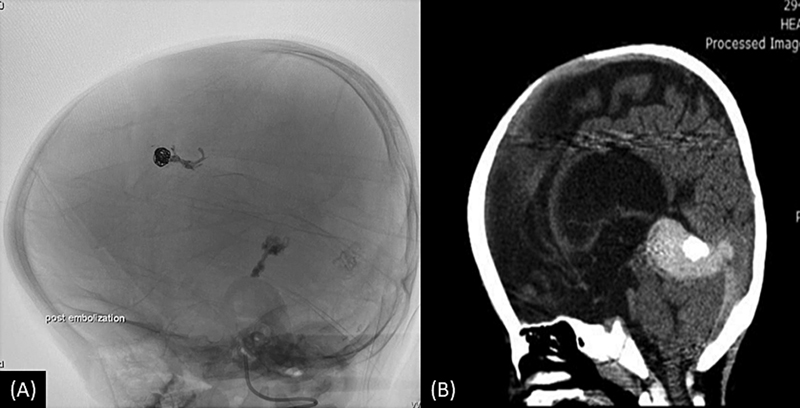
NBCA glue at a concentration of 70% was injected into the posterior choroidal artery at the fistula site, and a check angiogram was taken, which revealed closure of the Galenic fistula. Subsequently, a guide catheter was placed in the right internal carotid artery (ICA), and two coils were deployed into the venous sac of the right MCA pial fistula. After this, Onyx liquid embolic agent was injected at the fistula site, resulting in complete closure of the fistula ([Fig. 3B, D]).
Postoperative Imaging
A post-embolization non-contrast CT of brain demonstrated a hyperdense embolic cast in the vein of Galen and a coil mass and embolic cast at the location of the pial fistula without any fresh parenchymal changes ([Fig. 4]).
At 3-month follow-up, the patient remained neurologically stable without new deficits; developmental delay persisted, and follow-up MRI was planned.
Discussion
True VOGM is caused by abnormal persistence of the median prosencephalic vein (MPV) of Markowski (which develops during 6th–11th weeks of gestation).[5] Pial fistula may also develop later involving the vein of Galen, which forms after MPV regresses. In patients with true VOGM, there is a shunt leading to persistence of MPV which becomes dilated. In true VOGM, the choroidal vein and the thalamostriate vein drain separately, making an “epsilon configuration” which is composed of thalamic and subtemporal veins.[6] Thus, it is believed that the deep venous system is not connected to and does not drain into the ectatic MPV and vein of Galen in children with a true VOGM. In our patient shunt was noted antenatally at 26 to 28 weeks and we could not identify deep venous drainage into the Galenic vein. The angioarchitecture of fistula is discussed in [Fig. 5].

The cause of congenital PAVFs is debatable. It has been proposed that this results from errors in embryogenesis of cerebrovascular structures.[7] Similar to their dural counterparts, PAVFs have also been proposed to be caused by abnormal collateral development via VEGF-dependent angiogenesis.[8] The co-occurrence of these lesions may suggest shared vulnerabilities at this gestational age, where geometric proximity between primitive pial networks and deep Galenic drainage structures such as the basal vein of Rosenthal and its anastomoses with cortical veins enables mutual shunt development.[9] [10] In a slightly older population, pial AVF could also occur as a complication of VOGM-led venous hypertension, likely through mechanisms of vascular remodeling or collateral recruitment.[11] [12] [13] [14] [15] In our patient the two fistulas had an independent drainage pathway. VOGM-related venous hypertension leading to shunt formation may be considered in our patient. A recent study by Martin-Valiente et al in zebrafish models demonstrates that RASA1/EPHB4 mutations disrupt blood flow–mediated MAPK/PI3K signaling, causing defective vascular precursor fusion through this pathway. This results in VOGM-like malformations due to endothelial instability under hemodynamic stress.[16] Even in the absence of overt syndromic features like capillary malformations or lymphatic abnormalities (common in RASA1-associated CM-AVM syndrome) in our patient, the pathway remains a relevant consideration. Genetic testing could not be performed in our patient due to limited resources. This represents an important limitation of our study and highlights a potential area for future research. Disrupted flow signaling may prevent Galenic venous maturation and pial arterial remodeling, with resultant anatomically proximal “hotspots” for fistula development. Although VOGMs alone can lead to significant cardiac stress, the coexistence of VOGM with a PAVF further amplifies the shunt volume, thereby exacerbating both cardiac strain and cerebral injury.
It is important to note that hydrovenous hydrocephalus is a separate clinical entity from obstructive hydrocephalus, which is also why attempting early ventricular shunting to treat the hydrocephalus previously resulted in a 70% complication rate.[17] [18] [19] Shunting can reverse normal pressure gradient and cause brain edema, which can lead to further enlargement of the dilated draining vein of the VOGM, thus predisposing it to rupture.[12] Venous congestion compromises CSF resorption by heightened dural sinus pressure, accounting for our patient's ventriculomegaly. Hence, management of hydrovenous hydrocephalus should be done by closure of vascular shunt.
For treatment, endovascular embolization is still the first line in high-flow shunts, but dual pathology requires lesion-specific techniques. In this case, VOGM was managed via embolization using 70% NBCA, as it is an extremely high-flow shunt. Placement of coils was not financially feasible as a large number of coils would be required to reduce the flow. In this case, pial AVF was treated with embolization (Coils + Onyx), as coils inside the venous sac decreased the velocity of flow, providing a scaffold for controlled containment of Onyx.[20] [21] [22] [23] [24]
Other options are using coils alone and embolization using NBCA glue.
Single-procedure embolization was favored as we were within the contrast limitations, and pial fistula was amenable to easy targeted closure.
Isolated VOGMs show a wide range of outcomes, ranging from normal development following VOGM embolization in type I VOGM (mural type) to high mortality rates despite emergent treatment for VOGM type IV (choroidal with deep venous drainage).[25] Untreated VOGM is almost 100% fatal, and untreated PAVF are 63% fatal.[26] Concurrent shunts need early treatment as they may lead to increased venous hypertension, which would likely lead to hastening “melting brain” syndrome (ischemic parenchymal loss).[27]
Despite successful embolization, delayed cognitive deficits can occur from the failure of shunt occlusion or recanalization. Hence, close MRI follow-up is necessary, as around 37% of VOGM patients can experience complications postoperatively, and 37% may experience long-term complications.[28] [29] [30]
Conclusion
The simultaneous occurrence of VOGM and PAVF in neonates is a rare and complex clinical entity. Limited epidemiological information regarding PAVFs in children highlights their rarity among intracranial vascular malformations. DSA is the gold standard for diagnosis and delineation of the angioarchitecture of both malformations. Endovascular embolization continues to be the first-line treatment strategy, directed toward the obliteration of the ectatic arteriovenous shunts. Embryogenesis of VOGMs and PAVFs during the first trimester of pregnancy provides the theoretical window for a shared period of vulnerability or genetic susceptibility that may allow for their simultaneous presentation. Although treatment of isolated VOGMs shows heterogeneous long-term neurodevelopmental outcomes, PAVFs generally have better prognoses; literature regarding the simultaneous presentation is extremely limited. This highlights the need for further research, specifically through the publication of extensive case reports with long-term follow-up, to further inform our knowledge of natural history, optimal practice management strategies, and long-term neurodevelopmental implications of this rare combination. Knowledge of the possibility of this simultaneous presentation is of paramount importance in the context of guiding clinical management in affected neonates.
Conflict of Interest
None declared.
Acknowledgment
Authors acknowledge the support from the Department of Health Research, Government of India, MDRU – NSCB Medical College, Jabalpur.
Authors' Contributions
A.B. was involved in the conceptualization, manuscript writing, literature review, and imaging review. S.N. contributed through supervision, review of the manuscript, and assistance in manuscript drafting. S.S.T. was responsible for data collection, imaging interpretation, and assistance in manuscript drafting. N.Y. supervised the case, led the interventional procedure, and contributed to imaging interpretation, manuscript review, and editing. All authors have read and approved the final manuscript and agree to be accountable for all aspects of the work.
Ethical Approval
This study was reviewed and approved by the Institutional Ethics Committee of Netaji Subhash Chandra Bose Medical College, Jabalpur, India. Written informed consent for publication of clinical details and images was obtained from the patient's legal guardian. All procedures performed were in accordance with the ethical standards of the institutional and national research committee and with the Declaration of Helsinki (2013 revision).
Patients' Consent
Written informed consent was obtained from the patient's legal guardian for publication of this case report and any accompanying images as per the institutional guidelines.
-
References
- 1 Recinos PF, Rahmathulla G, Pearl M. et al. Vein of Galen malformations: epidemiology, clinical presentations, management. Neurosurg Clin N Am 2012; 23 (01) 165-177
- 2 Casasco A, Lylyk P, Hodes JE, Kohan G, Aymard A, Merland JJ. Percutaneous transvenous catheterization and embolization of vein of galen aneurysms. Neurosurgery 1991; 28 (02) 260-266
- 3 Halbach VV, Higashida RT, Hieshima GB, Hardin CW, Dowd CF, Barnwell SL. Transarterial occlusion of solitary intracerebral arteriovenous fistulas. AJNR Am J Neuroradiol 1989; 10 (04) 747-752
- 4 Valderrama J, Garcia R, Satyarthee G. et al. Intracranial pial arteriovenous fistula mimicking a vein of Galen aneurysm with hydrocephalus managed with endovascular method: case report. Iran J Neurosurg 2017; 3 (02) 67-63
- 5 Raybaud CA, Strother CM, Hald JK. Aneurysms of the vein of Galen: embryonic considerations and anatomical features relating to the pathogenesis of the malformation. Neuroradiology 1989; 31 (02) 109-128
- 6 Kang HS. Update on the vein of Galen aneurysmal malformation: disease concept and genetics. J Korean Neurosurg Soc 2024; 67 (03) 308-314
- 7 Hoh BL, Putman CM, Budzik RF, Ogilvy CS. Surgical and endovascular flow disconnection of intracranial pial single-channel arteriovenous fistulae. Neurosurgery 2001; 49 (06) 1351-1363 , discussion 1363–1364
- 8 Li Q, Zhang Q, Huang QH. et al. A pivotal role of the vascular endothelial growth factor signaling pathway in the formation of venous hypertension-induced dural arteriovenous fistulas. Mol Med Rep 2014; 9 (05) 1551-1558
- 9 Padget DH. The cranial venous system in man in reference to development, adult configuration, and relation to the arteries. Am J Anat 1956; 98 (03) 307-355
- 10 Alvarez H, Garcia Monaco R, Rodesch G, Sachet M, Krings T, Lasjaunias P. Vein of Galen aneurysmal malformations. Neuroimaging Clin N Am 2007; 17 (02) 189-206
- 11 Tu T, Song Z, Ma Y. et al. Adult dural arteriovenous fistulas in Galen region: more to be rediscovered. Front Neurol 2022; 13: 957713
- 12 Paramasivam S. Hydrocephalus in vein of Galen malformations. Neurol India 2021; 69: S376-S379
- 13 Phatouros CC, Halbach VV, Dowd CF. et al. Acquired pial arteriovenous fistula following cerebral vein thrombosis. Stroke 1999; 30 (11) 2487-2490
- 14 Terada T, Nakayama S, Wada A. et al. De novo pial arteriovenous fistula associated with cerebral infarction and venous hypertension: report of 2 cases suggesting a “second hit theory.”. Neurosurg Open 2021; 2 (02) ): okab015
- 15 Lasjaunias PL, Chng SM, Sachet M, Alvarez H, Rodesch G, Garcia-Monaco R. The management of vein of Galen aneurysmal malformations. Neurosurgery 2006; 59 (5, Suppl 3): S184-S194 , discussion S3–S13
- 16 Martin-Valiente E, Du Y, Goemans C. et al. Reversal of cerebrovascular anomalies in a zebrafish model of vein of Galen aneurysm. Nat Cardiovasc Res 2025; 4 (06) 773-789
- 17 Schneider SJ, Wisoff JS, Epstein FJ. Complications of ventriculoperitoneal shunt procedures or hydrocephalus associated with vein of Galen malformations in childhood. Neurosurgery 1992; 30 (05) 706-708
- 18 Jea A, Bradshaw TJ, Whitehead WE, Curry DJ, Dauser RC, Luerssen TG. The high risks of ventriculoperitoneal shunt procedures for hydrocephalus associated with vein of Galen malformations in childhood: case report and literature review. Pediatr Neurosurg 2010; 46 (02) 141-145
- 19 Meila D, Grieb D, Melber K. et al. Hydrocephalus in vein of Galen malformation: etiologies and therapeutic management implications. Acta Neurochir (Wien) 2016; 158 (07) 1279-1284
- 20 Choo DM, Shankar JJS. Onyx versus nBCA and coils in the treatment of intracranial dural arteriovenous fistulas. Interv Neuroradiol 2016; 22 (02) 212-216
- 21 Kim JW, Kim BM, Park KY, Kim DJ, Kim DI. Onyx embolization for isolated type dural arteriovenous fistula using a dual-lumen balloon catheter. Neurosurgery 2016; 78 (05) 627-636
- 22 Loh Y, Duckwiler GR. Onyx Trial Investigators. A prospective, multicenter, randomized trial of the Onyx liquid embolic system and N-butyl cyanoacrylate embolization of cerebral arteriovenous malformations. Clinical article. J Neurosurg 2010; 113 (04) 733-741
- 23 Ernst RJ, Tomsick TA. Embolization materials in neuroradiology. In: Aminoff MJ, Daroff RB. eds. Encyclopedia of the Neurological Sciences. Academic Press; 2003: 119-125
- 24 Khullar D, Andeejani AMI, Bulsara KR. Evolution of treatment options for vein of Galen malformations. J Neurosurg Pediatr 2010; 6 (05) 444-451 PubMed
- 25 Hauck EF, Yarden JA, Hauck LI, Bibawy JM, Mirshahi S, Grant GA. Vein of Galen malformations in the newborn: case series. J Neurosurg Case Lessons 2023; 5 (24) CASE23201
- 26 Nelson PK, Niimi Y, Lasjaunias P, Berenstein A. Endovascular embolization of congenital intracranial pial arteriovenous fistulas. Neuroimaging Clin 1992; 2 (02) 309-317
- 27 Hergan F, Huisman TAGM. “Melting brain” as complication of a vein of Galen aneurysmal malformation diagnosed by fetal MRI. Clin Obstet Gynecol Reprod Med 2018; 4 (01)
- 28 Savage C, Hale AT, Parr MS. et al. Outcomes of endovascular embolization for Vein of Galen malformations: an individual participant data meta-analysis. Front Pediatr 2022; 10: 976060
- 29 Nurimanov C, Makhambetov Y, Menlibayeva K. et al. Long-term outcomes of endovascular embolization in a vein of Galen aneurysmal malformation: a single-center experience. Diagnostics (Basel) 2023; 13 (16) 2704
- 30 Taffin H, Maurey H, Ozanne A. et al. Long-term outcome of vein of Galen malformation. Dev Med Child Neurol 2020; 62 (06) 729-734
Address for correspondence
Publication History
Article published online:
23 December 2025
© 2025. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Recinos PF, Rahmathulla G, Pearl M. et al. Vein of Galen malformations: epidemiology, clinical presentations, management. Neurosurg Clin N Am 2012; 23 (01) 165-177
- 2 Casasco A, Lylyk P, Hodes JE, Kohan G, Aymard A, Merland JJ. Percutaneous transvenous catheterization and embolization of vein of galen aneurysms. Neurosurgery 1991; 28 (02) 260-266
- 3 Halbach VV, Higashida RT, Hieshima GB, Hardin CW, Dowd CF, Barnwell SL. Transarterial occlusion of solitary intracerebral arteriovenous fistulas. AJNR Am J Neuroradiol 1989; 10 (04) 747-752
- 4 Valderrama J, Garcia R, Satyarthee G. et al. Intracranial pial arteriovenous fistula mimicking a vein of Galen aneurysm with hydrocephalus managed with endovascular method: case report. Iran J Neurosurg 2017; 3 (02) 67-63
- 5 Raybaud CA, Strother CM, Hald JK. Aneurysms of the vein of Galen: embryonic considerations and anatomical features relating to the pathogenesis of the malformation. Neuroradiology 1989; 31 (02) 109-128
- 6 Kang HS. Update on the vein of Galen aneurysmal malformation: disease concept and genetics. J Korean Neurosurg Soc 2024; 67 (03) 308-314
- 7 Hoh BL, Putman CM, Budzik RF, Ogilvy CS. Surgical and endovascular flow disconnection of intracranial pial single-channel arteriovenous fistulae. Neurosurgery 2001; 49 (06) 1351-1363 , discussion 1363–1364
- 8 Li Q, Zhang Q, Huang QH. et al. A pivotal role of the vascular endothelial growth factor signaling pathway in the formation of venous hypertension-induced dural arteriovenous fistulas. Mol Med Rep 2014; 9 (05) 1551-1558
- 9 Padget DH. The cranial venous system in man in reference to development, adult configuration, and relation to the arteries. Am J Anat 1956; 98 (03) 307-355
- 10 Alvarez H, Garcia Monaco R, Rodesch G, Sachet M, Krings T, Lasjaunias P. Vein of Galen aneurysmal malformations. Neuroimaging Clin N Am 2007; 17 (02) 189-206
- 11 Tu T, Song Z, Ma Y. et al. Adult dural arteriovenous fistulas in Galen region: more to be rediscovered. Front Neurol 2022; 13: 957713
- 12 Paramasivam S. Hydrocephalus in vein of Galen malformations. Neurol India 2021; 69: S376-S379
- 13 Phatouros CC, Halbach VV, Dowd CF. et al. Acquired pial arteriovenous fistula following cerebral vein thrombosis. Stroke 1999; 30 (11) 2487-2490
- 14 Terada T, Nakayama S, Wada A. et al. De novo pial arteriovenous fistula associated with cerebral infarction and venous hypertension: report of 2 cases suggesting a “second hit theory.”. Neurosurg Open 2021; 2 (02) ): okab015
- 15 Lasjaunias PL, Chng SM, Sachet M, Alvarez H, Rodesch G, Garcia-Monaco R. The management of vein of Galen aneurysmal malformations. Neurosurgery 2006; 59 (5, Suppl 3): S184-S194 , discussion S3–S13
- 16 Martin-Valiente E, Du Y, Goemans C. et al. Reversal of cerebrovascular anomalies in a zebrafish model of vein of Galen aneurysm. Nat Cardiovasc Res 2025; 4 (06) 773-789
- 17 Schneider SJ, Wisoff JS, Epstein FJ. Complications of ventriculoperitoneal shunt procedures or hydrocephalus associated with vein of Galen malformations in childhood. Neurosurgery 1992; 30 (05) 706-708
- 18 Jea A, Bradshaw TJ, Whitehead WE, Curry DJ, Dauser RC, Luerssen TG. The high risks of ventriculoperitoneal shunt procedures for hydrocephalus associated with vein of Galen malformations in childhood: case report and literature review. Pediatr Neurosurg 2010; 46 (02) 141-145
- 19 Meila D, Grieb D, Melber K. et al. Hydrocephalus in vein of Galen malformation: etiologies and therapeutic management implications. Acta Neurochir (Wien) 2016; 158 (07) 1279-1284
- 20 Choo DM, Shankar JJS. Onyx versus nBCA and coils in the treatment of intracranial dural arteriovenous fistulas. Interv Neuroradiol 2016; 22 (02) 212-216
- 21 Kim JW, Kim BM, Park KY, Kim DJ, Kim DI. Onyx embolization for isolated type dural arteriovenous fistula using a dual-lumen balloon catheter. Neurosurgery 2016; 78 (05) 627-636
- 22 Loh Y, Duckwiler GR. Onyx Trial Investigators. A prospective, multicenter, randomized trial of the Onyx liquid embolic system and N-butyl cyanoacrylate embolization of cerebral arteriovenous malformations. Clinical article. J Neurosurg 2010; 113 (04) 733-741
- 23 Ernst RJ, Tomsick TA. Embolization materials in neuroradiology. In: Aminoff MJ, Daroff RB. eds. Encyclopedia of the Neurological Sciences. Academic Press; 2003: 119-125
- 24 Khullar D, Andeejani AMI, Bulsara KR. Evolution of treatment options for vein of Galen malformations. J Neurosurg Pediatr 2010; 6 (05) 444-451 PubMed
- 25 Hauck EF, Yarden JA, Hauck LI, Bibawy JM, Mirshahi S, Grant GA. Vein of Galen malformations in the newborn: case series. J Neurosurg Case Lessons 2023; 5 (24) CASE23201
- 26 Nelson PK, Niimi Y, Lasjaunias P, Berenstein A. Endovascular embolization of congenital intracranial pial arteriovenous fistulas. Neuroimaging Clin 1992; 2 (02) 309-317
- 27 Hergan F, Huisman TAGM. “Melting brain” as complication of a vein of Galen aneurysmal malformation diagnosed by fetal MRI. Clin Obstet Gynecol Reprod Med 2018; 4 (01)
- 28 Savage C, Hale AT, Parr MS. et al. Outcomes of endovascular embolization for Vein of Galen malformations: an individual participant data meta-analysis. Front Pediatr 2022; 10: 976060
- 29 Nurimanov C, Makhambetov Y, Menlibayeva K. et al. Long-term outcomes of endovascular embolization in a vein of Galen aneurysmal malformation: a single-center experience. Diagnostics (Basel) 2023; 13 (16) 2704
- 30 Taffin H, Maurey H, Ozanne A. et al. Long-term outcome of vein of Galen malformation. Dev Med Child Neurol 2020; 62 (06) 729-734