

Subscribe to RSS
DOI: 10.1055/s-0045-1814383
Case Report and Review of Literature of Atypical Spindle Cell/Pleomorphic Lipomatous Tumor in the Paratesticular Region
Authors
Funding None.

Abstract
Introduction
The term “atypical spindle cell/pleomorphic lipomatous tumor” was introduced in the WHO Classification of Soft Tissue Tumors in 2020. This tumor is an adipocytic neoplasm of benign or low-grade category, is clinically indolent, has poorly circumscribed margins, and composed of mature adipocytes, lipoblasts, atypical spindle-shaped cells, and multinucleated cells.
Case Report
A 75-year-old male presented with a paratesticular mass. On microscopic examination, the tumor showed a mixture of two components—adipose and fibrous tissue components—which blended with each other along with scattered atypical giant cells. Immunohistochemically, smooth muscle actin showed diffuse positivity in the spindle cells. S100 was negative in the spindle cells and giant cells but was positive in the nuclei of some adipocytes. The Ki-67 index was only 5%. CD34 and desmin were positive in the blood vessel walls—in endothelial cells and muscle layer respectively—and negative in the giant cells. Immunohistochemistry (IHC) with MDM2 (murine double minute 2) and Rb (retinoblastoma) was negative, while CDK4 (cyclin-dependent kinase 4) was variably positive in the nuclei of the spindle cells.
Conclusion
The spectrum of adipocytic tumors that show overlapping morphologic features may pose diagnostic difficulty. Precise diagnosis of ASPLT is important, as it can be misdiagnosed as an intermediate grade or malignant lipomatous tumor. A tumor can be diagnosed as ASPLT when it is composed of a heterogeneous mixture of adipocytes, spindle cells with focal atypia, and multinucleated cells. Lipoblasts are not mandatory for diagnosis. IHC with MDM2, Rb1, Ki67, and molecular testing is helpful in differentiating benign ASPLT from other entities and in ensuring a better prognosis. CDK4 is not found to be useful.
Keywords
adipocytic neoplasm - atypical spindle cell/pleomorphic lipomatous tumor - multinucleated cells - paratesticular - WHO classificationIntroduction
The paratesticular region comprises fat tissue, fibrous tissue, epithelial tissue, mesothelial tissue; therefore, it can give rise to a variety of tumors.[1] Earlier, a subset of adipocytic tumors that showed both spindle cells and pleomorphism could not be included in any of the diagnostic categories of adipocytic tumors.[2] The term “atypical spindle cell/pleomorphic lipomatous tumor (ASPLT)” was introduced to describe such tumors, in the WHO classification of soft tissue tumors, in 2020.[3] [4] This tumor is an adipocytic neoplasm of benign or low-grade category. It is clinically indolent, has poorly circumscribed margins, and is composed of mature adipocytes, lipoblasts, atypical spindle-shaped cells, and multinucleated cells admixed together. This tumor is commonly observed in males ranging from 22 to 68 years, with a mean age of 54 to 63 years.[4] The most common location of this tumor is the limbs and limb girdles, accounting for 63% of cases.[3] Other areas which are rarely involved include the appendix, retroperitoneum, mediastinum, genitals, head and neck, gastric cardia, trachea, larynx, perineum, trunk, and skin.[4] [5] [6] It occurs more frequently in the superficial/subcutaneous plane than in the deep soft tissue.[4] This report describes an ASPLT in an unusual location.
Paratesticular atypical spindle cell lipomatous tumors/pleomorphic lipomatous tumors (ASCLTs or PPLTs) are rare and represent a subset of lipomatous tumors that arise in the paratesticular region. The tumor shows a predilection for male and middle to older age, as in this case.[4] [7] It may be associated with Li-Fraumeni syndrome.[8] [9] Benign tumors of the paratestis include lipoma, leiomyoma, juvenile xanthogranuloma, hemangioma, angiomyxoma, ganglioneuroma, rhabdomyoma, neurofibroma, solitary fibrous tumor, melanotic neuroectodermal tumor (retinal anlage tumor) in the young, desmoplastic small round cell tumor in adolescents, perineuriomas, calcifying fibrous pseudotumor, solitary fibrous tumor, and papillary cyst adenoma.[10] [11] [12] Lipoma is the most common benign tumor of the paratestis.[11] Adenomatoid tumor is a benign tumor of mesothelial origin that can occur in patients of all ages. It can mimic malignant tumor, leading to diagnostic difficulty.[4] [10] [13]
Sarcomas of the genitourinary region constitute 2% of soft tissue sarcomas.[14] Malignant tumors of the paratestis include Wilms' tumor, neuroblastoma, malignant peripheral nerve sheath tumor, rhabdomyosarcoma, yolk sac tumor, malignant mesothelioma, malignant fibrous histiocytoma, liposarcoma, leiomyosarcoma, fibrosarcoma, adenocarcinoma of rete testis, and metastatic tumors. The paratesticular region is the site prone to the development of embryonal rhabdomyosarcoma and embryonal rhabdomyosarcoma is the most common malignant tumor in this region.[10] [11] [13] [14] [15] [16] [17]
The differential diagnoses of an atypical lipomatous tumor include ASPLT, atypical lipomatous tumor, liposarcoma, de-differentiated liposarcoma, fat-forming solitary fibrous tumor, and spindle cell lipoma.[9] [10] [18] Examples for tumor-like lesions of the paratestis include meconium periorchitis, splenic-gonadal fusion, tuberculous epididymitis, epididymal cyst, filarial epididymitis, and fibromatous periorchitis.[10] [11]
Case Report
This manuscript was written after getting consent from the patient and approval from the Institutional Human Ethics Committee. A 75-year-old male presented with a paratesticular mass that had developed over the past 6 months, along with an umbilical hernia, type II diabetes mellitus, and systemic hypertension. The paratesticular swelling was insidious in onset and progressive in nature. He underwent right high inguinal orchiectomy and umbilical hernioplasty. We received a high orchiectomy specimen, with a mass in the paratesticular region measuring 7 × 6 × 2 cm. The outer surface of the tumor was covered with fascia. The cut surface of the tumor was yellow to gray–white in color, smooth and firm in consistency; the margins were pushing, but not infiltrative ([Fig. 1A] and [B]). The testis measured 5 × 3 × 2 cm. The tunica was intact and smooth. The string sign was positive. The testis and the spermatic cord were not adherent to the mass.

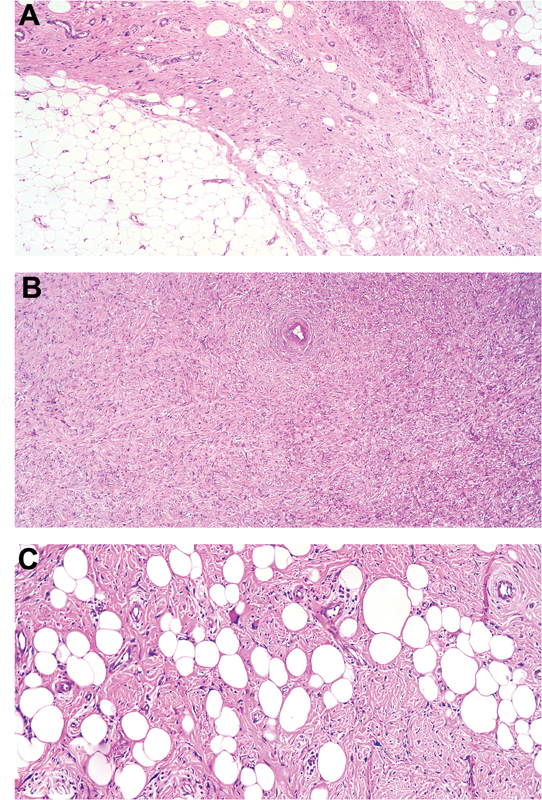
On microscopic examination, the tumor showed a mixture of two components, viz. adipose and fibrous tissue, which were blending with each other ([Fig. 2A]). The adipose tissue was mature and did not show any atypia. The fibrous tissue component comprised of plump spindle-shaped cells arranged in intersecting fascicles and showed no atypia ([Fig. 2B]). Scattered atypical giant cells were present, showing abundant eosinophilic cytoplasm, multinucleation, and multilobation of nuclei ([Fig. 2C]). These nuclei had coarse, clumped chromatin, prominent macronucleoli, and were accompanied by hemosiderin-laden macrophages ([Fig. 3A] and [B]). The fibrous component also showed lymphoid aggregates and lymphoplasmacytic infiltrate at a few foci. No necrosis, lipoblasts, ropey collagen, or floret type giant cells were seen. Both the epididymis and testis were free of tumor. The scrotal tissue showed calcinosis.

Immunohistochemically, smooth muscle actin showed diffuse positivity in the spindle cells ([Fig. 4A]). S100 was negative in the spindle cells and giant cells but positive in the nuclei of some adipocytes ([Fig. 4B]). Ki-67 was positive in 5% of the tumor cells ([Figs. 4C]). CD34 was positive in the endothelial cells of blood vessels and in some spindle cells, but negative in the giant cells ([Fig. 4D]). Desmin was positive in the muscle layer of blood vessels ([Fig. 5A]). MDM2 (murine double minute 2) ([Fig. 5B]) and Rb (retinoblastoma protein) ([Fig. 5C]) were negative. CDK4 (cyclin-dependent kinase 4) ([Fig. 5D]) showed patchy positivity in the nuclei of the spindle cells.


Based on the clinical, gross, microscopic, and immunohistochemical findings, the diagnosis of “ASPLT” was made. The patient was followed up for 11 months with three reviews during which no residual or recurrent tumor was found on clinical examination.
Discussion
Atypical Spindle Cell/Pleomorphic Lipomatous Tumor
ASPLT is a recently described adipocytic tumor that is morphologically low-grade and clinically indolent. It is incorporated in the 5th edition of the WHO Classification of Soft Tissue and Bone Tumors. ASPLT originated from the merging of “atypical spindle cell lipomatous tumor” (ASLT) and ”atypical pleomorphic lipomatous tumor” (APLT).[2]
In the past, atypical spindle cell lipomatous neoplasms were named “spindle cell liposarcoma.” “Spindle cell liposarcomas” were considered as a variant of “atypical lipomatous tumor/well-differentiated liposarcoma” (ALT/WDLS). In the 2002 and 2013 WHO Classification of Soft Tissue and Bone Tumors, “spindle cell liposarcoma” was regarded as a spindle cell variant of ALT/WDLS. With advancements in research, the clinical, histological, and molecular differences between some atypical spindle cell lipomatous neoplasms and ALT/WDLS became clear. Nonetheless, a group of such tumors could not be included under any of the diagnostic categories of adipocytic tumors. In 2017, Mariño-Enriquez et al proposed the term “atypical spindle cell lipomatous tumor” for this group of low-grade adipocytic tumors exhibiting spindle cell features. In the same year, Creytens et al proposed the term “atypical pleomorphic lipomatous tumor” for a group of low-grade pleomorphic adipocytic tumors with a pleomorphic lipoma-like appearance with atypical features. Furthermore, Creytens et al demonstrated morphologic and genetic features that are common to both APLT and ASLT. They suggested that these tumors belong to the same morphologic spectrum and named them as “ASPLT.”[2] The common age of presentation of ASPLT is middle age, though it can occur at any age.
The peak age of incidence is 50 to 60 years. It presents as a nodule in the subcutaneous fat or, less commonly, in the somatic soft tissues. The commonest sites of involvement are the limbs and limb girdles. Rare sites of involvement are head and neck, retro peritoneum, mediastinum, larynx, genital area, trunk, back, appendix, and trachea.[2]
Grossly ASPLTs are generally multinodular and unencapsulated, have ill-defined margins, and may show infiltration into the adjacent tissue. The size of the tumor varies from 0.5 cm to 28 cm.[2] [9] Microscopically, the tumor shows heterogeneous areas within the same lesion and is composed of adipocytes, spindle cells, multinucleated cells, and extracellular matrix. The spindle cells usually show mild focal nuclear atypia. The adipocytes are mature with slight variation in size and shape. Lipoblasts may or may not be present; even when present, they are few in numbers. Lipoblasts are uni-, bi-, or multivacuolated, and have hyperchromatic nuclei, which are sometimes multinucleated. These cells are scattered among the spindle cell or adipocyte components. The stromal component is predominantly collagenous, and may sometimes be myxoid containing “ropey collagen” fibers. Floret-like giant cells are described in the collagenous stroma. Mitotic figures are usually scarce, ranging from 1 to 2 mitotic figures per 50 high-power fields. Tumor necrosis is not found. Rarely, metaplasia is noted in the form of bone, cartilage, and smooth muscle.[2] [5] [7] [19] An interesting finding known as pericytic mimicry, which denotes the significant perivascular location of atypical spindle or pleomorphic cells, has been described in ASPLT, but was not found in our case.[20]
Immunohistochemically, the spindle cells and adipocytes show variable positivity for CD34, S100, and Desmin, and negativity for AE1/AE3, Rb, HMB45, and Melan A. Immunohistochemistry (IHC) for MDM2, CDK4, and p16 is either negative or only slightly reactive.[2] [5] [7] [9] [19] [20] In our case, there was patchy CDK4 positivity in the nuclei of the spindle cells, which was considered inconclusive.
Most cases of ASPLT are associated with loss of Rb1 and absence of MDM2 or CDK4 gene amplification which is detected by fluorescent in situ hybridization (FISH) (fluorescent in situ hybridization) or IHC.[4] [7] [9] The Rb1 gene is a tumor suppressor gene located at the 13q14 locus.[4] [21] FISH and multiplex ligation-dependent probe amplification show deletion in 13q14, including the Rb1, RCTBTB2, DLEU1, ITM2B, and FOXO1 genes. Monosomy 7 has been reported in some cases.[2] [20] [22]
With complete excision, the prognosis is excellent. Local recurrence is common in case of incomplete excision with a recurrence rate of 10 to 15%. Dedifferentiation and metastasis are nearly absent. Therefore, it is important to differentiate ASPLT from ALT/WDLS, which warrants more extensive surgical resection.[2]
Atypical Lipomatous Tumor/Well-Differentiated Liposarcoma
ALT/WDLS is a low-grade malignant tumor that is locally aggressive and can rarely metastasize, recur, or undergo dedifferentiation.[4] [9] [23] [24] It comprises 40 to 45% of all liposarcomas.[25] The clinical behavior of ALT and well-differentiated spindle cell liposarcoma is similar; however, well-differentiated spindle cell liposarcoma is different from ALT, in its pathological and molecular findings. These tumors are considered the atypical counterpart of spindle cell lipoma.[26] Paratesticular liposarcomas account for 12% of all liposarcomas, 3 to 7% of all paratesticular sarcomas, and only less than 200 cases have been reported so far.[27] [28] [29]
The common age of presentation of ALT is >60 years. It is commonly located in the extremities, in deep-seated locations such as retro peritoneum, mediastinum, paratesticular region and the size ranges from 1.5 to 5 cm.[26] [30] [31] MRI can help differentiate lipoma from ALT, with distinguishing features including the presence of T2-weighted signal lesions, contrast enhancement, size >5 cm, non-adipose components within the tumor, and septal thickness >2 mm.[30] In the study by Rauh et al, 40 cases of ALT were studied; six cases had local recurrence after surgery, and no patients developed metastasis. The mean age of presentation of the local recurrence was 15 months after the preceding surgery.[30] Dedifferentiation to dedifferentiated liposarcoma occurs in approximately 10% of patients.[2] [31] Though the large size of the tumor warrants wide resection, severe functional deficits may result, and hence marginal resection is preferred for these cases.[30] ALT and WDLS are identical with respect to morphology and karyotyping, but differ in clinical behavior and surgical resectability.[23] [30]
This tumor is composed of mature adipocytes and shows ill-defined margins, proliferation of spindle cells with mild atypia, lipoblasts, myxoid, or fibrous stroma, with nuclear atypia in adipocytes and stromal cells.[4] [18] [25] [31] Lipoblasts are not mandatory for the diagnosis of ALT/WDLS.[2] [25] Oil Red O can be used to identify them.[31] The phenomenon of pericytic mimicry has also been described in ALT/WDLS.[20]
Nagano et al developed a scoring system to differentiate between lipoma and atypical lipomatous tumor which helps surgeons proceed with marginal resection in suspected cases of ALT.[23] This scoring system is based on the evaluation of parameters such as tumor size, septa, depth, and enhancement on MRI. If the score is greater than or equal to 3, marginal resection of the tumor is recommended.[23]
Immunostaining for MDM2, CDK4, Ki-67, CD34, S100, or FISH is required to differentiate it from benign mimics. Loss of Rb1 gene and absence of MDM2 amplification is observed.[29] [30] [31] WDLS is associated with the amplification of MDM2 and CDK4, which can be demonstrated either by FISH or IHC.[4] [9] [25] [31]
Supernumerary ring chromosomes, also known as giant marker chromosomes or circular macrochromosomes, are present in ALT/WDLS with amplification of the 12q13-15 regions.[2] [20] [25] [31]
Fat-Forming Solitary Fibrous Tumor
Fat-forming solitary fibrous tumor (FFSFT) is a rare variant of solitary fibrous tumor with an indolent clinical course. It manifests commonly in the middle age and typically involves deep soft tissues of retroperitoneum and lower extremities. Rarely it may involve other sites such as the mediastinum, pleura, spine, orbit, or perineum. The morphology of FFSFT is similar to that of conventional SFT, except that it has an adipocytic component. The “staghorn-like” branching blood vessels that are characteristic of SFT are absent in ASPLT. SFTs are characterized by NAB2–STAT6 fusion gene and hence show nuclear STAT6 positivity. ASPLT differs from SFT in the absence of STAT6 expression, deletion of Rb1, and loss of nuclear Rb expression.[2] [9]
Spindle Cell/Pleomorphic Lipoma
Like ASPLT, spindle cell/pleomorphic lipoma (SL/PL) also occurs in the middle age and exhibits a predilection for male patients. The clinical presentation is usually restricted to sites such as subcutaneous fat of the back, shoulder, and neck, whereas the distribution of ASPLT is wider. SL/PL tumors are smaller than ASPLT typically ranging from 4 to 5 cm. They are usually well-circumscribed and often encapsulated with no infiltrative growth pattern. Similar to ASPLT, mature adipocytes, spindle cells, myxoid matrix, floret-like multinucleated cells are seen in SL/PL.
However, SL does not show bizarre pleomorphic cells, atypical spindle cells, or lipoblasts. Ropey collagen fibers are a characteristic feature of SL/PL, and they are not found in ASPLT. CD34 positivity in spindle cells, deletion of Rb1, lack of MDM2, and CDK4 gene amplification are features common to SL/PL and ASPLT.[2] [9] [32]
Conclusion
The 5th edition of the WHO Classification of adipocytic neoplasms has highlighted the spectrum of adipocytic tumors composed of spindle cells, giant cells, adipocytes, which show morphologic overlap and hence pose diagnostic challenges. This article presents a recently described tumor occurring in an unusual location. This ASPLT has not been reported in the paratesticular region in the literature, so far. This is the first article to describe this tumor in this location. Precise diagnosis of ASPLT is important, as it is likely to be misdiagnosed as an intermediate grade or malignant lipomatous tumor. Although immunohistochemical evaluation was done and a final diagnosis could be made, molecular tests could not be done in this case due to financial constraints. This is considered a limitation of this study.
IHC for MDM2, Rb1, Ki67 and molecular testing such as FISH or Karyotyping is helpful in cases with indeterminate morphology to differentiate benign ASPLT from other lipomatous tumors, whereas CDK4 is not considered a useful marker.
Conflict of Interest
None declared.
Acknowledgment
The author thanks the technicians of Histopathology Laboratory of Chettinad Hospital and Research Institute for preparing this case.
Patient's Consent
This article was written after obtaining written consent from the patient.
-
References
- 1 Unlü Y, Huq GE, Ozyalvaçli G. et al. Paratesticular sarcomas: a report of seven cases. Oncol Lett 2015; 9 (01) 308-312
- 2 Lecoutere E, Creytens D. Atypical spindle cell/pleomorphic lipomatous tumor. Histol Histopathol 2020; 35 (08) 769-778
- 3 Choi JH, Ro JY. The 2020 WHO Classification of Tumors of Soft Tissue: selected changes and new entities. Adv Anat Pathol 2021; 28 (01) 44-58
- 4 Memon R, Abdelfatah MM, Patel C. et al. Atypical spindle cell/pleomorphic lipomatous tumor of the stomach: a case report. Hum Pathol: Case Rep 2021; 25: 200540
- 5 Tchack MS, Broscius M, Reichel M. Primary Cutaneous Atypical Spindle Cell Lipomatous Tumor. Hindawi Case Reports in Pathology 2021; 4082289
- 6 Manganaro PMJ, Troncoso PM, Echavarría Cadena CA. et al. Atypical spindle cell lipomatous tumor of the perineum. Radiol Case Rep 2025; 21 (01) 158-163
- 7 Rodrigues E, Cardoso F, Scigliano H, Nora M. An atypical pleomorphic lipomatous tumor presenting as groin mass. Cureus 2021; 13 (11) e19410
- 8 Perret R, Charville GW, Alame M. et al. Atypical spindle cell/pleomorphic lipomatous tumor with sarcomatous transformation: clinicopathologic and molecular analysis of 4 cases. Mod Pathol 2024; 37 (04) 100454
- 9 Bahadır B, Behzatoğlu K, Hacıhasanoğlu E, Koca SB, Sığırcı BB, Tokat F. Atypical spindle cell/pleomorphic lipomatous tumor: a clinicopathologic, immunohistochemical, and molecular study of 20 cases. Pathol Int 2018; 68 (10) 550-556
- 10 Ulbright TM, Young RH. Testicular and paratesticular tumors and tumor-like lesions in the first 2 decades. Semin Diagn Pathol 2014; 31 (05) 323-381
- 11 Khandeparkar SGS, Pinto RGW. Histopathological spectrum of tumor and tumor-like lesions of the paratestis in a tertiary care hospital. Oman Med J 2015; 30 (06) 461-468
- 12 Barazani Y, Tareen B. Rare case of paratesticular solitary fibrous tumour (lipomatous hemangiopericytoma). Can Urol Assoc J 2012; 6 (03) E131-E133
- 13 Abell MR, Holtz F. Testicular and paratesticular neoplasms in patients 60 years of age and older. Cancer 1968; 21 (05) 852-870
- 14 Khandekar MJ, Raut CP, Hornick JL, Wang Q, Alexander BM, Baldini EH. Paratesticular liposarcoma: unusual patterns of recurrence and importance of margins. Ann Surg Oncol 2013; 20 (07) 2148-2155
- 15 Coppes MJ, Rackley R, Kay R. Primary testicular and paratesticular tumors of childhood. Med Pediatr Oncol 1994; 22 (05) 329-340
- 16 Huddart R, Hazell S, Horwich A. Rare Tumors of the testis and paratesticular tissues. In: Raghavan D, Blanke CD, Johnson DH, Moots PL, Reaman GH, Rose PG. et al., eds. Textbook of Uncommon Cancer. 1st ed.. Wiley; 2012: 77-96
- 17 Amin MB. Selected other problematic testicular and paratesticular lesions: rete testis neoplasms and pseudotumors, mesothelial lesions and secondary tumors. Mod Pathol 2005; 18 (Suppl. 02) S131-S145
- 18 Mariño-Enriquez A, Nascimento AF, Ligon AH, Liang C, Fletcher CDM. Atypical spindle cell lipomatous tumor: clinicopathologic characterization of 232 cases demonstrating a morphologic spectrum. Am J Surg Pathol 2017; 41 (02) 234-244
- 19 Zhang Z, Liu N, Chen M, Peng R, Chen HJ, Zhang HY. Atypical spindle cell lipomatous tumor/atypical pleomorphic lipomatous tumor and atypical mammary-type myofibroblastoma: clinicopathological, immunohistochemical, and multiplex fluorescence in situ hybridization analyses. Chin Med J (Engl) 2021; 134 (19) 2370-2372
- 20 Creytens D, Mentzel T, Ferdinande L, van Gorp J, Van Dorpe J, Flucke U. “Fat-rich” (spindle cell-poor) variant of atypical spindle cell/pleomorphic lipomatous tumor: striking mimic of “classical” atypical lipomatous tumor/well-differentiated liposarcoma. Int J Surg Pathol 2019; 27 (08) 868-871
- 21 Creytens D, Mentzel T, Ferdinande L. et al. "Atypical" pleomorphic lipomatous tumor: a clinicopathologic, immunohistochemical and molecular study of 21 cases, emphasizing its relationship to atypical spindle cell lipomatous tumor and suggesting a morphologic spectrum (atypical spindle cell/pleomorphic lipomatous tumor). Am J Surg Pathol 2017; 41 (11) 1443-1455
- 22 Nishio J, Nakayama S, Chijiiwa Y, Koga M, Aoki M. Atypical spindle cell/pleomorphic lipomatous tumor: a review and update. Cancers (Basel) 2024; 16 (18) 3146
- 23 Nagano S, Yokouchi M, Setoguchi T. et al. Differentiation of lipoma and atypical lipomatous tumor by a scoring system: implication of increased vascularity on pathogenesis of liposarcoma. BMC Musculoskelet Disord 2015; 16 (01) 36
- 24 Burasapat C, Wongprakob N, Wanichjaroen N, Pruksapong C, Satayasoontorn K. Atypical Lipomatous Tumor/Well-Differentiated Liposarcoma with Intramuscular Lipoma-Like Component of the Thigh. Hindawi Case Reports in Surgery 2020; 8846932
- 25 Peck T, Gervasio KA, Zhang PJL. et al. Atypical lipomatous tumor/well-differentiated liposarcoma with myxoid stroma in a hereditary retinoblastoma survivor. Ocul Oncol Pathol 2020; 6 (02) 79-86
- 26 Mentzel T, Palmedo G, Kuhnen C. Well-differentiated spindle cell liposarcoma (‘atypical spindle cell lipomatous tumor’) does not belong to the spectrum of atypical lipomatous tumor but has a close relationship to spindle cell lipoma: clinicopathologic, immunohistochemical, and molecular analysis of six cases. Mod Pathol 2010; 23 (05) 729-736
- 27 Schoonjans C, Servaes D, Bronckaers M. Liposarcoma scroti: a rare paratesticular tumor. Acta Chir Belg 2016; 116 (02) 122-125
- 28 Mouden K, Wakrim S, Semmar A. Paratesticular liposarcoma: a case report. Pan Afr Med J 2019; 33: 282
- 29 Vinayagam K, Hosamath V, Honnappa S, Rau AR. Paratesticular liposarcoma-masquerading as a testicular tumour. J Clin Diagn Res 2014; 8 (02) 165-166
- 30 Rauh J, Klein A, Baur-Melnyk A. et al. The role of surgical margins in atypical lipomatous tumours of the extremities. BMC Musculoskelet Disord 2018; 19 (01) 152
- 31 Zhan H, Cao S, Gao T. et al. Giant atypical lipomatous tumor/well-differentiated liposarcoma affects lower limb activity: a case report. Medicine (Baltimore) 2019; 98 (42) e17619
- 32 Ohshima Y, Nishio J, Nakayama S, Koga K, Aoki M, Yamamoto T. Spindle cell lipoma and pleomorphic lipoma: an update and review. Cancer Diagn Progn 2023; 3 (03) 282-290
Address for correspondence
Publication History
Article published online:
24 December 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Unlü Y, Huq GE, Ozyalvaçli G. et al. Paratesticular sarcomas: a report of seven cases. Oncol Lett 2015; 9 (01) 308-312
- 2 Lecoutere E, Creytens D. Atypical spindle cell/pleomorphic lipomatous tumor. Histol Histopathol 2020; 35 (08) 769-778
- 3 Choi JH, Ro JY. The 2020 WHO Classification of Tumors of Soft Tissue: selected changes and new entities. Adv Anat Pathol 2021; 28 (01) 44-58
- 4 Memon R, Abdelfatah MM, Patel C. et al. Atypical spindle cell/pleomorphic lipomatous tumor of the stomach: a case report. Hum Pathol: Case Rep 2021; 25: 200540
- 5 Tchack MS, Broscius M, Reichel M. Primary Cutaneous Atypical Spindle Cell Lipomatous Tumor. Hindawi Case Reports in Pathology 2021; 4082289
- 6 Manganaro PMJ, Troncoso PM, Echavarría Cadena CA. et al. Atypical spindle cell lipomatous tumor of the perineum. Radiol Case Rep 2025; 21 (01) 158-163
- 7 Rodrigues E, Cardoso F, Scigliano H, Nora M. An atypical pleomorphic lipomatous tumor presenting as groin mass. Cureus 2021; 13 (11) e19410
- 8 Perret R, Charville GW, Alame M. et al. Atypical spindle cell/pleomorphic lipomatous tumor with sarcomatous transformation: clinicopathologic and molecular analysis of 4 cases. Mod Pathol 2024; 37 (04) 100454
- 9 Bahadır B, Behzatoğlu K, Hacıhasanoğlu E, Koca SB, Sığırcı BB, Tokat F. Atypical spindle cell/pleomorphic lipomatous tumor: a clinicopathologic, immunohistochemical, and molecular study of 20 cases. Pathol Int 2018; 68 (10) 550-556
- 10 Ulbright TM, Young RH. Testicular and paratesticular tumors and tumor-like lesions in the first 2 decades. Semin Diagn Pathol 2014; 31 (05) 323-381
- 11 Khandeparkar SGS, Pinto RGW. Histopathological spectrum of tumor and tumor-like lesions of the paratestis in a tertiary care hospital. Oman Med J 2015; 30 (06) 461-468
- 12 Barazani Y, Tareen B. Rare case of paratesticular solitary fibrous tumour (lipomatous hemangiopericytoma). Can Urol Assoc J 2012; 6 (03) E131-E133
- 13 Abell MR, Holtz F. Testicular and paratesticular neoplasms in patients 60 years of age and older. Cancer 1968; 21 (05) 852-870
- 14 Khandekar MJ, Raut CP, Hornick JL, Wang Q, Alexander BM, Baldini EH. Paratesticular liposarcoma: unusual patterns of recurrence and importance of margins. Ann Surg Oncol 2013; 20 (07) 2148-2155
- 15 Coppes MJ, Rackley R, Kay R. Primary testicular and paratesticular tumors of childhood. Med Pediatr Oncol 1994; 22 (05) 329-340
- 16 Huddart R, Hazell S, Horwich A. Rare Tumors of the testis and paratesticular tissues. In: Raghavan D, Blanke CD, Johnson DH, Moots PL, Reaman GH, Rose PG. et al., eds. Textbook of Uncommon Cancer. 1st ed.. Wiley; 2012: 77-96
- 17 Amin MB. Selected other problematic testicular and paratesticular lesions: rete testis neoplasms and pseudotumors, mesothelial lesions and secondary tumors. Mod Pathol 2005; 18 (Suppl. 02) S131-S145
- 18 Mariño-Enriquez A, Nascimento AF, Ligon AH, Liang C, Fletcher CDM. Atypical spindle cell lipomatous tumor: clinicopathologic characterization of 232 cases demonstrating a morphologic spectrum. Am J Surg Pathol 2017; 41 (02) 234-244
- 19 Zhang Z, Liu N, Chen M, Peng R, Chen HJ, Zhang HY. Atypical spindle cell lipomatous tumor/atypical pleomorphic lipomatous tumor and atypical mammary-type myofibroblastoma: clinicopathological, immunohistochemical, and multiplex fluorescence in situ hybridization analyses. Chin Med J (Engl) 2021; 134 (19) 2370-2372
- 20 Creytens D, Mentzel T, Ferdinande L, van Gorp J, Van Dorpe J, Flucke U. “Fat-rich” (spindle cell-poor) variant of atypical spindle cell/pleomorphic lipomatous tumor: striking mimic of “classical” atypical lipomatous tumor/well-differentiated liposarcoma. Int J Surg Pathol 2019; 27 (08) 868-871
- 21 Creytens D, Mentzel T, Ferdinande L. et al. "Atypical" pleomorphic lipomatous tumor: a clinicopathologic, immunohistochemical and molecular study of 21 cases, emphasizing its relationship to atypical spindle cell lipomatous tumor and suggesting a morphologic spectrum (atypical spindle cell/pleomorphic lipomatous tumor). Am J Surg Pathol 2017; 41 (11) 1443-1455
- 22 Nishio J, Nakayama S, Chijiiwa Y, Koga M, Aoki M. Atypical spindle cell/pleomorphic lipomatous tumor: a review and update. Cancers (Basel) 2024; 16 (18) 3146
- 23 Nagano S, Yokouchi M, Setoguchi T. et al. Differentiation of lipoma and atypical lipomatous tumor by a scoring system: implication of increased vascularity on pathogenesis of liposarcoma. BMC Musculoskelet Disord 2015; 16 (01) 36
- 24 Burasapat C, Wongprakob N, Wanichjaroen N, Pruksapong C, Satayasoontorn K. Atypical Lipomatous Tumor/Well-Differentiated Liposarcoma with Intramuscular Lipoma-Like Component of the Thigh. Hindawi Case Reports in Surgery 2020; 8846932
- 25 Peck T, Gervasio KA, Zhang PJL. et al. Atypical lipomatous tumor/well-differentiated liposarcoma with myxoid stroma in a hereditary retinoblastoma survivor. Ocul Oncol Pathol 2020; 6 (02) 79-86
- 26 Mentzel T, Palmedo G, Kuhnen C. Well-differentiated spindle cell liposarcoma (‘atypical spindle cell lipomatous tumor’) does not belong to the spectrum of atypical lipomatous tumor but has a close relationship to spindle cell lipoma: clinicopathologic, immunohistochemical, and molecular analysis of six cases. Mod Pathol 2010; 23 (05) 729-736
- 27 Schoonjans C, Servaes D, Bronckaers M. Liposarcoma scroti: a rare paratesticular tumor. Acta Chir Belg 2016; 116 (02) 122-125
- 28 Mouden K, Wakrim S, Semmar A. Paratesticular liposarcoma: a case report. Pan Afr Med J 2019; 33: 282
- 29 Vinayagam K, Hosamath V, Honnappa S, Rau AR. Paratesticular liposarcoma-masquerading as a testicular tumour. J Clin Diagn Res 2014; 8 (02) 165-166
- 30 Rauh J, Klein A, Baur-Melnyk A. et al. The role of surgical margins in atypical lipomatous tumours of the extremities. BMC Musculoskelet Disord 2018; 19 (01) 152
- 31 Zhan H, Cao S, Gao T. et al. Giant atypical lipomatous tumor/well-differentiated liposarcoma affects lower limb activity: a case report. Medicine (Baltimore) 2019; 98 (42) e17619
- 32 Ohshima Y, Nishio J, Nakayama S, Koga K, Aoki M, Yamamoto T. Spindle cell lipoma and pleomorphic lipoma: an update and review. Cancer Diagn Progn 2023; 3 (03) 282-290