

Subscribe to RSS
DOI: 10.12945/j.aorta.2015.14.070
Rare Case of Vaginal Delivery in Giant Aortic Aneurysm
Authors
Corresponding Author
Publication History
08 November 2014
16 February 2015
Publication Date:
24 September 2018 (online)

Abstract
A 33-year-old woman underwent successful vaginal delivery despite previously unsuspected 8-cm ascending and 6-cm descending aortic aneurysms. These were repaired immediately after delivery.
It is well known that aortic dissection is a serious problem during pregnancy due to increased risk of maternal death[1]. In some congenital and genetic disorders (Marfan syndrome, bicuspid aortic valve, aortic coarctation), the natural history of the disease is well-known. However, there are a number of congenital heart diseases with aortic dilatation that are not well characterized. We present here a rare case of successful vaginal delivery in a patient with large ascending and descending aortic aneurysms, previously unsuspected.
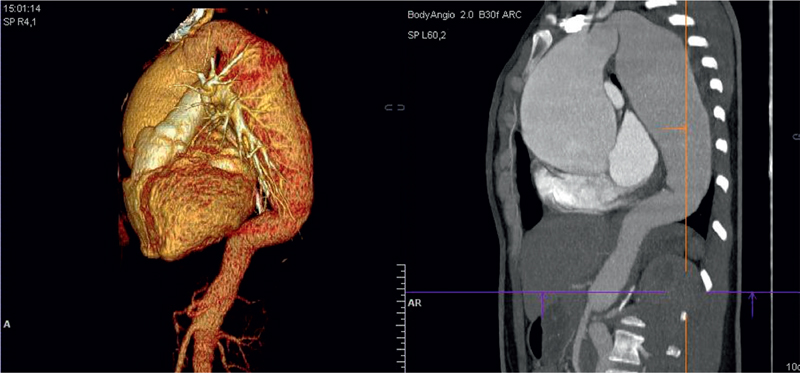
A 33-year-old woman was admitted to the hospital 20 days after her first vaginal delivery from an outside hospital. She complained of chest pain during and after delivery. The patient had no family history of aortic disease or known connective tissue disorders. On examination, there were no signs of genetic disorders such as Marfan syndrome, or Ehlers-Danlos syndrome. On echocardiography an aneurysm of the ascending aorta was found, with severe aortic regurgitation. The aortic valve was tricuspid. On computed tomography (CT) scan, the aneurysms of ascending and descending aorta were identified, with maximum size of the ascending aorta of 81 mm and maximum size of the descending aorta of 61 mm. There were no signs of aortic dissection ([Figure 1]).
The patient underwent a Bentall-De Bono procedure with the Kouchoukos modification with hemiarch reconstruction. Histology of aorta showed cystic medial degeneration with pseudocyst formation in the media, accompanied by extensive loss of elastic lamina. On control CT before the second stage of operation which was performed in 6 months time, enlargement of descending aorta and aortic dissection were found ([Figure 2]). The dissection of the descending aorta developed after Stage 1 of the operation and there were no signs of dissection on initial scans. The size of the aorta enlarged dramatically from 61 mm to 67 mm. Endovascular treatment of the descending aorta with Valliant Thoracic Captiva stent graft was performed. The stent graft did not cover any of the great vessels. On control CT performed 6 months after the procedure there were no signs of deterioration ([Figure 3]).


This is a unique case of vaginal delivery in a woman with giant aortic aneurysm that was not complicated by dissection during delivery. It is well known that aortic aneurysms in young patients are usually associated with connective tissue disorders such as Marfan syndrome, or bicuspid aortic valve. We presume that aortic dissection in this patient was part of the natural history of non-syndromic familial thoracic aortic aneurysm. In the 2014 European Society of Cardiology Guidelines on the diagnosis and treatment of aortic diseases, a new section on non-syndromic familial thoracic aortic aneurysm and dissection was included[2]. Numerous etiologic mutations have been identified. Routine echocardiography is not recommended for all pregnant women without previous cardiac medical history. That is most likely the reason why in this patient the aortic enlargement was undetected due to lack of family history of aortic disease.
Conflict of Interest
The authors have no conflict of interest relevant to this publication.
-
References
- 1 Immer FF, Bansi AG, Immer-Bansi AS, McDougall J, Zehr KJ, Schaff HV. Aortic dissection in pregnancy: Analysis of risk factors and outcome. Ann Thorac Surg 2003; 76: 309-314 . DOI: 10.1016/S0003-4975(03)00169-3
- 2 Erbel R, Aboyans V, Boileau C, Bossone E, Bartolomeo RD, Eggebrecht H. , et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J 2014; 35: 2873-2926 . DOI: 10.1093/eurheartj/ehu281
Corresponding Author
-
References
- 1 Immer FF, Bansi AG, Immer-Bansi AS, McDougall J, Zehr KJ, Schaff HV. Aortic dissection in pregnancy: Analysis of risk factors and outcome. Ann Thorac Surg 2003; 76: 309-314 . DOI: 10.1016/S0003-4975(03)00169-3
- 2 Erbel R, Aboyans V, Boileau C, Bossone E, Bartolomeo RD, Eggebrecht H. , et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J 2014; 35: 2873-2926 . DOI: 10.1093/eurheartj/ehu281