

Subscribe to RSS
DOI: 10.1055/s-0045-1813644
Beyond Turf Wars: Redefining Boundaries and Building Consensus in Interventional Radiology
Authors


Abstract
Interventional radiology (IR) has evolved from diagnostic angiography to a core therapeutic specialty addressing acute ischemic stroke, peripheral arterial disease, hepatobiliary obstruction, and cancer care. This expansion has blurred professional boundaries, leading to “turf wars” with diagnostic radiology, neurology, neurosurgery, vascular surgery, cardiology, and oncology. While many practitioners avoid discussing turf openly due to its controversial nature, a scientific approach reveals both challenges and constructive outcomes. Using a Delphi-style framework of consensus, disputes can be reframed as opportunities for growth.
A systematic review was conducted according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 guidelines. Databases searched included PubMed/MEDLINE, Embase, Scopus, Web of Science, Cochrane Library, and DOAJ (2000–2025). Search terms combined “interventional radiology” with “turf wars,” “scope of practice,” “referral,” “outcomes,” “training,” and “policy.” Eligible studies included comparative outcomes analyses, registries, society guidelines, and policy reports. Data were synthesized narratively, emphasizing referral dynamics, outcomes parity, training, and society/policy roles.
Seventy-three studies, including registry analyses, comparative cohorts, and society guidelines, were included. Five themes emerged: (1) Neurointervention—stroke thrombectomy outcomes are equivalent across IR, neurosurgery, and neurology when training is standardized, yet activation pathways remain contested. (2) Peripheral vascular intervention—IR procedures reduce complications and cost relative to surgery, although vascular surgeons often control referrals. (3) Interventional oncology/hepatobiliary IR—tumor boards with IR representation significantly increase ablation and TACE/TARE (transarterial chemoembolization/transarterial radioembolization utilization), but surgical colleagues often dominate early decision-making. (4) Intra-radiology dynamics—debates persist between IR and diagnostic radiology, and between neuro-IR and peripheral IR, reinforcing the importance of imaging literacy. (5) Society/policy roles—credentialing, coding, and advocacy (Society of Interventional Radiology, Cardiovascular and Interventional Radiological Society of Europe, European Society of Radiology, Indian Society of Vascular and Interventional Radiology) remain pivotal to IR's recognition.
Turf wars in IR are less markers of dysfunction than signs of maturation. When framed symmetrically—acknowledging the concerns of IR and surgical/clinical colleagues—they catalyze positive effects: protocolization, registry development, training harmonization, and policy traction. IR's future rests not on defending turf but on demonstrating measurable outcomes, building consensus, and delivering patient-centered care.
Introduction
Interventional radiology (IR) has grown from Charles Dotter's first angioplasty in 1964[1] into a specialty central to modern medicine. No longer limited to diagnostic angiography, IR now offers minimally invasive therapies for acute ischemic stroke, peripheral arterial disease (PAD), hepatocellular carcinoma (HCC), uterine fibroids, venous disease, and hepatobiliary obstruction. These procedures reduce morbidity, shorten hospitalization, and frequently provide cost-effective alternatives to surgery.[2]
This rapid expansion has inevitably generated turf wars—professional disputes over procedural ownership.[3] In IR, these conflicts arise on three levels. First, within radiology, tensions exist between IR and diagnostic radiology (DR) over imaging literacy, and between neuro-IR and peripheral IR over resources. Second, across specialties, IR overlaps with neurology and neurosurgery (stroke, aneurysms), vascular surgery (PAD, venous disease), cardiology (endovascular interventions), surgical oncology (ablation), and hepatobiliary surgery (embolization and drainage). Third, at the policy level, coding and credentialing frameworks often determine visibility and reimbursement.
Such disputes are not unique. Gastroenterology took endoscopy from radiology; cardiology consolidated angioplasty and echocardiography. IR's uniqueness lies in its dual identity: imaging mastery coupled with therapeutic capability. This duality not only enables unique contributions but also makes boundaries fragile.
Despite their importance, turf wars are seldom discussed openly due to political sensitivities. Yet systematic analysis is essential. Using a Delphi-style consensus analogy, conflicts can be reframed as iterative steps toward maturity. Literature already shows outcomes parity: IR achieves results comparable to neurosurgeons in stroke thrombectomy[4] and to surgeons in oncologic ablation[5] when training is standardized. Professional societies such as Society of Interventional Radiology (SIR), Cardiovascular and Interventional Radiological Society of Europe (CIRSE), and Indian Society of Vascular and Interventional Radiology (ISVIR) emphasize clinical ownership, harmonized curricula, and policy advocacy[6] [7] as tools to secure IR's future.
Turf wars, therefore, should not be viewed solely as crises. They are catalysts—clarifying training standards, stimulating registries, and strengthening IR's integration into multidisciplinary care.
Materials and Methods
Review Design and Rationale
This study was conducted as a systematic review structured in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. The review aimed to consolidate evidence on the phenomenon of “turf wars” in IR, focusing on comparative outcomes, referral dynamics, training standards, credentialing, and policy frameworks. Because the topic spans clinical outcomes, health systems research, and policy documents, a narrative thematic synthesis approach was selected rather than quantitative meta-analysis. This design allowed integration of heterogeneous data sources—ranging from randomized controlled trials (RCTs) and registry analyses to consensus guidelines and society position papers—into a coherent synthesis.
Data Sources and Search Strategy
We systematically searched six major biomedical databases to ensure comprehensive coverage:
-
PubMed/MEDLINE (National Library of Medicine)—for peer-reviewed clinical and policy studies.
-
Embase (Elsevier)—to capture European and non-U.S. studies.
-
Scopus (Elsevier)—for broad coverage of interdisciplinary literature.
-
Web of Science Core Collection (Clarivate Analytics)—for citation tracking and gray literature.
-
Cochrane Library (Wiley)—for systematic reviews and evidence syntheses.
-
Directory of Open Access Journals (DOAJ)—to capture open-access articles not indexed elsewhere.
In addition, supplementary searches were undertaken in:
-
Google Scholar (first 200 hits, ranked by relevance).
-
Web sites of relevant professional societies: SIR, CIRSE, European Society of Radiology (ESR), American College of Radiology, and ISVIR. These sources were particularly important for identifying consensus statements, white papers, and policy documents.
Timeframe: January 1, 2000 to August 15, 2025. This period was chosen to reflect contemporary practice, coinciding with IR's evolution from primarily diagnostic angiography into a clinically recognized specialty.
Search Terms and Boolean Logic
Search strategies were iteratively refined in collaboration with an experienced medical librarian. Four broad concept domains were identified, and their terms were combined using Boolean operators (“AND,” “OR”) and truncations (“*”).
-
Turf/Scope of Practice: “turf war*,” “scope of practice,” “inter-specialty conflict,” “professional boundary,” “encroachment,” “ownership.”
-
IR Domains: “interventional radiology,” “neurointervention,” “peripheral intervention,” “interventional oncology,” “hepatobiliary intervention,” “endovascular therapy.”
-
Outcomes: “outcomes,” “mortality,” “complications,” “safety,” “efficacy,” “success rate,” “comparative study.”
-
Training and Policy: “training standards,” “curriculum,” “credentialing,” “accreditation,” “policy,” “guideline,” “society statement,” “reimbursement,” “coding.”
Example PubMed Query
(“interventional radiology”[MeSH] OR “neurointervention” OR “interventional oncology”) AND (“turf wars” OR “scope of practice” OR “professional boundary” OR “encroachment”) AND (“training” OR “credentialing” OR “outcomes” OR “policy” OR “guideline”)
Each database strategy was adapted to its syntax. Hand-searching of reference lists from included articles supplemented the electronic search.
Eligibility Criteria
Inclusion Criteria
-
Language: English.
-
Publication type: peer-reviewed original research (RCTs, prospective and retrospective cohort studies, registry analyses), systematic or narrative reviews, consensus guidelines, policy analyses, and society statements.
-
Content: Must directly or indirectly address turf conflicts involving IR, including comparative outcomes, referral dynamics, training/credentialing, or policy/advocacy roles.
Exclusion Criteria
-
Case reports/series without turf relevance.
-
Non-English publications without accessible translations.
-
Purely technical or engineering notes unrelated to interspecialty boundaries.
-
Opinion blogs or nonacademic commentaries.
Study Selection Process
The search identified 1,243 records. After removal of duplicates, 912 records remained. Title and abstract screening yielded 374 potential studies. Of these, 102 full texts were reviewed in detail, and 73 studies met inclusion criteria.
Study selection was performed by two independent reviewers. Disagreements were resolved through discussion, and if consensus was not reached, a third reviewer adjudicated. The entire process was documented in a PRISMA 2020 flow diagram to ensure transparency.
Data Extraction
A standardized data extraction sheet was developed and pilot-tested on five studies. Extracted variables included:
-
Bibliographic details (year, country, journal).
-
Clinical domain (neurointervention, peripheral vascular IR, oncology/hepatobiliary IR, intra-radiology).
-
Conflict type (IR vs. DR, IR vs. surgical colleagues, intra-IR).
-
Comparative outcomes (technical success, complication rates, mortality, length of stay, functional outcomes).
-
Referral and workflow dynamics (who initiates referrals, delays in activation, role of tumor boards, or stroke codes).
-
Training and credentialing emphasis (curriculum requirements, imaging literacy, society standards).
-
Society or policy involvement (coding inclusion, reimbursement, advocacy statements).
Data extraction was performed by two reviewers independently, with discrepancies resolved through consensus.
Quality Assessment
Given the heterogeneity of included studies, different tools were used:
-
RCTs: Cochrane Risk of Bias Tool.
-
Cohort/registry studies: Newcastle–Ottawa Scale (NOS).
-
Systematic reviews: AMSTAR-2 checklist.
-
Guidelines/consensus statements: AGREE II instrument.
-
Policy reports and society statements: descriptive appraisal (clarity, stakeholder involvement, applicability).
The majority of outcome-focused RCTs were high quality but only tangentially related to turf conflicts (e.g., thrombectomy trials comparing operators). Registry and cohort studies were generally moderate quality, with limitations including retrospective design and referral biases. Policy documents were variable but valuable for contextualizing society-level perspectives.
Data Synthesis
Because of heterogeneity across study designs, meta-analysis was not feasible. Instead, a narrative thematic synthesis approach was applied. Studies were grouped into five major domains:
-
Neurointervention: including stroke thrombectomy, aneurysm coiling, arteriovenous malformation (AVM) embolization.
-
Peripheral vascular IR: PAD revascularization, chronic limb-threatening ischemia (CLTI), venous disease.
-
Interventional oncology (IO) and hepatobiliary IR: ablation, embolization, radioembolization, biliary interventions.
-
Intra-radiology conflicts: IR versus DR, neuro-IR versus peripheral IR.
-
Society/policy frameworks: credentialing, coding, advocacy, curricula.
Within each domain, quantitative outcomes were summarized where available (e.g., reperfusion rates, patency rates, survival outcomes), whereas qualitative themes (referral control, training debates, coding disputes) were integrated narratively.
Limitations of the Review
Several limitations must be acknowledged:
-
Publication bias: Most studies originated in North America and Europe; representation from low- and middle-income countries (LMICs) was limited.
-
Implicit data: Turf conflicts are often not the explicit subject of publications; many findings had to be inferred from context.
-
Heterogeneity: Study designs varied widely, precluding quantitative pooling.
-
Policy documents: Society statements and advocacy papers are inherently consensus-driven and may reflect organizational bias.
-
Time frame: While the 2000 to 2025 window reflects modern IR practice, earlier historical turf dynamics may not be captured.
Despite these limitations, the methodology provided a structured, reproducible, and transparent synthesis of evidence across diverse sources.
Results
Neurointervention
Stroke Thrombectomy
The advent of mechanical thrombectomy transformed acute ischemic stroke therapy. Pivotal trials such as MR CLEAN, EXTEND-IA, and REVASCAT demonstrated superior outcomes of thrombectomy compared with medical therapy alone. Subsequent registries and real-world data consolidated thrombectomy as standard of care.
A central question in turf disputes is whether outcomes differ depending on operator specialty. Comparative studies and multicenter registries consistently show no significant differences in reperfusion rates, functional independence at 90 days, or mortality between procedures performed by interventional radiologists, neurosurgeons, or neurologists[8]—provided training and credentialing standards are met. Technical success rates (Thrombolysis in Cerebral Infarction (TICI) ≥ 2b) approach 80%, and functional independence (modified Rankin Scale (mRS) ≤ 2 at 90 days) is achieved in approximately 45% of patients, irrespective of operator background.
However, workflow dynamics often create disparities. In many systems, neurologists lead stroke codes and control patient triage, activating IR late in the pathway. This contributes to delays in door-to-puncture time, which strongly predicts outcome. Centers that employ joint activation protocols (neurology and IR activated simultaneously) consistently report reduced treatment delays and improved patient outcomes.[5] Thus, while competence is equivalent, referral governance remains a contested space.
Aneurysm Coiling and Arteriovenous Malformation Embolization
Cerebral aneurysm management illustrates another longstanding turf war. Historically the domain of neurosurgeons, endovascular coiling pioneered by IR challenged open clipping. Comparative studies demonstrate equivalent or superior safety[7] of coiling, with lower perioperative morbidity and shorter hospital stay. Analyses show no outcome inferiority when coiling is performed by IR versus neurosurgeons, provided institutional training and case volumes are adequate.
AVMs provide further examples. Successful embolization depends more on case complexity and center experience than operator background. Registries highlight that outcomes in AVM embolization correlate with institutional volume rather than specialty.[8] Nevertheless, ownership disputes persist, especially in hybrid neurosurgical centers where neurosurgeons increasingly acquire endovascular skills.
Key finding: In neurointervention, operator competence is equivalent across specialties, but referral structures and institutional visibility largely determine turf outcomes.
Peripheral Vascular Interventions
Peripheral Arterial Disease and Chronic Limb-Threatening Ischemia
PAD and CLTI are archetypal battlegrounds between IR and vascular surgery. Historically dominated by open bypass, management shifted with angioplasty and stenting.
Large administrative datasets (e.g., U.S. Medicare analyses) demonstrate that IR-led angioplasty and stenting are associated with:
-
Lower periprocedural morbidity.
-
Shorter hospital stays.[9]
-
Reduced cost compared with surgical bypass.
Long-term patency rates remain broadly equivalent between IR and surgical approaches, although restenosis is more frequent after angioplasty, whereas bypass carries higher perioperative risk.[10] Registry data suggest that center experience and adherence to protocols are stronger determinants of limb salvage than operator background.
High-volume IR programs report limb salvage rates exceeding 80% in CLTI,[11] comparable to surgical outcomes. In some contexts, IR revascularization serves as a bridge to definitive bypass, underscoring potential complementarity rather than competition.[12]
Referral Dynamics and Gatekeeping
Despite equivalent outcomes, IR often plays a secondary role. Vascular surgeons, as admitting physicians for PAD, frequently capture referrals. Consequently, IR is sometimes relegated to salvage cases—occlusions after failed bypass or patients deemed unfit for surgery.
Innovations such as multidisciplinary PAD/wound clinics mitigate these dynamics. When IR and vascular surgery jointly manage patients, referral delays decrease, utilization of minimally invasive options rises, and patient access improves.
Venous Interventions
Venous stenting and embolization (e.g., for May–Thurner syndrome, pelvic congestion) represent newer battlegrounds. IR has historically led these areas, but vascular surgery and cardiology increasingly perform similar interventions. Coding frameworks often list venous procedures under vascular surgery, creating structural disadvantages for IR despite procedural leadership.
Key finding: In peripheral interventions, IR achieves outcomes parity with surgery, but referral capture by vascular surgeons remains decisive in determining visibility and patient flow.
Interventional Oncology and Hepatobiliary Interventional Radiology
Oncologic Interventions
IO has emerged as the fourth pillar of cancer care,[13] alongside surgery, medical oncology, and radiation oncology. Procedures include transarterial chemoembolization (TACE),[14] transarterial radioembolization (TARE), microwave and radiofrequency ablation, and cryoablation.
Randomized trials and consensus statements demonstrate strong evidence:
-
HCC: Ablation achieves survival outcomes equivalent to resection in small tumors (<3 cm), with fewer complications and shorter hospital stays.
-
Colorectal liver metastases: The COLLISION trial confirmed that ablation is noninferior to surgery in selected patients.[15]
-
Radioembolization: Provides disease control in intermediate and advanced HCC,[16] comparable to systemic therapy, with better tolerability.[17]
These results confirm that IR is not merely an adjunct but a frontline oncologic discipline.
Referral Dynamics
Despite outcome parity, IR is often underrepresented in tumor boards. Studies demonstrate that when IR is not present, patients are less likely to be offered ablation or embolization—even when appropriate. Conversely, IR presence in tumor boards increases utilization of minimally invasive oncologic therapies by 25 to 40%.
Hepatobiliary Interventions
Biliary drainage and portal vein embolization highlight additional disputes. Gastroenterologists and hepatobiliary surgeons often dominate these pathways. IR is sometimes consulted only after endoscopic failure, despite evidence of equivalent or superior outcomes with primary percutaneous approaches.
Key finding: In oncology and hepatobiliary IR, evidence supports equivalence or superiority of IR therapies, but underrepresentation in tumor boards leads to systematic underutilization.
Turf Within Radiology
Interventional Radiology versus Diagnostic Radiology
Disputes within radiology reflect concerns about professional identity. DR colleagues question whether IR, in seeking independence, risks diluting its imaging expertise. Conversely, IR practitioners argue that being treated as a “service” under DR undermines clinical legitimacy.
Consensus across societies suggests that 2 to 3 years of dedicated diagnostic imaging training should be integral even in independent IR tracks. This ensures imaging literacy while legitimizing IR as a clinical specialty with longitudinal responsibility.
Neuro-Interventional Radiology versus Peripheral Interventional Radiology
Internal imbalances also exist. Neuro-IR, because of its emergency nature and high visibility, often attracts disproportionate resources, research funding, and conference representation. Peripheral, hepatobiliary, and oncologic IR specialists frequently feel marginalized. These inequities risk fragmenting the specialty unless addressed by societies and training programs.
Key finding: Internal turf wars highlight the importance of balanced training and visibility within IR, preventing dominance by a single subspecialty.
Society and Policy Roles
Professional societies play critical roles in legitimizing IR within health care systems:
-
SIR: Advocates for clinical ownership—outpatient clinics, inpatient admissions, follow-up—as essential to IR identity.
-
CIRSE (Europe): Developed harmonized curricula that integrate both imaging literacy and clinical responsibility.
-
ESR: Explicitly warned of encroachment by nonradiologists performing interventional and diagnostic procedures.
-
ISVIR (India): Campaigns for inclusion of IR-specific codes in national health schemes such as Central Government Health Scheme (CGHS) and Ayushman Bharat, with successes including device-specific approvals (e.g., cyanoacrylate venous closure).
Policy frameworks decisively shape turf outcomes. Coding attribution determines visibility: if a procedure is coded under vascular surgery, IR becomes invisible in reimbursement, regardless of who performs it. Internationally, decisions by Centers for Medicare and Medicaid Services (United States), National Health Service (United Kingdom), and Indian national schemes illustrate how reimbursement frameworks either marginalize or legitimize IR.
Key finding: Societies and policy frameworks are pivotal in shaping turf dynamics, with coding and credentialing functioning as de facto determinants of ownership.
Discussion
Turf Wars as Historical Catalysts in Medicine
The phenomenon of turf wars is not unique to IR. Medical history repeatedly shows that when technological innovations disrupt traditional[2] practices, professional boundaries are contested and redrawn. In the early 20th century, gastroenterology gradually appropriated endoscopy from radiology, arguing that clinical follow-up justified its ownership. Cardiology, initially dependent on radiology for coronary angiography and echocardiography, consolidated these modalities by embedding them into longitudinal patient care. Similarly, orthopaedic surgery and rheumatology clashed over joint interventions. In each case, the specialty that integrated both procedural skill and clinical continuity prevailed.
IR today occupies a similar crossroads. It is one of the most technologically innovative specialties in medicine, with procedures that span nearly every organ system. Yet its relatively young identity and dependence on referrals make it vulnerable to encroachment by more established clinical disciplines. Turf wars in IR, therefore, are not signs of dysfunction but markers of maturation—pressures that will ultimately force the specialty to clarify its scope, standardize training, and embed itself more deeply in patient care.
Outcomes Parity: Evidence versus Perception
Perhaps the most consistent finding across the literature is that outcomes parity exists between IR and competing specialties when training standards are equivalent.[3] [17] Stroke thrombectomy demonstrates this most clearly[8]: reperfusion rates, mortality, and functional independence at 90 days are statistically indistinguishable whether procedures are performed by interventional radiologists, neurosurgeons, or neurologists. Similarly, peripheral revascularization achieves limb salvage rates equivalent to surgical bypass, with lower morbidity and cost. In oncology, ablation for small HCC provides survival outcomes comparable[16] to resection, with fewer complications.
Despite these data, perception often lags behind evidence. Neurologists and neurosurgeons argue that stroke and aneurysms are fundamentally neurological diseases requiring longitudinal follow-up beyond the procedure. Vascular surgeons emphasize their role in comprehensive limb care—from ulcer management to revascularization to amputation. Surgical oncologists and hepatobiliary surgeons point to definitive histology and longitudinal continuity as reasons for controlling oncologic pathways. These perspectives highlight an important truth: in turf wars, perceptions of continuity and accountability often outweigh comparative outcomes.
For IR, this represents both a challenge and an opportunity. Demonstrating procedural competence is necessary but insufficient. Building trust with colleagues and patients requires visible clinical ownership—through outpatient clinics, inpatient admissions, longitudinal follow-up, and proactive participation in multidisciplinary teams.
Referral Dynamics: The True Battleground
Across all domains, the most decisive factor in turf wars is not operator competence but control of referral pathways.
-
Stroke care: In most systems, neurologists lead code stroke activations. If IR is activated only after thrombolysis failure, treatment delays occur, diminishing outcomes. Conversely, when stroke codes activate neurology and IR simultaneously, door-to-puncture times improve and outcomes align with trial benchmarks.
-
PAD: Vascular surgeons, as admitting physicians, often direct patient flow. As a result, IR may see patients only after failed bypass or when surgery is not feasible. Multidisciplinary PAD and wound clinics, where IR and surgery jointly evaluate patients, mitigate this imbalance and improve access to minimally invasive therapies.
-
Oncology: Tumor boards serve as the gateway to cancer treatment. Studies show that when IR is absent from these boards, patients are less likely to be offered embolization or ablation. When IR participates, utilization of minimally invasive therapies increases by 25 to 40%.
-
Hepatobiliary disease: Gastroenterologists and surgeons often dominate biliary drainage and portal vein embolization pathways. IR is sometimes called only after endoscopic approaches fail, despite evidence supporting percutaneous drainage as a primary option in selected cases.
Thus, turf wars are less about technical proficiency and more about who controls the first clinical decision point. Embedding IR into these gateways—stroke codes, PAD clinics, tumor boards, hepatobiliary pathways—is essential for equitable patient access.
Training, Credentialing, and the Dual Identity of Interventional Radiology
Training remains the most sensitive internal issue for IR. Should IR remain within DR or evolve as an independent specialty? DR colleagues worry that independence risks erosion of imaging literacy; IR practitioners fear that remaining under DR reduces them to a technical “service” rather than a clinical discipline.
Consensus across professional societies emphasizes that imaging mastery is non-negotiable.[5] [6] At least 2 to 3 years of dedicated diagnostic training is recommended even in independent IR tracks. Without imaging expertise, procedural safety and appropriateness are compromised. At the same time, IR must cultivate a strong clinical identity: admitting patients, running outpatient clinics, and providing follow-up care.
This dual identity—imaging-based, clinically embedded—is what distinguishes IR from competitors. Surgeons may match IR in procedural competence but lack radiological expertise. Radiologists may interpret imaging but cannot provide therapeutic alternatives. By maintaining both skill sets, IR secures its unique legitimacy.
High-Income versus Low- and Middle-Income Countries
The dynamics of turf wars also vary across health system contexts.
-
High-income countries: Turf disputes often center on coding, reimbursement, and recognition within insurance frameworks. Stroke thrombectomy and oncologic ablation are common battlegrounds.
-
LMICs: Turf conflicts are compounded by resource limitations and workforce shortages. In many LMICs, IR training is less standardized, and nonradiology specialists often dominate procedures by default. At the same time, rapid technology adoption creates opportunities for IR to assert leadership if training frameworks can be developed.
-
Distinct health turf dynamics in LMICs: Turf conflicts in IR acquire a unique dimension in LMICs, where structural, educational, and economic factors differ markedly from high-income settings. Resource scarcity remains the most visible determinant: limited numbers of angiography suites, heterogeneous device availability, and high procedural costs concentrate advanced interventions in a few urban tertiary centers, often in the private sector. Training pathways are another critical source of divergence. Although several fellowship and postdoctoral programs in IR and neurointervention exist, they remain nonuniform and variably accredited. Consequently, trainees admitted from diverse backgrounds—neurology, neurosurgery, or DR—tend to retain their parent specialty identity even after procedural training, perpetuating subtle biases and “cold war” dynamics in multidisciplinary decision-making. This fragmentation is accentuated by an academic–exposure mismatch: institutes of national importance may provide rigorous theoretical and research orientation but limited access to high-end devices, whereas large private hospitals offer abundant procedural exposure without equivalent academic scaffolding. The result is a nonstandardized professional landscape where institutional priorities, financial models, and training pedigrees shape turf perceptions more strongly than comparative outcomes data. At the same time, these challenges create opportunities. The relative newness of IR in LMICs allows flexibility in designing context-specific curricula, society-driven credentialing, and innovative service models that may bypass entrenched hierarchies seen in high-income countries. Recognizing and addressing these distinct systemic dynamics is essential for framing turf disputes in LMICs not merely as limitations but as levers for more inclusive specialty development.
Impact of Turf Disputes on Patient Outcomes and Experience
While interprofessional dynamics often dominate discourse on turf wars, the most critical consequences are borne by patients. Disputes over procedural ownership can directly translate into delays in time-sensitive conditions such as acute ischemic stroke, where contested activation pathways prolong door-to-puncture times and adversely affect functional recovery. In oncology, the absence of interventional radiologists on tumor boards has been shown to reduce patient access to minimally invasive therapies such as ablation or transarterial embolization, thereby limiting treatment options that could lower morbidity and shorten hospitalization. Similarly, fragmented referral structures create confusion for patients, who may encounter inconsistent advice when navigating between neurologists, surgeons, and radiologists, undermining trust in the health system. Beyond clinical outcomes, these disputes also affect the patient experience—delays, duplication of investigations, and contradictory communication erode confidence in care pathways. Importantly, patient-centered framing of solutions—such as joint stroke activation protocols, mandated IR presence in tumor boards, or multidisciplinary PAD clinics—demonstrates how resolving turf disputes can yield tangible improvements in access, safety, and satisfaction. Future work should also include social and operational research using patient- and caregiver-focused surveys or qualitative interviews to capture first-hand perspectives. Such insights would provide an essential counterbalance to professional narratives and ensure that consensus-building efforts remain anchored in patient benefit rather than disciplinary advantage.
The Role of Professional Societies and Policy Frameworks
Professional societies play a decisive role in shaping turf outcomes.
-
SIR: Advocates for clinical ownership, emphasizing OPDs, admissions, and longitudinal follow-up as essential to IR identity.
-
CIRSE: Published harmonized curricula to ensure IR practitioners are trained in both diagnostic imaging and clinical care.
-
ESR: Explicitly warned against encroachment by non-radiologists performing both diagnostic and interventional procedures.
-
ISVIR: Focuses on policy advocacy, lobbying for inclusion of IR-specific codes in national health insurance schemes such as CGHS and Ayushman Bharat. Device-specific coding victories, such as for cyanoacrylate closure of varicose veins, illustrate tangible progress.
Policy frameworks, particularly reimbursement codes, often determine turf outcomes more decisively than scientific data. If a procedure is reimbursed under surgery, IR effectively disappears from administrative visibility, regardless of technical competence. Internationally, CMS in the United States, NHS in the United Kingdom, and Indian national health schemes all illustrate how coding determines legitimacy. Thus, advocacy for coding inclusion is as critical as proving clinical efficacy.
Positive Effects of Turf Wars
Although often portrayed negatively, turf wars can yield positive systemic effects:
-
Training clarity: Disputes force specialties to define curricula and credentialing standards.
-
Registry creation: Stroke, PAD, and oncologic registries often arose in response to interspecialty competition, providing invaluable outcome data.
-
Policy traction: Advocacy for coding and reimbursement gains urgency in the face of encroachment.
-
Collaboration: Turf conflicts often catalyze joint protocols—for example, shared stroke codes or PAD clinics.
-
Visibility: By contesting territory, IR has increased its visibility in multidisciplinary care and public health policy.
Thus, turf wars act as catalysts for growth, pushing the specialty toward greater maturity.
Symmetric Perspectives: A Balanced Lens
To analyze turf wars constructively, it is essential to acknowledge the legitimacy of both sides.
-
IR perspective: Imaging mastery, minimally invasive expertise, early activation, coding recognition, and the ability to reduce morbidity and cost.
-
Surgical/clinical perspective: Longitudinal care, accountability, continuity from diagnosis to definitive management, and concern that episodic IR involvement may fragment care.
Neither perspective is invalid. The challenge is integration rather than dominance. Joint governance structures—shared stroke codes, multidisciplinary PAD clinics, tumor boards with mandated IR presence—provide symmetric solutions. Such integration addresses concerns on both sides while prioritizing patient outcomes.
Delphi Consensus Analogy: Conflict as Structured Dialogue
A useful way to conceptualize turf wars is through the lens of the Delphi consensus method ([Fig. 1]):
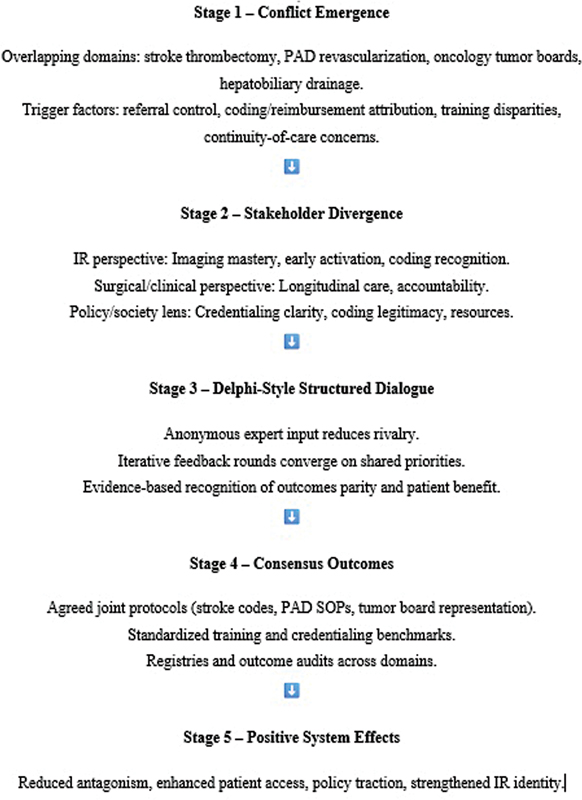
-
Conflict emerges: New procedures blur professional boundaries.
-
Stakeholders diverge: IR emphasizes imaging and minimally invasive access; surgeons/neurologists emphasize longitudinal continuity.
-
Iterative dialogue: Evidence, registries, and society statements progressively clarify the issues.
-
Consensus outcomes: Shared protocols, harmonized training curricula, and joint governance structures emerge ([Table 1]).
-
System matures: Disputes evolve into structured collaboration, improving access, and outcomes.
By reframing turf conflicts as iterative consensus-building processes, the specialty can view them not as threats but as opportunities.
A Practical Roadmap for Building Consensus
-
Establish IR-led outpatient and inpatient services to demonstrate longitudinal patient ownership, strengthen clinical visibility, and reduce reliance on referrals.
-
Mandate IR representation on multidisciplinary platforms such as tumor boards, stroke codes, and PAD clinics to ensure equitable access to minimally invasive therapies.
-
Standardize training and credentialing pathways across diverse backgrounds (radiology, neurology, neurosurgery, surgery) to reduce fragmentation and reinforce unified professional identity.
-
Develop and lead multispecialty registries and outcome audits in areas such as stroke, peripheral vascular disease, and IO, thereby generating robust data for benchmarking and policy advocacy.
-
Engage in targeted advocacy for coding and reimbursement reform, emphasizing that attribution of procedures under IR is critical for visibility, sustainability, and fair resource allocation.
-
Promote joint governance structures where IR collaborates with clinical colleagues in shared protocols, reducing delays and enhancing patient-centered care.
-
Integrate emerging technologies responsibly, with IR taking a leadership role in validating AI and robotics to prevent unregulated diffusion of skills and to enhance system-wide access.
-
Strengthen representation in LMIC contexts, by building society-driven accreditation models, encouraging public–private partnerships, and ensuring resource-sensitive training that bridges academic–exposure mismatches.
-
Foster patient engagement and feedback, including operational research through surveys or qualitative studies, to ensure that reforms are aligned with patient needs rather than disciplinary interests.
|
Domain |
Comparator specialties |
Key outcome measures |
Findings (IR vs. other) |
References |
|---|---|---|---|---|
|
Acute ischemic stroke (mechanical thrombectomy) |
IR vs. neurosurgery vs. neurology |
Successful reperfusion (TICI ≥2b), sICH, 90-d mRS |
Equivalent reperfusion and functional independence across operators when training standardized; workflow efficiency more predictive of outcomes than specialty |
• Shuaib et al., 2022[3] • Society of Interventional Radiology, 2018[5] • Pierot et al., 2019[7] |
|
Intracranial aneurysm coiling |
IR vs. neurosurgery |
Periprocedural complications, rebleeding, retreatment rates |
Comparable safety and efficacy; center volume and case experience stronger predictors of outcomes than specialty |
• Pierot et al., 2019[7] • Spetzler et al., 2015[8] |
|
PAD/CLTI revascularization) |
IR vs. vascular surgery |
Periprocedural morbidity, LOS, mortality, patency, limb salvage |
IR procedures associated with lower morbidity, shorter LOS, reduced cost; long-term patency similar |
• Goodney et al., 2012[9] • Bradbury et al., 2010[10] • Mustapha et al., 2019[11] • Oklu et al., 2016[12] |
|
Hepatocellular carcinoma (TACE/TARE, ablation) |
IR vs. surgical oncology |
Overall survival, recurrence, complications |
IR-based ablation/TACE noninferior to resection in selected HCC; fewer complications and shorter LOS |
• Filippiadis et al., 2017[13] • Llovet et al., 2021[14] • Puijk et al., 2021[15] • Shiina et al., 2012[16] • Sangro et al., 2011[17] |
Abbreviations: HCC, hepatocellular carcinoma; IR, interventional radiology; LOS, length of stay; TACE, transarterial chemoembolization; TARE, transarterial radioembolization.
By consolidating these imperatives into a practical roadmap, turf disputes can be reframed as opportunities to achieve systemic reform, safeguard patient interests, and consolidate IR's position as a clinically embedded, outcomes-driven specialty.
Future Directions
The literature and consensus analysis point toward several imperatives for IR:
-
Embed clinically: IR must run outpatient clinics, admit patients, and provide follow-up to demonstrate longitudinal care.
-
Standardize training: Imaging mastery should remain non-negotiable, whereas curricula emphasize both procedural competence and clinical ownership.
-
Lead registries: Transparent outcome reporting builds trust with colleagues and policymakers.
-
Advocate for coding: Recognition in reimbursement schemes is essential for visibility and sustainability.
-
Promote joint governance: Shared stroke codes, PAD clinics, and tumor boards institutionalize collaboration.
-
Role of emerging technologies, AI, and robotics: AI and robotics will reshape interspecialty boundaries in IR—enhancing triage, expanding access, but also risking diffusion of procedural skills to other fields. Proactive leadership in validation, training, and ethical integration is essential for IR to ensure these technologies strengthen rather than erode its clinical identity.
Conclusion
Turf wars in IR are often perceived as disruptive, but when examined systematically, they represent important markers of specialty maturation. Our review of two decades of evidence demonstrates three consistent themes: first, outcomes parity exists across domains such as stroke thrombectomy, peripheral arterial revascularization, and oncologic ablation when operators are adequately trained; second, referral dynamics—control of patient pathways through stroke codes, PAD clinics, and tumor boards—prove more decisive than technical competence in determining visibility; and third, policy and society frameworks—particularly coding, credentialing, and advocacy—ultimately define structural legitimacy. Importantly, turf disputes have catalyzed positive developments: registries, standardized curricula, outcome audits, and greater visibility of IR in multidisciplinary care ([Table 2]). By applying a Delphi-style consensus lens, these conflicts can be reframed as iterative steps toward integration rather than zero-sum struggles. The path forward requires IR to retain its dual identity—anchored in imaging mastery while fully embedded in clinical practice. Clinical ownership, transparent outcome reporting, and active participation in policy advocacy are essential. Ultimately, the future of IR will not be determined by defending territory, but by demonstrating value through measurable outcomes, collaborative governance, and patient-centered care.
Abbreviations: CIRSE, Cardiovascular and Interventional Radiological Society of Europe; IO, interventional oncology; IR, interventional radiology; PAD, peripheral arterial disease; SIR, Society of Interventional Radiology.
Conflict of Interest
None declared.
Acknowledgments
The author acknowledges the contribution of peer-reviewed literature and professional society guidelines (SIR, CIRSE, ESR, ISVIR) that informed this work.
-
References
- 1 Levin DC, Rao VM, Bonn J. Turf wars in radiology: the battle for peripheral vascular interventions. J Am Coll Radiol 2005; 2 (01) 68-71
- 2 European Society of Radiology 2009. The future role of radiology in healthcare. Insights Imaging 2010; 1 (01) 2-11
- 3 Shuaib A. et al. Outcomes of thrombectomy by different operator specialties. Stroke 2022; 53 (07) 2112-2120
- 4 Brown DB. et al. Impact of IR participation in tumor boards. J Vasc Interv Radiol 2017; 28 (05) 643-650
- 5 Society of Interventional Radiology. Position statement on clinical practice. J Vasc Interv Radiol 2018; 29 (05) 761-767
- 6 CIRSE Standards of Practice Committee. Training curriculum in interventional radiology. Cardiovasc Intervent Radiol 2017; 40 (02) 183-189
- 7 Pierot L. et al. Safety and efficacy of aneurysm coiling. J Neurointerv Surg 2019; 11 (06) 569-574
- 8 Spetzler RF. et al. AVM embolization outcomes. Neurosurgery 2015; 77 (05) 609-618
- 9 Goodney PP. et al. National trends in PAD revascularization. J Vasc Surg 2012; 55 (02) 406-414
- 10 Bradbury AW. et al. Bypass versus angioplasty in severe limb ischemia. Lancet 2010; 376 (9749): 1074-1082
- 11 Mustapha JA. et al. Limb salvage by IR in CLTI. Circ Cardiovasc Interv 2019; 12 (01) e007899
- 12 Oklu R. et al. Imaging-based planning in PAD interventions. J Vasc Interv Radiol 2016; 27 (08) 1151-1157
- 13 Filippiadis DK. et al. Interventional oncology: fourth pillar of cancer care. Cancer Treat Rev 2017; 53: 98-104
- 14 Llovet JM. et al. International consensus on TACE. Hepatology 2021; 73 (01) 314-327
- 15 Puijk RS. et al. COLLISION trial: ablation vs resection. J Clin Oncol 2021; 39 (03) 265-277
- 16 Shiina S. et al. RFA versus resection in small HCC. Hepatology 2012; 57 (05) 1945-1955
- 17 Sangro B. et al. Radioembolization for advanced HCC. Lancet Oncol 2011; 12 (09) 859-868
Address for correspondence
Publication History
Article published online:
26 November 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Levin DC, Rao VM, Bonn J. Turf wars in radiology: the battle for peripheral vascular interventions. J Am Coll Radiol 2005; 2 (01) 68-71
- 2 European Society of Radiology 2009. The future role of radiology in healthcare. Insights Imaging 2010; 1 (01) 2-11
- 3 Shuaib A. et al. Outcomes of thrombectomy by different operator specialties. Stroke 2022; 53 (07) 2112-2120
- 4 Brown DB. et al. Impact of IR participation in tumor boards. J Vasc Interv Radiol 2017; 28 (05) 643-650
- 5 Society of Interventional Radiology. Position statement on clinical practice. J Vasc Interv Radiol 2018; 29 (05) 761-767
- 6 CIRSE Standards of Practice Committee. Training curriculum in interventional radiology. Cardiovasc Intervent Radiol 2017; 40 (02) 183-189
- 7 Pierot L. et al. Safety and efficacy of aneurysm coiling. J Neurointerv Surg 2019; 11 (06) 569-574
- 8 Spetzler RF. et al. AVM embolization outcomes. Neurosurgery 2015; 77 (05) 609-618
- 9 Goodney PP. et al. National trends in PAD revascularization. J Vasc Surg 2012; 55 (02) 406-414
- 10 Bradbury AW. et al. Bypass versus angioplasty in severe limb ischemia. Lancet 2010; 376 (9749): 1074-1082
- 11 Mustapha JA. et al. Limb salvage by IR in CLTI. Circ Cardiovasc Interv 2019; 12 (01) e007899
- 12 Oklu R. et al. Imaging-based planning in PAD interventions. J Vasc Interv Radiol 2016; 27 (08) 1151-1157
- 13 Filippiadis DK. et al. Interventional oncology: fourth pillar of cancer care. Cancer Treat Rev 2017; 53: 98-104
- 14 Llovet JM. et al. International consensus on TACE. Hepatology 2021; 73 (01) 314-327
- 15 Puijk RS. et al. COLLISION trial: ablation vs resection. J Clin Oncol 2021; 39 (03) 265-277
- 16 Shiina S. et al. RFA versus resection in small HCC. Hepatology 2012; 57 (05) 1945-1955
- 17 Sangro B. et al. Radioembolization for advanced HCC. Lancet Oncol 2011; 12 (09) 859-868