

Subscribe to RSS
DOI: 10.1055/s-0046-1816044
The Current Landscape of Nanopaclitaxel Formulations and the Benefits of Polymeric Micellar Paclitaxel in Solid Tumors
Authors
Funding Funding for medical writing support was provided by Lupin Ltd.

Abstract
The tumor microenvironment (TME) creates a complex biochemical and physical barrier affecting the penetration of chemotherapeutic agents into the tumor. Nanotherapy, which allows targeted drug delivery, has generated considerable interest in recent times to overcome the limitations of conventional chemotherapeutics and target the TME. The therapeutic efficacy of nanoformulations is significantly influenced by the particle size. Paclitaxel (PTX) is one of the most effective chemotherapeutic drugs for solid tumors, but its major limitation is its low water solubility. Its organic solvent formulation (Taxol) is known to cause severe toxicity. Therefore, various PTX nanoformulations have been developed using carriers, such as albumin, liposomes, and polymeric micelles. Each carrier has specific characteristics that offer some advantages and also lead to some limitations. There is scarce literature on the comparative profiles of the various types of PTX nanoformulations. Polymeric micelles that are smaller than 100 nm have acquired considerable attention due to their unique structure and high-loading capacity. Currently, there is only one approved and marketed formulation of polymeric micellar PTX (Genexol-PM). Over the years since preclinical evaluation, 22 studies on Genexol-PM in various solid tumors have been published, making it the most widely studied polymeric micellar PTX, demonstrating its safety, efficacy, and higher maximum tolerated dose compared to the conventional formulations. However, many of these were phase 2 trials, and studies on the available liposomal PTX formulations are scarce. There is a need for more PTX nanoformulations with different carriers, and more phase 3 and phase 4 studies on the available PTX nanoformulations. Moreover, head-to-head studies comparing the outcomes of various PTX nanoformulations are necessary to help clinicians make an informed decision when choosing nano PTX for their patients.
Introduction
The tumor microenvironment (TME) includes immune cells, endothelial and inflammatory cells, fibroblasts, and lymphocytes, along with extracellular matrix (ECM), stroma, and vasculature.[1] Besides promoting the growth of tumor cells, tumor invasion, and metastasis, the TME also influences therapeutic efficacy and drug tolerance.[2] [3] It creates a complex biochemical and physical barrier, limiting the conventional chemotherapeutic agents from entering the tumor.[2] The barrier can also aggravate drug resistance by protecting pro-proliferation factors in the TME and tumor mass.[1] [4]
In addition to drug resistance TME also causes nonspecific distribution of chemotherapeutic drugs in normal tissues.[2] Nanotherapy has generated considerable interest in recent times to overcome the limitations of conventional chemotherapeutics and target the TME.[5] [6] Nanoparticles allow targeted drug delivery and release in the TME.[7] [8] [9] They modulate major TME components and increase the retention time of drugs in the tumor. Hence, they can be used as passive drug delivery platforms. Furthermore, they can be actively targeted to tumor tissues by altering their structure and conjugating them to specific ligands.[10] [11] By adapting the size and shape of nanocarriers, their permeability in tumor tissues can be improved.[2]
The differential deposition of nanoparticles in tumor tissues leads to a higher concentration of the drug in the tumor than in the plasma or other organs.[12] Nanoparticles can also solubilize hydrophobic drugs and have better pharmacokinetics and biocompatibility. With controlled drug release in response to external stimuli and the ability to reach specific targets, the overall efficacy is considerably improved.[13] Nanocarriers directly reach the targeted area through the bloodstream. Solid tumors have a leaky vasculature structure and poor lymphatic drainage. With their small size, nanocarriers can escape from the leaky vasculature overlying the tumor and accumulate preferentially in the tumor tissue. The blocked lymphatics retain the nanoparticles within the tumor.[14] This enhanced permeability and retention (EPR) effect improves drug accumulation inside the tumor. On accumulation, the nanoparticles induce DNA damage through the overproduction of reactive oxygen species (ROS). This may finally lead to apoptosis and the death of tumor cells.[12] However, the lymphatic drainage of nanoparticles and their therapeutic efficacy are significantly influenced by the particle size. Large particles can get entrapped in the ECM, preventing them from further penetration. In contrast, small particles precipitously diffuse out of lymph nodes and have a limited effect on immune responses.[3] [15] [16] [17] Nanoparticles with a size of 20 to 50 nm can penetrate the ECM more easily than larger particles and are better suited to withstand high interstitial pressure.[18] [19] [20]
Paclitaxel (PTX) is one of the most effective chemotherapeutic drugs and is usually used for solid tumors such as lung cancer, ovarian cancer, breast cancer, and others.[21] [22] [23] [24] It is a mitotic inhibitor and has a high therapeutic efficacy against several solid tumors.[25] However, its major limitation is its low water solubility. Hence, it was formulated in organic solvents such as Cremophor EL (CrEL) and dehydrated ethanol (50/50, v/v) under the trademark “Taxol.”[21] However, CrEL has significant dose-limiting neurotoxic adverse effects and hypersensitivity.[25] Moreover, CrEL modifies the pharmacokinetic profile of PTX in vivo to unpredictable nonlinear plasma pharmacokinetics.[25] [26] [27] Therefore, alternative PTX nanoformulations have been developed to minimize or overcome these limitations.[14]
While several types of non–albumin-based nanoformulations of PTX are available, there is scarce literature on the comparative benefits and disadvantages of the different types. Although there are no head-to-head studies comparing the various PTX nanoformulations, this article aims to provide a comparative narrative for the benefit of clinicians. We discuss the key physical features of each type of nanoformulation, the benefits and drawbacks of each, and the currently marketed and approved PTX nanoformulations. Since polymeric micelles are the smallest nanoparticles, this article discusses polymeric micellar PTX in more detail.
Types of Nanoformulations
Nanoformulations can be prepared using various nanoplatforms, such as solid lipid nanoparticles, liposomes, nanoemulsions, polymer–drug conjugates, polymeric micelles, gold nanoparticles, carbon nanotubes, protein nanoparticles, metal-organic frameworks, and covalent organic frameworks.[28] [29] [30] [31] Each platform has specific characteristics that make it advantageous for some types of uses, while creating limitations for others.[12] Different factors, such as physical and biological stability, manufacturing method, scale-up possibility, freeze-drying conditions, and sterilization requirements, can influence the effectiveness of nanomedicine in drug delivery. The biocompatibility, biodegradability, and non-immunogenicity of nanoformulations play important roles in effective therapeutic delivery, better bioavailability, and reduced adverse effects.[29] [32] [33] Nanoparticles smaller than 100 nm but larger than 10 nm are optimal for tumor penetration.[34] However, the biggest challenge in the development of nanoparticle therapeutics is long-term stability. Nanoparticles often exhibit physical and chemical instability. Lyophilization, also known as freeze-drying, has been explored as a key solution for increasing stability. Lyophilization also increases the shelf life, ensuring safer storage and transportation of drug-loaded nanoparticles.[35] [36] [37]
Lipids and polymers (polymeric micelles) are the most commonly used materials for preparing biocompatible and biodegradable nanoparticles.[32] Liposome-based lipid nanoparticles do not provide control over the time of drug release, and, in most cases, do not achieve effective intracellular delivery of the drug molecules. Thus, their potential to be useful against multidrug-resistant cancers is limited.[34] Since they have to be made manually, they can be difficult to synthesize. The manual loading of liposomes is also difficult; hence, they are not as readily available as other systems of drug delivery. Another challenge is the size of liposomes, which is usually more than 100 nm. Moreover, while liposomes have been relatively nontoxic, anticancer liposomes containing cytotoxic agents have shown indirect signs of macrophage destruction.[38] [39]
Solid lipid nanoparticles can incorporate both hydrophobic and hydrophilic drugs, and the particle size ranges from 70 to 300 nm, depending on the specific formulation.[40] They can provide improved drug stability (through the use of co-emulsifiers and co-surfactants), enhanced drug delivery, better drug absorption, and biocompatibility. Other advantages over conventional drug delivery systems include biocompatibility and biodegradability, versatile route of administration, enhanced stability, and low toxicity.[40] They can also be administered through various routes and allow controlled drug release.[41] Despite these advantages, there are major barriers to their successful clinical use. During the manufacturing process, solid lipid nanoparticles can undergo polymorphic changes within the lipid matrices, leading to drug expulsion and loss of therapeutic efficacy.[40] Another concern is surfactant-related toxicity and unresolved long-term safety risks.[40]
Polymeric Micelles as Nanoparticles
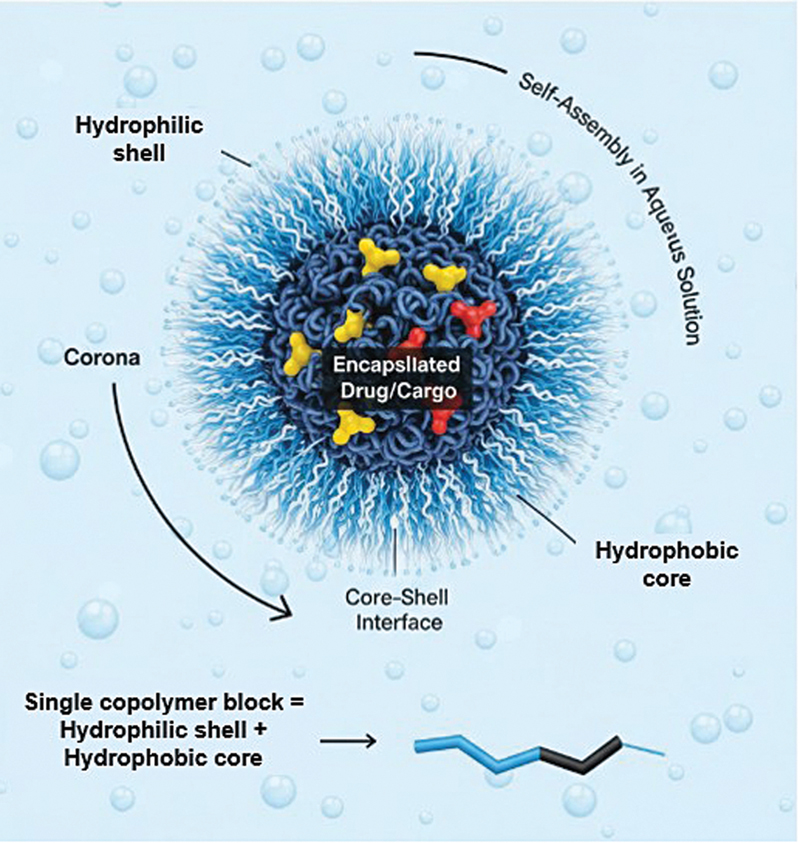
A polymeric micelle usually contains hundreds of block copolymers and has a diameter of 20 to 50 nm. It has two spherical concentric regions—a densely packed core consisting of hydrophobic blocks and a hydrophilic shell consisting of a dense brush of poly(ethylene oxide) ([Fig. 1]). Hydrophobic drugs can be physically integrated within the core of the polymeric micelle.[42] [43] Polymeric micelles have acquired considerable attention due to their unique structure and high-loading capacity.[25] Since they are smaller than 100 nm, they accumulate more easily in tumors compared to the liposomes.[34] The small size also enables extravasation from blood vessels into the tumor tissue.[43] Furthermore, the small size allows them to escape clearance in the liver and kidneys. They can evade the mononuclear phagocytic system in the liver, and their optimal size also precludes them from renal clearance. Thus, they remain in circulation in the bloodstream for a long time.[13]
The hydrophilic compartment for the copolymer is poly(ethylene glycol) (PEG). PEG is hydrophilic, nonionic, biocompatible, inert to many organic compounds, has low toxicity, and protects the drugs from enzymatic degradation.[13] [43] The hydrophilic shell of the micelle prevents a quick uptake by the reticuloendothelial system (RES), thereby prolonging the circulation time in the body.[43] Various polymers such as poly(propylene glycol) (PPG), poly(caprolactone) (PCL), poly(L-lactide) (PLA), poly(propylene oxide) (PPO), poly(D,L-lactic acid) (PDLLA), poly(L-aspartate), and poloxamers have been used as hydrophobic compartments.[13] [43] The type and molecular weight of the hydrophobic block define the stability of polymeric micelles. The hydrophobic block should have a high drug-loading capacity and good compatibility of the core with the incorporated drug.[43]
Currently Approved and Marketed Nano PTX Formulations
Nanoparticle human-albumin-bound PTX (Abraxane) was the first nanoformulation developed to address the toxicity caused by CrEL-based PTX formulations. Abraxane is a nanoparticle colloidal suspension, formed by homogenizing PTX with human serum albumin under high pressure.[44] The albumin-PTX particle is approximately 130 nm in diameter.[45] Compared to Taxol, Abraxane has advantages, such as lower infusion volume and a shorter time required for administration (30–40 minutes), no need for premedication, and no need for special infusion sets (bag, tubing, and in-line filters).[14] However, it has been associated with a significant decrease in white blood cells, red blood cells, and allergic reactions.[46] There are other challenges associated with albumin-bound nanoparticles. Albumin can react with blood protein, leading to a decrease in the number of nanoparticles entering the tumor tissue. Moreover, albumin is not adequately stable due to its structural properties amid the complex body milieu containing various enzymes and proteins.[47] Hence, nanoformulations using other carriers have been developed.
Other than albumin, PTX has been formulated in various nanodelivery systems, such as liposomes, polymeric micelles, and polymeric conjugates.[14] The aqueous solubility of PTX is considerably increased when it is conjugated with water-soluble polymers. These polymers are small in size, which facilitates the preferential delivery of PTX into the tumor site due to the EPR effect, as explained earlier. In healthy tissues, they remain undetected by RES, thereby reducing the side effects of the drug. Hence, higher maximum tolerated doses (MTDs) are realized.[21]
The currently marketed formulations of nano PTX are shown in [Table 1]. Of these, Abraxane and Genexol PM are lyophilized products approved for storage at 25°C ± 2°C, while Nanoxel is a liquid formulation approved for storage at 2 to 8°C.[48] Lyophilization details of other formulations are not available. Some formulations require dextrose for administration (Bevetex, Nanoxel), which can make it challenging to use them for patients with diabetes. Some others require special filters (Pazenir, Nanoxel) or special IV sets (Nanoxel).
|
Formulation |
Countries approved in |
Nanocarrier used |
Particle size |
Administration |
Brand formulation |
Manufacturer |
Approved indication |
Regulatory approval year |
|---|---|---|---|---|---|---|---|---|
|
USFDA/India |
Colloidal suspension without solvent of paclitaxel bound to albumin in the form of spherical nanoparticles Albumin-bound nanoparticles; lyophilized for room temperature storage[7] |
130 nm |
900 mg human albumin for reconstitution |
Paclitaxel protein-bound particles for injectable suspension 100 mg |
Abraxis Biosciences Inc. |
Metastatic breast cancer Locally advanced or metastatic non-small cell lung cancer (NSCLC) Metastatic adenocarcinoma of the pancreas India: for treatment of breast cancer after failure of combination chemo for metastatic disease or relapse within 6 mo of adjuvant chemotherapy |
2005/2008 India |
|
|
South Korea. China |
Emulsion |
187 nm[56] |
Prepared as a semi-solid wax that melts at approximately 30°C and administered orally[57] |
Liporaxel (oral paclitaxel based on a novel lipid formulation) |
Daehwa Pharmaceutical |
treatment of gastric cancer |
2016 (SA) 2024 (China) |
|
|
European Union |
Albumin-bound nanoparticles. Needs to be stored below 25°C[58] |
130 nm |
Requires 20 mL of sodium chloride (0.9%) solution for reconstitution and 15 µm filter for administration through IV set[58] |
Generic version of Abraxane |
Ratio-pharma GmbH |
Metastatic breast cancer, Met adenocarcinoma of the pancreas, non-small cell lung cancer |
2019 |
|
|
Bevetex[50] |
India |
Polymeric-lipid nanodispersion |
50–150 nm |
Dextrose; administered using a regular IV set |
Injection concentrate for nanodispersion 100 mg/300 mg |
Sun Pharma Laboratories Ltd. |
Breast cancer |
2014 |
|
China |
Non-pegylated liposome |
400 nm |
Premedication protocols are required to reduce vehicle-related toxicity |
Liposomal paclitaxel |
Luye Pharma Group; Sike Pharmaceutical Co. Ltd., Nanjing, Jiangsu, P.R. China |
Ovarian, breast, gastric, and non-small cell lung cancers |
2003 |
|
|
Russia, the European Union, orphan drug designation from the USFDA |
Surfactant XR-17 |
20–60 nm |
Freeze-dried powder dissolved in a conventional solution |
Oasmia Pharmaceutical AB |
Epithelial ovarian cancer in combination with carboplatin |
2015 |
||
|
Nanoxel[60] |
India |
Polymer micelle (polyvinyl-pyrrolidone, cholesteryl sulfate, and caprylic acid); NOT lyophilized for storage at room temperature, needs storage at 2–8°C[14] |
100–110 nm[14] |
Requires 5% w/v dextrose injection infusion bag provided along with the combi pack to be used |
Paclitaxel nanoparticles |
Fresenius Kabi India Pvt. Ltd. |
Breast cancer, ovarian cancer, non-small cell lung cancer, and AIDS related Kaposi's sarcoma |
2008 |
|
Korea, India, Vietnam, the Philippines, and Indonesia. In development for metastatic breast cancer and NSCLC in the US and Singapore |
Polymer micelle (PEG-PDLLA); lyophilized for room temperature storage[14] |
20–50 nm |
Reconstituted in 0.9% saline or 5% dextrose, administered using a regular IV set |
Nanoparticle, polymeric micelle formulation of the chemotherapy drug paclitaxel |
Seoyoon Cheong, Korea—Samyang Biopharmaceuticals |
Treatment of breast cancer and NSCLC—India Metastatic breast cancer, non-small cell lung cancer (NSCLC), ovarian cancer, and pancreatic cancer—South Korea |
2007 |
GENEXOL-PM—The First Polymeric Micellar PTX
Genexol-PM is prepared using the di-block co-polymer (mPEG-PDLLA), where PEG forms the hydrophilic shell and PDLLA forms the hydrophobic core ([Fig. 2]).

PEG is popular in polymer-based drug delivery systems, as it is soluble in water and has a low intrinsic toxicity. The hydrophilicity of PEG improves the solubility of hydrophobic medicines or carriers in water. It improves the stability of drugs and reduces or prevents drug aggregation in vivo and in storage.[49] Among polyesters (such as poly(L,D-lactide), PLA), PLA is favored because it is biodegradable by hydrolysis and enzymatic activity, and has a low immunogenicity. The US Food and Drug Administration (FDA) has authorized various formulations incorporating PLA.[49] The mPEG-PDLLA micelles first interact with cell membranes, followed by the release of loaded PTX, which is internalized into the cells by endocytosis. Thus, PEG-PLA micelles can overcome multiple drug resistance.[21] [50]
In preclinical evaluation of Genexol-PM, the biodistribution of PTX showed two to three times higher levels in tissues, including liver, spleen, kidneys, lungs, heart, and tumor, as compared to Taxol. The in vivo antitumor efficacy of this polymeric micellar PTX was significantly higher than that of Taxol.[42] It has the highest MTD compared to any of the other formulations. It also demonstrated bioequivalence to Abraxane in the first eight patients enrolled in the USFDA-registered TRIBECA clinical trial.[45] It is currently approved for the treatment of non-small cell lung cancer (NSCLC) and ovarian cancer in Korea and for metastatic breast cancer in Korea, India, Vietnam, the Philippines, and Indonesia[14] and is in development for metastatic breast cancer and NSCLC in the United States and Singapore.[14] [50] Over the years since preclinical evaluation, 22 studies on Genexol-PM have been published, making it the most widely studied polymeric micellar PTX.
Clinical Studies on the Safety and Efficacy of Polymeric Micellar PTX
The first phase 1 study was conducted in 2004 to determine the MTD, dose-limiting toxicities, and pharmacokinetic profile of Genexol-PM in 21 patients with advanced, solid malignancies, refractory to conventional treatment or with no effective therapy for their condition. A total of 81 cycles of Genexol-PM were administered with a median of 3.9 cycles per patient. The drug was safely administered in the outpatient setting over 3 hours without prophylactic medication and in-line filtration. It was nontoxic at dosages up to 300 mg/m2. At the MTD of 390 mg/m2, various drug-limiting toxicities (DLTs), including neuropathy, myalgia, and neutropenia, were observed. Grades 3 to 4 neutropenia occurred between doses of 230 and 390 mg/m2, but these were of short lasting and normalized before the next cycle.[51] Subsequently, it was evaluated for in vitro cytotoxicity and in vivo antitumor activity in pancreatic tumors. It was superior to gemcitabine and Taxol at equivalent clinical doses in two human pancreatic tumor xenograft models (MIA PaCa-2 and PANC-1) without drug toxicity. It also showed considerably better tumor inhibitory activity compared to gemcitabine or Taxol.[52] Since these early studies, Genexol-PM has been investigated in patients with various solid tumors such as breast, lung, pancreatic, urothelial, gynecological, thymic, head-face-neck, and biliary cancers. Among these, phase 3 and 4 studies have been conducted in breast cancer.
[Table 2] shows the studies with polymeric micellar PTX in breast cancer. Doses of 260 to 300 mg/m2 every 3 weeks were tolerated well, with neuropathy and neutropenia being the most common adverse effects. The objective response rate ranged from 39 to 67%, with progression-free survival (PFS) of 7 to 9 months.
|
Study type and year |
Patients |
Regimen(s) |
Outcomes |
Adverse effects |
|---|---|---|---|---|
|
Phase 2,[61] 2008 |
41 with histologically confirmed metastatic breast cancer |
Genexol-PM 300 mg/m2 every 3 wk |
Overall response rate was 58.5% (with 5 complete responses and 19 partial responses). Thirty-seven patients who received Genexol-PM as a first-line therapy showed a response rate of 59.5%. Median time to progression: 9 mo |
Grade 3 non-hematologic toxicities, including sensory peripheral neuropathy (51.2%) |
|
Phase 2,[62] 2016 |
30 patients with advanced HER-2-negative breast cancer |
Genexol-PM 260 mg/m2 and doxorubicin 50 mg/m2; 3-wk interval cycle. Six to nine cycles of combination chemotherapy |
Objective response rate 67%; disease control rate 87%, median duration of response 5.5 mo, median PFS was 7.4 mo, OS 38.7 mo |
Most common Grade 3/4 toxicities were neutropenia (43%) and neutropenic fever (27%) |
|
Phase 3,[63] 2017 |
212 patients with recurrent or metastatic HER2-negative breast cancer |
Genexol-PM 260 mg/m2 or Genexol 175 mg/m2 IV every 3 wk |
Mean received dose intensity of Genexol-PM was 246.8 ± 21.3 mg/m2 Median follow-up 24.5 mo Objective response rate of Genexol-PM 39.1%; partial response 39.1%, stable disease 43.8%, progressive disease 6.7%, OS 28.8 mo; PFS 8.0 mo |
The most common toxicity was neutropenia (68.6%) |
|
Phase 4,[64] 2014 |
148 patients with locally recurrent or metastatic breast cancer |
Partial response 24.32%, stable disease 35.81%, progressive disease 39.1%. Efficacy was 42.47% in patients who received six or more cycles. 26.67% without concomitant chemotherapy had partial responses |
11.29% of patients reported a total of 34 serious adverse events; the most frequent were neutropenia (1.61%), febrile neutropenia (1.61%), headache (1.61%), vomiting (1.08%), fever (1.08%), dyspnea (1.08%), and tachycardia (1.08%) |
Abbreviations: HER2, human epidermal growth factor receptor 2; OS, overall survival; PFS, progression-free survival.
[Table 3] shows the studies conducted with polymeric micellar PTX in gynecological cancers. The studies showed that doses up to 260 mg/m2 were well tolerated, but there was a possibility of DLTs at 300 mg/m2 every 3 weeks. The main adverse events continued to be neuropathy and neutropenia, but were not dose-limiting. In the phase 2 study, the overall response rate was 88.0%[53] with a 260 mg/m2 dose every 3 weeks in patients with epithelial ovarian cancer. In patients with stage III to IV high-grade serous ovarian cancer, the median PFS was 35.5 months with a dose of 280 mg/m2 every 3 weeks.[54]
|
Study type and year |
Patients |
Regimen(s) |
Outcomes |
Adverse effects |
|---|---|---|---|---|
|
Phase 1,[65] 2016 |
18 patients with advanced epithelial ovarian cancer and measurable residual disease after debulking surgery |
Different doses of Genexol-PM (220, 260, and 300 mg/m2, once every 3 wk) and 5 area under the curve (AUC) carboplatin |
The best overall response rate was 94.1%; complete response was reported in 6 patients and partial response in 11 patients. One patient had progressive disease. |
DLTs not reported at 220 mg/m2 or 260 mg/m2, but at 300 mg/m2, 1 patient experienced DLT (grade 3 general pain). Neutropenia and neuromuscular toxicity; 22.2% incidence of grade 3/4 neutropenia. Most common non-hematologic toxicity was peripheral neuropathy (17.6%) |
|
Phase 2,[53] 2017 |
98 patients with International Federation of Gynecology and Obstetrics stage IC-IV epithelial ovarian cancer |
Genexol-PM 260 mg/m2 (n = 50) or Genexol 175 mg/m2 (n = 48) with 5 area under the curve carboplatin every 3 weeks (6 cycles) |
Median follow-up 18.0 months. Overall response rate 88.0% with Genexol-PM, and 77.1% with Genexol. Median time to progression was 14.8 months with Genexol-PM and 15.4 months with Genexol. Tumor progression was seen in 20 (40%) patients in the Genexol-PM group, and 18 (37.5%) patients in the Genexol group |
Neutropenia was the most common toxicity (86.0% vs. 77.1%, p = 0.120; Genexol-PM vs Genexol). Peripheral neuropathy incidences were 84.0% versus 64.6% (p= 0.148; Genexol-PM vs Genexol) |
|
Phase 1,[66] 2023 |
18 patients with gynecologic cancer (ovary and fallopian tube in 15 cases and endometrium in 3 cases); 11 patients were newly diagnosed and 7 were recurrent cases |
Cohort 1 received 100 mg/m2 weekly Genexol-PM and 5 area under the curve (AUC) carboplatin, Cohort 2 received 120 mg/m2 weekly Genexol-PM and 5 AUC carboplatin, and Cohort 3 120 mg/m2 weekly Genexol-PM and 6 AUC carboplatin |
Median duration of follow-up was 60.5 months. The overall response rate of weekly Genexol-PM in combination with carboplatin was 72.2%. Median PFS and OS were not reached |
1 patient discontinued the treatment due to DLT. 97.3% of adverse events were resolved without sequelae. Neutropenia was the most common hematological adverse event, and grade 3/4 neutropenia was observed in all patients |
|
Prospective cohort study with historical controls,[54] 2024 |
128 patients with stage III–IV high-grade serous ovarian cancer who underwent upfront surgery |
Cohort 1 (n = 49) Genexol-PM (280 mg/m2) and carboplatin at an area under the curve (AUC) of 5 every 3 wk. Historical controls: cohort 2 (n = 53) PTX (175 mg/m2) and carboplatin (AUC 5), cohort 3 (n = 26) PTX (175 mg/m2), carboplatin (AUC 5) and bevacizumab (15 mg/kg |
Cohort 1 showed better PFS than cohort 2 (median, 35.5 vs. 28.1 mo; p < 0.01), no difference between cohorts 1 and 3 (median, 35.5 vs. 24.9 mo; p = 0.17). OS was not different between the three cohorts. Stage III disease was a favorable factor for PFS |
Abbreviations: DLT, drug-limiting toxicity; OS, overall survival; PFS, progression-free survival; PTX, paclitaxel.
[Table 4] shows studies of polymeric micellar PTX in pancreatic cancer and lung cancer. A higher dose (300 or 350 mg/m2) was administered in treatment-naive patients with pancreatic cancer. In patients with advanced NSCLC, doses ranging from 230 to 300 mg/m2 were tolerated without serious adverse effects. Neutropenia and neuropathy continued to be the leading adverse effects.
|
Study type and year |
Patients |
Regimen(s) |
Outcomes |
Adverse effects |
|---|---|---|---|---|
|
Multicenter, open-label Phase II; 2010[67] |
56 patients with locally advanced or metastatic pancreatic cancer, ECOG performance status ≤ 2, no prior chemotherapy, and adequate organ function |
Initial patients were treated with 435 mg/m2 (n = 11). The dose was reduced for subsequent patients to 350 or 300 mg/m2 (n = 45) |
Median time to tumor progression for patients treated with 300 or 350 mg/m2 doses was 3.2 mo. Median PFS was 2.8 mo. Median OS was 6.5 mo. There was 1 complete remission and 2 partial remissions with an overall response rate of 6.7%. Disease control rate (CR + PR + stable disease) was 60.0% |
Most common grade 3 toxicities were: neutropenia (40.0%), fatigue (17.8%), infection, dehydration, neuropathy (each 13.3%), and abdominal pain (11.1%) |
|
Multicenter, phase 2 study; 2023[68] |
32 patients, median age 65 years, recurrent and metastatic adenocarcinoma of the pancreas |
GENEXOL-PM (125 mg/m2) and gemcitabine (1,000 mg/m2) IV on days 1, 8, and 15 every 4 wk |
Overall response rate was 19.2%; clinical benefit rate (partial response + stable disease) was 34.6%; median PFS and OS were 8 and 22 mo, respectively. Median number of cycles administered was 5.0 (range = 1–21) |
Most common grade 3 or higher hematological toxicities were: neutropenia in 29.0% of patients, neutrophil count decrease (16.1%), and anemia (16.1%). The most common grade 3/4 non-hematological toxicities were generalized muscle weakness (11.5%), pneumonitis (11.5%), and liver abscess (4.3%) |
|
Multicenter phase II trial; 2007[69] |
69 Patients with advanced NSCLC |
Genexol-PM 230 mg/m2 and cisplatin 60 mg/m2 on day 1 of a 3-wk cycle as first-line therapy. Dose escalation of Genexol-PM to 300 mg/m2 was conducted from the second cycle if the prespecified toxic effects were not observed after the first cycle |
The overall response rate was 37.7%; all responses were partial responses. 29.0% achieved a stable disease status. The median time to progression was 5.8 mo and the median survival period was 21.7 mo Dose intensity (the actual dose delivered as a proportion of the planned dose) was 97% at the first cycle (planned dose, 76.7 mg/m2/wk) and 84% at subsequent cycles (planned dose, 100 mg/m2/wk) for Genexol-PM. Dose escalation of Genexol-PM to 300 mg/m2 at the second cycle was carried out in 46% of patients |
Major non-hematologic toxic effects included grade 3 peripheral sensory neuropathy (13.0%) and grade 3/4 arthralgia (7.3%). Four patients (5.8%) experienced grade 3/4 hypersensitivity reactions. The major hematological toxic effects were grade 3/4 neutropenia (29.0 and 17.4%, respectively) |
|
Prospective, single-arm, single-center phase II study; 2013[70] |
43 Patients with advanced NSCLC; ECOG PS 0–2 |
Genexol-PM 230 mg/m2 on day 1 and gemcitabine 1,000 mg/m2 on day 1 and day 8 of a 3-wk cycle. Six cycles of chemotherapy were planned unless there was disease progression |
Patients received the study drugs with a median of 4 cycles per patient (range 1–6). The overall response rate was 46.5%. the median PFS was 4.0 mo, and the median OS was 14.8 mo |
The most common toxicities were anemia (n = 29, 67%), asthenia (n = 17, 40%), myalgia (n = 16, 37%), peripheral neuropathy (n = 15, 35%), and diarrhea. (n = 12, 30%). The most common grade 3/4 adverse events were neutropenia (n = 7, 16%) and pneumonia (n = 5, 12%); two patients died of pneumonia and dyspnea |
Abbreviations: CR, complete response; ECOG, Eastern Cooperative Oncology Group; NSCLC, non-small cell lung cancer; OS, overall survival; PFS, progression-free survival; PR, partial response; PS, performance score.
Studies with polymeric micellar PTX in other solid tumors are shown in [Table 5]. Phase 2 studies in various other solid tumors, such as head/face/neck cancers, urothelial carcinoma, thymic cancer, biliary tract cancer, and upper gastrointestinal cancers, have been conducted. Except for grade 2 hypersensitivity reactions in eight patients undergoing palliative treatment for thymic cancer, most other patients had neutropenia and neuropathy of grade 3 or 4 as the main adverse events. The doses ranged from 200 to 300 mg/m2, depending on the cancer type and cycle frequency.
|
Study type and year |
Patients |
Regimen(s) |
Outcomes |
Adverse effects |
|
|---|---|---|---|---|---|
|
Phase I pharmacokinetic study[71] |
24 patients were refractory to previous chemotherapy. The majority of patients had lung, nasopharyngeal, and breast cancers |
Genexol-PM on a weekly basis for 3 wk, followed by a resting week. The starting dose was 80 mg/m2, and the maximum administered dose was 200 mg/m2 |
Five (21%) patients had a partial response, nine (38%) had stable disease, and seven (29%) had disease progression. The median number of cycles of Genexol-PM administered was 4. The MTD was defined at 180 mg/m2 |
The most common grade 3 non-hematologic adverse events in cycle 1 were fatigue (4%) and neuropathy (4%), occurring mainly at 200 mg/m2 |
|
|
Multicenter phase II study[72] |
34 patients with advanced urothelial carcinoma who developed disease progression after gemcitabine and cisplatin combination chemotherapy |
Genexol-PM 240 mg/m2 IV every 3 wk. Dose escalation to 300 mg/m2 was allowed during the second and subsequent cycles if prespecified toxicities were not observed during the first cycle |
7 responses (21%), including one complete response (CR), with a median response duration of 6.5 mo, were seen. The median time to progression was 2.7 mo with a median overall survival of 6.5 mo |
The most common grade 3/4 non-hematologic toxicities were peripheral neuropathy (sensory type 5.9%; motor type 8.8%) and infection (5.9%). Grade ≥3 hematologic toxicities occurred in only one patient |
|
|
Prospective phase II study[73] |
42 patients with unresectable thymic epithelial tumors; median age was 59 y |
Cisplatin (70 mg/m2) and Genexol-PM (230 mg/m2) on day 1 of a 3-wk cycle as first-line palliative chemotherapy |
The median number of treatment cycles was six. Objective response rate was 62.5% with rates of 46% for advanced thymoma and 70% for thymic carcinoma. With a median follow-up of 15.5 mo, the median PFS for all 42 patients was 9.8 mo. 2-y OS was 77.9% for thymoma and 65.9% for thymic carcinoma |
The most common grade 3 and 4 treatment-related adverse event was neutropenia in 11 patients (26%). Eight patients (19%) experienced grade 2 hypersensitivity reactions |
|
|
Retrospective observational study[74] |
48 patients with solid tumor malignancies—cancer of the breast (21), gynecological cancer (12), lung (2), upper GI (6). 77.08% had advanced cancers. 66.67% had received previous chemotherapy |
Genexol-PM 125 mg/m2 as a single agent weekly therapy or in combination with platinum doublet, 230 mg/m2 on day 1 of a 3-wk cycle. 72.92% received weekly therapy of Genexol-PM |
Response rate in advanced cancers at the end of schedule therapy was 60.4% |
The major non-hematologic toxic effects included grade 3 peripheral sensory neuropathy (14.6%). Adjustment in doses was required in 41.6% patients. One patient (2.08%) experienced grade 3/4 hypersensitivity reactions. The major hematological toxic effects were grade 3/4 neutropenia, 27.08% required hospital admission |
|
|
Multicenter phase II clinical trial[75] |
39 patients with unresectable or metastatic biliary tract cancer |
100 mg/m2 Genexol-PM and 1,000 mg/m2 gemcitabine intravenously on days 1 and 8 every 21 days |
10 partial responses (25.6%) and 18 with stable diseases (46.2%) were confirmed with a median response duration of 4.1 mo. The median PFS was 5.9 ± 1.6 mo and OS 11.9 ± 1.4 mo. The median number of cycles administered was 4.0 (range = 1–10) |
Grade 3 or more neutropenia occurred in 12 patients (26.7%). The most common grade 3/4 non-hematological toxicities were febrile neutropenia (13.4%) and elevation of liver enzymes (6.7%) |
|
|
Open-label, single-arm, phase II study[76] |
52 patients with locally advanced head and neck squamous cell carcinoma |
Genexol-PM (230 mg/m2) and cisplatin (60 mg/m2) every 3 wk as induction therapy. After three cycles, definitive treatment of either concurrent chemoradiotherapy (CCRT) with weekly cisplatin (30 mg/m2) or surgery |
47 completed three cycles of IC, and the ORR was 55.8%. Fifty-one patients received definitive treatment (CCRT [n = 44] or radical surgery [n =7]). The rate of complete response following CCRT was 81.8% (36/44). After a median follow-up of 39 mo, estimates of PFS and OS at 3 y were 54.3 and 71.3%, respectively |
Most common grade 3 or 4 toxicities were neutropenia (15.4%), anorexia (7.7%), and general weakness (7.7%) |
Abbreviations: ECOG, Eastern Cooperative Oncology Group; OS, overall survival; PFS, progression-free survival; PS, performance score.
Thus, several studies have established the efficacy, safety, and tolerance of higher doses of polymeric micellar PTX compared to Taxol.
However, there are no other approved and marketed polymeric micellar PTX formulations. Furthermore, despite the availability of several nanocarriers, the only other PTX nanoformulations are albumin-bound or lipid emulsions. Studies on the available formulations are scarce. Moreover, there are no head-to-head studies comparing the various formulations. Hence, Abraxane continues to be widely used despite its limitations. There is a dire need for newer and safer nanoformulations of PTX.
Conclusion
There have been several advances in nanoformulations of PTX to overcome the risk of anaphylactic hypersensitivity reactions and other severe adverse events due to the solvent CrEL. The first nanoformulation, which was human albumin-bound PTX, can react with proteins in the blood and is not sufficiently stable due to its structural properties. Small-sized nanoformulations (<100 nm) increase the plasma half-life of the drugs and ensure better tumor penetration with fewer adverse effects. Lipids and polymers (polymeric micelles) have been the most commonly used materials for preparing nano PTX. Among these, the smaller size of polymeric micellar PTX facilitates extravasation from blood vessels into the tumor tissue, besides evading the phagocytic system. They can escape recognition by the RES in healthy tissues, thus reducing the adverse effects of the drug, with better tolerance of higher doses. However, currently, there is only one approved and marketed formulation of polymeric micellar PTX, and studies on the available liposomal PTX formulations are scarce. There is a need for more PTX nanoformulations with different carriers, and more phase 3 and phase 4 studies on the available PTX nanoformulations for more conclusive evidence of their advantages and to increase their use in clinical practice. Moreover, head-to-head studies comparing the outcomes of various PTX nanoformulations are necessary to help clinicians make an informed decision when choosing nano PTX for their patients.
Conflict of Interest
G.P., M.K., and K.P. are employees of Lupin Ltd.
Acknowledgments
Dr. Sangeeta Dhanuka from MedicoMindsPro provided writing support for the manuscript.
Declaration of GenAI Use
AI was used to create images of polymeric micellar PTX.
Authors' Contributions
All authors contributed equally to conceptualization, defining the content, conducting a literature search, preparing the manuscript, editing, and reviewing. The manuscript has been read and approved by all the authors, the requirements for authorship have been met, and each author believes that the manuscript represents honest work.
Patient's Consent
Patient consent is not applicable as this is a narrative review article. The data from previously published studies has been reviewed.
-
References
- 1 Raju GSR, Pavitra E, Varaprasad GL. et al. Nanoparticles mediated tumor microenvironment modulation: current advances and applications. J Nanobiotechnology 2022; 20 (01) 274
- 2 Meng W, Huang L, Guo J, Xin Q, Liu J, Hu Y. Innovative nanomedicine delivery: targeting tumor microenvironment to defeat drug resistance. Pharmaceutics 2024; 16 (12) 1549
- 3 Yang M, Li J, Gu P, Fan X. The application of nanoparticles in cancer immunotherapy: targeting tumor microenvironment. Bioact Mater 2020; 6 (07) 1973-1987
- 4 Neophytou CM, Panagi M, Stylianopoulos T, Papageorgis P. The role of tumor microenvironment in cancer metastasis: molecular mechanisms and therapeutic opportunities. Cancers (Basel) 2021; 13 (09) 2053
- 5 Ravi Kiran AVVV, Kusuma Kumari G, Krishnamurthy PT, Khaydarov RR. Tumor microenvironment and nanotherapeutics: intruding the tumor fort. Biomater Sci 2021; 9 (23) 7667-7704
- 6 Fernandes C, Suares D, Yergeri MC. Tumor microenvironment targeted nanotherapy. Front Pharmacol 2018; 9: 1230
- 7 Deng J, Yuan S, Pan W, Li Q, Chen Z. Nanotherapy to reshape the tumor microenvironment: a new strategy for prostate cancer treatment. ACS Omega 2024; 9 (25) 26878-26899
- 8 Tang L, Mei Y, Shen Y. et al. Nanoparticle-mediated targeted drug delivery to remodel tumor microenvironment for cancer therapy. Int J Nanomedicine 2021; 16: 5811-5829
- 9 Tian H, Zhang T, Qin S. et al. Enhancing the therapeutic efficacy of nanoparticles for cancer treatment using versatile targeted strategies. J Hematol Oncol 2022; 15 (01) 132
- 10 Gavas S, Quazi S, Karpiński TM. Nanoparticles for cancer therapy: current progress and challenges. Nanoscale Res Lett 2021; 16 (01) 173
- 11 Tu Y, Yao Z, Yang W. et al. Application of nanoparticles in tumour targeted drug delivery and vaccine. Front Nanotechnol 2022; 4
- 12 Nirmala MJ, Kizhuveetil U, Johnson A, G. B, Nagarajan R, Muthuvijayan V. Cancer nanomedicine: a review of nano-therapeutics and challenges ahead. RSC Adv 2023; 13 (13) 8606-8629
- 13 Jin GW, Rejinold NS, Choy JH. Multifunctional polymeric micelles for cancer therapy. Polymers (Basel) 2022; 14 (22) 4839
- 14 Bernabeu E, Cagel M, Lagomarsino E, Moretton M, Chiappetta DA. Paclitaxel: What has been done and the challenges remain ahead. Int J Pharm 2017; 526 (1-2): 474-495
- 15 Xia Y, Fu S, Ma Q, Liu Y, Zhang N. Application of nano-delivery systems in lymph nodes for tumor immunotherapy. Nano-Micro Lett 2023; 15 (01) 145
- 16 Lee J, Kang S, Park H, Sun JG, Kim EC, Shim G. Nanoparticles for lymph node-directed delivery. Pharmaceutics 2023; 15 (02) 565
- 17 Park W, Heo YJ, Han DK. New opportunities for nanoparticles in cancer immunotherapy. Biomater Res 2018; 22 (01) 24
- 18 Cassani M, Fernandes S, Pagliari S, Cavalieri F, Caruso F, Forte G. Unraveling the role of the tumor extracellular matrix to inform nanoparticle design for nanomedicine. Adv Sci (Weinh) 2025; 12 (02) e2409898
- 19 Trac N, Chung EJ. Overcoming physiological barriers by nanoparticles for intravenous drug delivery to the lymph nodes. Exp Biol Med (Maywood) 2021; 246 (22) 2358-2371
- 20 Goodman TT, Olive PL, Pun SH. Increased nanoparticle penetration in collagenase-treated multicellular spheroids. Int J Nanomedicine 2007; 2 (02) 265-274
- 21 Ma P, Mumper RJ. Paclitaxel nano-delivery systems: a comprehensive review. J Nanomed Nanotechnol 2013; 4 (02) 1000164
- 22 Sharifi-Rad J, Quispe C, Patra JK. et al. Paclitaxel: application in modern oncology and nanomedicine-based cancer therapy. Oxid Med Cell Longev 2021; 2021 (01) 3687700
- 23 Abu Samaan TM, Samec M, Liskova A, Kubatka P, Büsselberg D. Paclitaxel's mechanistic and clinical effects on breast cancer. Biomolecules 2019; 9 (12) 789
- 24 Sati P, Sharma E, Dhyani P. et al. Paclitaxel and its semi-synthetic derivatives: comprehensive insights into chemical structure, mechanisms of action, and anticancer properties. Eur J Med Res 2024; 29 (01) 90
- 25 Deng C, Xu C, Zhang X. et al. A novel paclitaxel-loaded polymeric micelle system with favorable biocompatibility and superior antitumor activity. Anticancer Res 2018; 38 (01) 219-225
- 26 Gelderblom H, Verweij J, Nooter K, Sparreboom A, Cremophor EL. Cremophor EL: the drawbacks and advantages of vehicle selection for drug formulation. Eur J Cancer 2001; 37 (13) 1590-1598
- 27 Scripture CD, Figg WD, Sparreboom A. Paclitaxel chemotherapy: from empiricism to a mechanism-based formulation strategy. Ther Clin Risk Manag 2005; 1 (02) 107-114
- 28 Ahmed S, Rehman SU, Tabish M. Cancer nanomedicine: a step towards improving the drug delivery and enhanced efficacy of chemotherapeutic drugs. OpenNano 2022; 7: 100051
- 29 Gressler S, Hipfinger C, Part F, Pavlicek A, Zafiu C, Giese B. A systematic review of nanocarriers used in medicine and beyond - definition and categorization framework. J Nanobiotechnology 2025; 23 (01) 90
- 30 Kashapov R, Ibragimova A, Pavlov R. et al. Nanocarriers for biomedicine: from lipid formulations to inorganic and hybrid nanoparticles. Int J Mol Sci 2021; 22 (13) 7055
- 31 Patra JK, Das G, Fraceto LF. et al. Nano based drug delivery systems: recent developments and future prospects. J Nanobiotechnology 2018; 16 (01) 71
- 32 Thapa RK, Kim JO. Nanomedicine-based commercial formulations: current developments and future prospects. J Pharm Investig 2023; 53 (01) 19-33
- 33 Jin X, Qian H, Xie Y. et al. Biocompatible and biodegradable nanocarriers for targeted drug delivery in precision medicine. Biomimetics (Basel) 2025; 10 (07) 430
- 34 Davis ME, Chen ZG, Shin DM. Nanoparticle therapeutics: an emerging treatment modality for cancer. Nat Rev Drug Discov 2008; 7 (09) 771-782
- 35 Gatto MS, Najahi-Missaoui W. Lyophilization of nanoparticles, does it really work? Overview of the current status and challenges. Int J Mol Sci 2023; 24 (18) 14041
- 36 Fonte P, Reis S, Sarmento B. Facts and evidences on the lyophilization of polymeric nanoparticles for drug delivery. J Control Release 2016; 225: 75-86
- 37 Ghanbarzadeh S, Valizadeh H, Zakeri-Milani P. The effects of lyophilization on the physico-chemical stability of sirolimus liposomes. Adv Pharm Bull 2013; 3 (01) 25-29
- 38 Khan M, Kethar J, Gabber G, Advisor U. Should Pharmaceutical Scientists Use Liposomes or Micelles as A Means of Drug Delivery?. Accessed December 30, 2025 at: www.JSR.org
- 39 Sercombe L, Veerati T, Moheimani F, Wu SY, Sood AK, Hua S. Advances and challenges of liposome assisted drug delivery. Front Pharmacol 2015; 6: 286
- 40 Tiwary P, Oswal K, Varghese R, Peri RV, Gupta P. Solid lipid nanoparticles in cervical cancer: a comprehensive review of a decade of progress and prospects. RSC Pharm 2025; 2 (05) 930-949
- 41 Geszke-Moritz M, Moritz M. Solid lipid nanoparticles as attractive drug vehicles: composition, properties and therapeutic strategies. Mater Sci Eng C 2016; 68: 982-994
- 42 Kim SC, Kim DW, Shim YH. et al. In vivo evaluation of polymeric micellar paclitaxel formulation: toxicity and efficacy. J Control Release 2001; 72 (1-3): 191-202
- 43 Oerlemans C, Bult W, Bos M, Storm G, Nijsen JFW, Hennink WE. Polymeric micelles in anticancer therapy: targeting, imaging and triggered release. Pharm Res 2010; 27 (12) 2569-2589
- 44 Blair HA, Deeks ED. Albumin-bound paclitaxel: a review in non-small cell lung cancer. Drugs 2015; 75 (17) 2017-2024
- 45 Sofias AM, Dunne M, Storm G, Allen C. The battle of “nano” paclitaxel. Adv Drug Deliv Rev 2017; 122: 20-30
- 46 Gradishar WJ, Tjulandin S, Davidson N. et al. Phase III trial of nanoparticle albumin-bound paclitaxel compared with polyethylated castor oil-based paclitaxel in women with breast cancer. J Clin Oncol 2005; 23 (31) 7794-7803
- 47 Meng R, Zhu H, Wang Z, Hao S, Wang B. Preparation of drug-loaded albumin nanoparticles and its application in cancer therapy. J Nanomater 2022; 2022 (01)
- 48 Ron N, Cordia J, Yang A. et al. Comparison of Physicochemical Characteristics and Stability of Three Novel Formulations of Paclitaxel: Abraxane, Nanoxel, and Genexol PM; 2025. Accessed December 30, 2025 at: https://aacrjournals.org/cancerres/article/68/9_Supplement/5622/546594/Comparison-of-physicochemical-characteristics-and
- 49 Wang Q, Atluri K, Tiwari AK, Babu RJ. Exploring the application of micellar drug delivery systems in cancer nanomedicine. Pharmaceuticals (Basel) 2023; 16 (03) 433
- 50 Rodríguez F, Caruana P, De la Fuente N. et al. Nano-based approved pharmaceuticals for cancer treatment: present and future challenges. Biomolecules 2022; 12 (06) 784
- 51 Kim TY, Kim DW, Chung JY. et al. Phase I and pharmacokinetic study of Genexol-PM, a Cremophor-free, polymeric micelle-formulated paclitaxel, in patients with advanced malignancies. Clin Cancer Res 2004; 10 (11) 3708-3716
- 52 Kim S-O, Lee YH, Jeong S-W. et al. Superior Antitumor Efficacy of Genexol®-PM, a Biodegradable Polymeric Micelle Formulation of Paclitaxel (Genexol®) Compared with Gemzar® (Gemcitabine) and Taxol® in Human Pancreatic Cancer Cells in Vitro and in Vivo.; 2025. Accessed December 30, 2025 at: https://aacrjournals.org/cancerres/article/65/9_Supplement/337/519807/Superior-antitumor-efficacy-of-GenexolR-PM-a
- 53 Lee SW, Kim YM, Cho CH. et al. An open-label, randomized, parallel, Phase II trial to evaluate the efficacy and safety of a Cremophor-free polymeric micelle formulation of paclitaxel as first-line treatment for ovarian cancer: a Korean Gynecologic Oncology Group Study (KGOG-3021). Cancer Res Treat 2018; 50 (01) 195-203
- 54 Park SJ, Son JH, Kong TW, Chang SJ, Kim HS. Effect of high-dose polymeric nanoparticle micellar paclitaxel on improved progression-free survival in patients with optimally resected stage III or IV high-grade carcinoma of the ovary: a prospective cohort study with historical controls. Front Oncol 2024; 14: 1203129
- 55 Kim SB, Seo JH, Ahn JH. et al. Phase II study of DHP107 (oral paclitaxel) in the first-line treatment of HER2-negative recurrent or metastatic breast cancer (OPTIMAL study). Ther Adv Med Oncol 2021; 13: 17 588359211061989
- 56 Jang Y, Ko MK, Park YE. et al. Effect of paclitaxel content in the DHP107 oral formulation on oral bioavailability and antitumor activity. J Drug Deliv Sci Technol 2018; 48: 183-192
- 57 Jang Y, Chung HJ, Hong JW, Yun CW, Chung H. Absorption mechanism of DHP107, an oral paclitaxel formulation that forms a hydrated lipidic sponge phase. Acta Pharmacol Sin 2017; 38 (01) 133-145
- 58 Pazenir. Summary of Product Characteristics. Accessed June 19, 2025 at https://www.ema.europa.eu/en/documents/product-information/pazenir-epar-product-information_en.pdf
- 59 Borgå O, Lilienberg E, Bjermo H, Hansson F, Heldring N, Dediu R. Pharmacokinetics of total and unbound paclitaxel after administration of paclitaxel micellar or nab-paclitaxel: an open, randomized, cross-over, explorative study in breast cancer patients. Adv Ther 2019; 36 (10) 2825-2837
- 60 Ranade AA, Joshi DA, Phadke GK. et al. Clinical and economic implications of the use of nanoparticle paclitaxel (Nanoxel) in India. Ann Oncol 2013; 24 (Suppl. 05) v6-v12
- 61 Lee KS, Chung HC, Im SA. et al. Multicenter phase II trial of Genexol-PM, a Cremophor-free, polymeric micelle formulation of paclitaxel, in patients with metastatic breast cancer. Breast Cancer Res Treat 2008; 108 (02) 241-250
- 62 Cho EK, Yun HY, Kim YY, Jeon YS, Park H. Abstract P2–15–11: a phase II trial of Genexol-PM and doxorubicin in patients with advanced Her-2 negative breast cancer. Cancer Res 2020; 80 (4 Suppl): P2 –15–11 P2-15–11
- 63 Park IH, Sohn JH, Kim SB. et al. An open-label, randomized, parallel, Phase III Trial evaluating the efficacy and safety of polymeric micelle-formulated paclitaxel compared to conventional Cremophor EL-based paclitaxel for recurrent or metastatic HER2-negative breast cancer. Cancer Res Treat 2017; 49 (03) 569-577
- 64 Hwang L, Douglas C, Nam D, Trieu V. P0216IG-001 phase 4 data in Korea: safety and efficacy. Eur J Cancer 2014; 50: e70
- 65 Lee SW, Kim YM, Kim YT, Kang SB. An open-label, multicenter, phase I trial of a Cremophor-free, polymeric micelle formulation of paclitaxel combined with carboplatin as a first-line treatment for advanced ovarian cancer: a Korean Gynecologic Oncology Group study (KGOG-3016). J Gynecol Oncol 2017; 28 (03) e26
- 66 Nam SH, Lee SW, Lee YJ, Kim YM. Safety and tolerability of weekly Genexol-PM, a Cremophor-free polymeric micelle formulation of paclitaxel, with carboplatin in gynecologic cancer: a Phase I study. Cancer Res Treat 2023; 55 (04) 1346-1354
- 67 Saif MW, Podoltsev NA, Rubin MS. et al. Phase II clinical trial of paclitaxel loaded polymeric micelle in patients with advanced pancreatic cancer. Cancer Invest 2010; 28 (02) 186-194
- 68 Lee HW, Kang Y, Kim H. et al. Phase 2 study of weekly polymeric micelle-formulated paclitaxel plus gemcitabine in patients with recurrent and metastatic adenocarcinoma of the pancreas. J Clin Oncol 2023;
- 69 Kim DW, Kim SY, Kim HK. et al. Multicenter phase II trial of Genexol-PM, a novel Cremophor-free, polymeric micelle formulation of paclitaxel, with cisplatin in patients with advanced non-small-cell lung cancer. Ann Oncol 2007; 18 (12) 2009-2014
- 70 Ahn HK, Jung M, Sym SJ. et al. A phase II trial of Cremophor EL-free paclitaxel (Genexol-PM) and gemcitabine in patients with advanced non-small cell lung cancer. Cancer Chemother Pharmacol 2014; 74 (02) 277-282
- 71 Lim WT, Tan EH, Toh CK. et al. Phase I pharmacokinetic study of a weekly liposomal paclitaxel formulation (Genexol-PM) in patients with solid tumors. Ann Oncol 2010; 21 (02) 382-388
- 72 Lee JL, Ahn JH, Park SH. et al. Phase II study of a Cremophor-free, polymeric micelle formulation of paclitaxel for patients with advanced urothelial cancer previously treated with gemcitabine and platinum. Invest New Drugs 2012; 30 (05) 1984-1990
- 73 Kim HS, Lee JY, Lim SH. et al. A prospective Phase II study of cisplatin and Cremophor EL-free paclitaxel (Genexol-PM) in patients with unresectable thymic epithelial tumors. J Thorac Oncol 2015; 10 (12) 1800-1806
- 74 Bhatt AD, Ranade AA. 578P A retrospective observational study of efficacy and safety of Genexol-PM, a novel Cremophor-free, polymeric micelle formulation of paclitaxel, in patients with solid tumours. Ann Oncol 2016; 27: ix188
- 75 Kim JY, Do YR, Song HS. et al. Multicenter Phase II clinical trial of Genexol-PM® with gemcitabine in advanced biliary tract cancer. Anticancer Res 2017; 37 (03) 1467-1473
- 76 Keam B, Lee KW, Lee SH. et al. A Phase II Study of Genexol-PM and cisplatin as induction chemotherapy in locally advanced head and neck squamous cell carcinoma. Oncologist 2019; 24 (06) 751-e231
Address for correspondence
Publication History
Article published online:
29 January 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Raju GSR, Pavitra E, Varaprasad GL. et al. Nanoparticles mediated tumor microenvironment modulation: current advances and applications. J Nanobiotechnology 2022; 20 (01) 274
- 2 Meng W, Huang L, Guo J, Xin Q, Liu J, Hu Y. Innovative nanomedicine delivery: targeting tumor microenvironment to defeat drug resistance. Pharmaceutics 2024; 16 (12) 1549
- 3 Yang M, Li J, Gu P, Fan X. The application of nanoparticles in cancer immunotherapy: targeting tumor microenvironment. Bioact Mater 2020; 6 (07) 1973-1987
- 4 Neophytou CM, Panagi M, Stylianopoulos T, Papageorgis P. The role of tumor microenvironment in cancer metastasis: molecular mechanisms and therapeutic opportunities. Cancers (Basel) 2021; 13 (09) 2053
- 5 Ravi Kiran AVVV, Kusuma Kumari G, Krishnamurthy PT, Khaydarov RR. Tumor microenvironment and nanotherapeutics: intruding the tumor fort. Biomater Sci 2021; 9 (23) 7667-7704
- 6 Fernandes C, Suares D, Yergeri MC. Tumor microenvironment targeted nanotherapy. Front Pharmacol 2018; 9: 1230
- 7 Deng J, Yuan S, Pan W, Li Q, Chen Z. Nanotherapy to reshape the tumor microenvironment: a new strategy for prostate cancer treatment. ACS Omega 2024; 9 (25) 26878-26899
- 8 Tang L, Mei Y, Shen Y. et al. Nanoparticle-mediated targeted drug delivery to remodel tumor microenvironment for cancer therapy. Int J Nanomedicine 2021; 16: 5811-5829
- 9 Tian H, Zhang T, Qin S. et al. Enhancing the therapeutic efficacy of nanoparticles for cancer treatment using versatile targeted strategies. J Hematol Oncol 2022; 15 (01) 132
- 10 Gavas S, Quazi S, Karpiński TM. Nanoparticles for cancer therapy: current progress and challenges. Nanoscale Res Lett 2021; 16 (01) 173
- 11 Tu Y, Yao Z, Yang W. et al. Application of nanoparticles in tumour targeted drug delivery and vaccine. Front Nanotechnol 2022; 4
- 12 Nirmala MJ, Kizhuveetil U, Johnson A, G. B, Nagarajan R, Muthuvijayan V. Cancer nanomedicine: a review of nano-therapeutics and challenges ahead. RSC Adv 2023; 13 (13) 8606-8629
- 13 Jin GW, Rejinold NS, Choy JH. Multifunctional polymeric micelles for cancer therapy. Polymers (Basel) 2022; 14 (22) 4839
- 14 Bernabeu E, Cagel M, Lagomarsino E, Moretton M, Chiappetta DA. Paclitaxel: What has been done and the challenges remain ahead. Int J Pharm 2017; 526 (1-2): 474-495
- 15 Xia Y, Fu S, Ma Q, Liu Y, Zhang N. Application of nano-delivery systems in lymph nodes for tumor immunotherapy. Nano-Micro Lett 2023; 15 (01) 145
- 16 Lee J, Kang S, Park H, Sun JG, Kim EC, Shim G. Nanoparticles for lymph node-directed delivery. Pharmaceutics 2023; 15 (02) 565
- 17 Park W, Heo YJ, Han DK. New opportunities for nanoparticles in cancer immunotherapy. Biomater Res 2018; 22 (01) 24
- 18 Cassani M, Fernandes S, Pagliari S, Cavalieri F, Caruso F, Forte G. Unraveling the role of the tumor extracellular matrix to inform nanoparticle design for nanomedicine. Adv Sci (Weinh) 2025; 12 (02) e2409898
- 19 Trac N, Chung EJ. Overcoming physiological barriers by nanoparticles for intravenous drug delivery to the lymph nodes. Exp Biol Med (Maywood) 2021; 246 (22) 2358-2371
- 20 Goodman TT, Olive PL, Pun SH. Increased nanoparticle penetration in collagenase-treated multicellular spheroids. Int J Nanomedicine 2007; 2 (02) 265-274
- 21 Ma P, Mumper RJ. Paclitaxel nano-delivery systems: a comprehensive review. J Nanomed Nanotechnol 2013; 4 (02) 1000164
- 22 Sharifi-Rad J, Quispe C, Patra JK. et al. Paclitaxel: application in modern oncology and nanomedicine-based cancer therapy. Oxid Med Cell Longev 2021; 2021 (01) 3687700
- 23 Abu Samaan TM, Samec M, Liskova A, Kubatka P, Büsselberg D. Paclitaxel's mechanistic and clinical effects on breast cancer. Biomolecules 2019; 9 (12) 789
- 24 Sati P, Sharma E, Dhyani P. et al. Paclitaxel and its semi-synthetic derivatives: comprehensive insights into chemical structure, mechanisms of action, and anticancer properties. Eur J Med Res 2024; 29 (01) 90
- 25 Deng C, Xu C, Zhang X. et al. A novel paclitaxel-loaded polymeric micelle system with favorable biocompatibility and superior antitumor activity. Anticancer Res 2018; 38 (01) 219-225
- 26 Gelderblom H, Verweij J, Nooter K, Sparreboom A, Cremophor EL. Cremophor EL: the drawbacks and advantages of vehicle selection for drug formulation. Eur J Cancer 2001; 37 (13) 1590-1598
- 27 Scripture CD, Figg WD, Sparreboom A. Paclitaxel chemotherapy: from empiricism to a mechanism-based formulation strategy. Ther Clin Risk Manag 2005; 1 (02) 107-114
- 28 Ahmed S, Rehman SU, Tabish M. Cancer nanomedicine: a step towards improving the drug delivery and enhanced efficacy of chemotherapeutic drugs. OpenNano 2022; 7: 100051
- 29 Gressler S, Hipfinger C, Part F, Pavlicek A, Zafiu C, Giese B. A systematic review of nanocarriers used in medicine and beyond - definition and categorization framework. J Nanobiotechnology 2025; 23 (01) 90
- 30 Kashapov R, Ibragimova A, Pavlov R. et al. Nanocarriers for biomedicine: from lipid formulations to inorganic and hybrid nanoparticles. Int J Mol Sci 2021; 22 (13) 7055
- 31 Patra JK, Das G, Fraceto LF. et al. Nano based drug delivery systems: recent developments and future prospects. J Nanobiotechnology 2018; 16 (01) 71
- 32 Thapa RK, Kim JO. Nanomedicine-based commercial formulations: current developments and future prospects. J Pharm Investig 2023; 53 (01) 19-33
- 33 Jin X, Qian H, Xie Y. et al. Biocompatible and biodegradable nanocarriers for targeted drug delivery in precision medicine. Biomimetics (Basel) 2025; 10 (07) 430
- 34 Davis ME, Chen ZG, Shin DM. Nanoparticle therapeutics: an emerging treatment modality for cancer. Nat Rev Drug Discov 2008; 7 (09) 771-782
- 35 Gatto MS, Najahi-Missaoui W. Lyophilization of nanoparticles, does it really work? Overview of the current status and challenges. Int J Mol Sci 2023; 24 (18) 14041
- 36 Fonte P, Reis S, Sarmento B. Facts and evidences on the lyophilization of polymeric nanoparticles for drug delivery. J Control Release 2016; 225: 75-86
- 37 Ghanbarzadeh S, Valizadeh H, Zakeri-Milani P. The effects of lyophilization on the physico-chemical stability of sirolimus liposomes. Adv Pharm Bull 2013; 3 (01) 25-29
- 38 Khan M, Kethar J, Gabber G, Advisor U. Should Pharmaceutical Scientists Use Liposomes or Micelles as A Means of Drug Delivery?. Accessed December 30, 2025 at: www.JSR.org
- 39 Sercombe L, Veerati T, Moheimani F, Wu SY, Sood AK, Hua S. Advances and challenges of liposome assisted drug delivery. Front Pharmacol 2015; 6: 286
- 40 Tiwary P, Oswal K, Varghese R, Peri RV, Gupta P. Solid lipid nanoparticles in cervical cancer: a comprehensive review of a decade of progress and prospects. RSC Pharm 2025; 2 (05) 930-949
- 41 Geszke-Moritz M, Moritz M. Solid lipid nanoparticles as attractive drug vehicles: composition, properties and therapeutic strategies. Mater Sci Eng C 2016; 68: 982-994
- 42 Kim SC, Kim DW, Shim YH. et al. In vivo evaluation of polymeric micellar paclitaxel formulation: toxicity and efficacy. J Control Release 2001; 72 (1-3): 191-202
- 43 Oerlemans C, Bult W, Bos M, Storm G, Nijsen JFW, Hennink WE. Polymeric micelles in anticancer therapy: targeting, imaging and triggered release. Pharm Res 2010; 27 (12) 2569-2589
- 44 Blair HA, Deeks ED. Albumin-bound paclitaxel: a review in non-small cell lung cancer. Drugs 2015; 75 (17) 2017-2024
- 45 Sofias AM, Dunne M, Storm G, Allen C. The battle of “nano” paclitaxel. Adv Drug Deliv Rev 2017; 122: 20-30
- 46 Gradishar WJ, Tjulandin S, Davidson N. et al. Phase III trial of nanoparticle albumin-bound paclitaxel compared with polyethylated castor oil-based paclitaxel in women with breast cancer. J Clin Oncol 2005; 23 (31) 7794-7803
- 47 Meng R, Zhu H, Wang Z, Hao S, Wang B. Preparation of drug-loaded albumin nanoparticles and its application in cancer therapy. J Nanomater 2022; 2022 (01)
- 48 Ron N, Cordia J, Yang A. et al. Comparison of Physicochemical Characteristics and Stability of Three Novel Formulations of Paclitaxel: Abraxane, Nanoxel, and Genexol PM; 2025. Accessed December 30, 2025 at: https://aacrjournals.org/cancerres/article/68/9_Supplement/5622/546594/Comparison-of-physicochemical-characteristics-and
- 49 Wang Q, Atluri K, Tiwari AK, Babu RJ. Exploring the application of micellar drug delivery systems in cancer nanomedicine. Pharmaceuticals (Basel) 2023; 16 (03) 433
- 50 Rodríguez F, Caruana P, De la Fuente N. et al. Nano-based approved pharmaceuticals for cancer treatment: present and future challenges. Biomolecules 2022; 12 (06) 784
- 51 Kim TY, Kim DW, Chung JY. et al. Phase I and pharmacokinetic study of Genexol-PM, a Cremophor-free, polymeric micelle-formulated paclitaxel, in patients with advanced malignancies. Clin Cancer Res 2004; 10 (11) 3708-3716
- 52 Kim S-O, Lee YH, Jeong S-W. et al. Superior Antitumor Efficacy of Genexol®-PM, a Biodegradable Polymeric Micelle Formulation of Paclitaxel (Genexol®) Compared with Gemzar® (Gemcitabine) and Taxol® in Human Pancreatic Cancer Cells in Vitro and in Vivo.; 2025. Accessed December 30, 2025 at: https://aacrjournals.org/cancerres/article/65/9_Supplement/337/519807/Superior-antitumor-efficacy-of-GenexolR-PM-a
- 53 Lee SW, Kim YM, Cho CH. et al. An open-label, randomized, parallel, Phase II trial to evaluate the efficacy and safety of a Cremophor-free polymeric micelle formulation of paclitaxel as first-line treatment for ovarian cancer: a Korean Gynecologic Oncology Group Study (KGOG-3021). Cancer Res Treat 2018; 50 (01) 195-203
- 54 Park SJ, Son JH, Kong TW, Chang SJ, Kim HS. Effect of high-dose polymeric nanoparticle micellar paclitaxel on improved progression-free survival in patients with optimally resected stage III or IV high-grade carcinoma of the ovary: a prospective cohort study with historical controls. Front Oncol 2024; 14: 1203129
- 55 Kim SB, Seo JH, Ahn JH. et al. Phase II study of DHP107 (oral paclitaxel) in the first-line treatment of HER2-negative recurrent or metastatic breast cancer (OPTIMAL study). Ther Adv Med Oncol 2021; 13: 17 588359211061989
- 56 Jang Y, Ko MK, Park YE. et al. Effect of paclitaxel content in the DHP107 oral formulation on oral bioavailability and antitumor activity. J Drug Deliv Sci Technol 2018; 48: 183-192
- 57 Jang Y, Chung HJ, Hong JW, Yun CW, Chung H. Absorption mechanism of DHP107, an oral paclitaxel formulation that forms a hydrated lipidic sponge phase. Acta Pharmacol Sin 2017; 38 (01) 133-145
- 58 Pazenir. Summary of Product Characteristics. Accessed June 19, 2025 at https://www.ema.europa.eu/en/documents/product-information/pazenir-epar-product-information_en.pdf
- 59 Borgå O, Lilienberg E, Bjermo H, Hansson F, Heldring N, Dediu R. Pharmacokinetics of total and unbound paclitaxel after administration of paclitaxel micellar or nab-paclitaxel: an open, randomized, cross-over, explorative study in breast cancer patients. Adv Ther 2019; 36 (10) 2825-2837
- 60 Ranade AA, Joshi DA, Phadke GK. et al. Clinical and economic implications of the use of nanoparticle paclitaxel (Nanoxel) in India. Ann Oncol 2013; 24 (Suppl. 05) v6-v12
- 61 Lee KS, Chung HC, Im SA. et al. Multicenter phase II trial of Genexol-PM, a Cremophor-free, polymeric micelle formulation of paclitaxel, in patients with metastatic breast cancer. Breast Cancer Res Treat 2008; 108 (02) 241-250
- 62 Cho EK, Yun HY, Kim YY, Jeon YS, Park H. Abstract P2–15–11: a phase II trial of Genexol-PM and doxorubicin in patients with advanced Her-2 negative breast cancer. Cancer Res 2020; 80 (4 Suppl): P2 –15–11 P2-15–11
- 63 Park IH, Sohn JH, Kim SB. et al. An open-label, randomized, parallel, Phase III Trial evaluating the efficacy and safety of polymeric micelle-formulated paclitaxel compared to conventional Cremophor EL-based paclitaxel for recurrent or metastatic HER2-negative breast cancer. Cancer Res Treat 2017; 49 (03) 569-577
- 64 Hwang L, Douglas C, Nam D, Trieu V. P0216IG-001 phase 4 data in Korea: safety and efficacy. Eur J Cancer 2014; 50: e70
- 65 Lee SW, Kim YM, Kim YT, Kang SB. An open-label, multicenter, phase I trial of a Cremophor-free, polymeric micelle formulation of paclitaxel combined with carboplatin as a first-line treatment for advanced ovarian cancer: a Korean Gynecologic Oncology Group study (KGOG-3016). J Gynecol Oncol 2017; 28 (03) e26
- 66 Nam SH, Lee SW, Lee YJ, Kim YM. Safety and tolerability of weekly Genexol-PM, a Cremophor-free polymeric micelle formulation of paclitaxel, with carboplatin in gynecologic cancer: a Phase I study. Cancer Res Treat 2023; 55 (04) 1346-1354
- 67 Saif MW, Podoltsev NA, Rubin MS. et al. Phase II clinical trial of paclitaxel loaded polymeric micelle in patients with advanced pancreatic cancer. Cancer Invest 2010; 28 (02) 186-194
- 68 Lee HW, Kang Y, Kim H. et al. Phase 2 study of weekly polymeric micelle-formulated paclitaxel plus gemcitabine in patients with recurrent and metastatic adenocarcinoma of the pancreas. J Clin Oncol 2023;
- 69 Kim DW, Kim SY, Kim HK. et al. Multicenter phase II trial of Genexol-PM, a novel Cremophor-free, polymeric micelle formulation of paclitaxel, with cisplatin in patients with advanced non-small-cell lung cancer. Ann Oncol 2007; 18 (12) 2009-2014
- 70 Ahn HK, Jung M, Sym SJ. et al. A phase II trial of Cremophor EL-free paclitaxel (Genexol-PM) and gemcitabine in patients with advanced non-small cell lung cancer. Cancer Chemother Pharmacol 2014; 74 (02) 277-282
- 71 Lim WT, Tan EH, Toh CK. et al. Phase I pharmacokinetic study of a weekly liposomal paclitaxel formulation (Genexol-PM) in patients with solid tumors. Ann Oncol 2010; 21 (02) 382-388
- 72 Lee JL, Ahn JH, Park SH. et al. Phase II study of a Cremophor-free, polymeric micelle formulation of paclitaxel for patients with advanced urothelial cancer previously treated with gemcitabine and platinum. Invest New Drugs 2012; 30 (05) 1984-1990
- 73 Kim HS, Lee JY, Lim SH. et al. A prospective Phase II study of cisplatin and Cremophor EL-free paclitaxel (Genexol-PM) in patients with unresectable thymic epithelial tumors. J Thorac Oncol 2015; 10 (12) 1800-1806
- 74 Bhatt AD, Ranade AA. 578P A retrospective observational study of efficacy and safety of Genexol-PM, a novel Cremophor-free, polymeric micelle formulation of paclitaxel, in patients with solid tumours. Ann Oncol 2016; 27: ix188
- 75 Kim JY, Do YR, Song HS. et al. Multicenter Phase II clinical trial of Genexol-PM® with gemcitabine in advanced biliary tract cancer. Anticancer Res 2017; 37 (03) 1467-1473
- 76 Keam B, Lee KW, Lee SH. et al. A Phase II Study of Genexol-PM and cisplatin as induction chemotherapy in locally advanced head and neck squamous cell carcinoma. Oncologist 2019; 24 (06) 751-e231