

Subscribe to RSS
DOI: 10.1590/0004-282X20200132
Solitaire stent retriever failure during thrombectomy: is there any image that can predict non-recanalization?
Falha do Solitaire Stent retriever durante a trombectomia: há alguma imagem que pode predizer a não recanalização?Authors

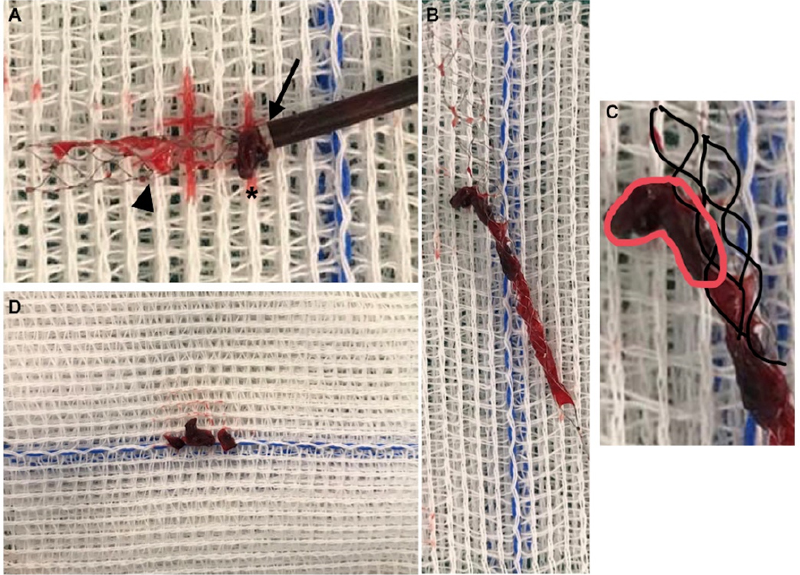
Thrombus configuration[1],[2] may induce variability in artery recanalization.
The “closed tripod sign” (CTS) could be interpreted as poor stent apposition due to the high clot density and low rates of recanalization ([Figure 1]).

If CTS is visualized during the procedure, the stent retriever technique may be substituted for the aspiration-retriever technique for stroke (ARTS)[3] with the blind exchange maneuver described by Nogueira et al.[4] ([Figure 2]). For large vessel occlusion (LVO) strokes of the anterior circulation, we always use the balloon guide catheter (Cello, ev3/Covidien, Irvine, CA, USA).

CTS was visualized after Solitaire deployment, the Rebar catheter was withdrawn, and blind advancement of the ACE68 was performed over the bare retriever delivery wire (blind exchange). ACE68 was advanced until clot contact, and the aspiration was blocked. Stent and ACE68 were pulled as a unit ([Figure 3]). After this maneuver,thrombolysis in cerebral infarction (TICI) 3 was achieved.
Conflict of interest:
There is no conflict of interest to declare.
Authors’ contribution:
All authors contributed equally to this work.
-
References
- 1 Mokin M, Morr S, Natarajan SK, Lin N, Snyder KV, Hopkins LN, et al. Thrombus density predicts successful recanalization with Solitaire stent retriever thrombectomy in acute ischemic stroke. J Neurointerv Surg. 2015 Feb;7(2):104-7. https://doi.org/10.1136/neurintsurg-2013-011017
- 2 Maekawa K, Shibata M, Nakajima H, Mizutani A, Kitano Y, Seguchi M, et al. Erythrocyte-rich thrombus is associated with reduced number of maneuvers and procedure time in patients with acute ischemic stroke undergoing mechanical thrombectomy. Cerebrovasc Dis Extra. 2018 Jan;8(1):39-49. https://doi.org/10.1159/000486042
- 3 Massari F, Henninger N, Lozano JD, Patel A, Kuhn AL, Howk M, et al. ARTS (Aspiration-Retriever Technique for Stroke): Initial clinical experience. Interv Neuroradiol. 2016 Jun;22(3):325-32. https://doi.org/10.1177/1591019916632369
- 4 Haussen DC, Al-Bayati AR, Eby B, Ravindran K, Rodrigues GM, Frankel MR, et al. Blind exchange with mini-pinning technique for distal occlusion thrombectomy. J Neurointerv Surg. 2020 Apr;12(4):392-5. https://doi.org/10.1136/neurintsurg-2019-015205
Publication History
Received: 20 April 2020
Accepted: 19 July 2020
Article published online:
01 June 2023
© 2021. Academia Brasileira de Neurologia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
References
- 1 Mokin M, Morr S, Natarajan SK, Lin N, Snyder KV, Hopkins LN, et al. Thrombus density predicts successful recanalization with Solitaire stent retriever thrombectomy in acute ischemic stroke. J Neurointerv Surg. 2015 Feb;7(2):104-7. https://doi.org/10.1136/neurintsurg-2013-011017
- 2 Maekawa K, Shibata M, Nakajima H, Mizutani A, Kitano Y, Seguchi M, et al. Erythrocyte-rich thrombus is associated with reduced number of maneuvers and procedure time in patients with acute ischemic stroke undergoing mechanical thrombectomy. Cerebrovasc Dis Extra. 2018 Jan;8(1):39-49. https://doi.org/10.1159/000486042
- 3 Massari F, Henninger N, Lozano JD, Patel A, Kuhn AL, Howk M, et al. ARTS (Aspiration-Retriever Technique for Stroke): Initial clinical experience. Interv Neuroradiol. 2016 Jun;22(3):325-32. https://doi.org/10.1177/1591019916632369
- 4 Haussen DC, Al-Bayati AR, Eby B, Ravindran K, Rodrigues GM, Frankel MR, et al. Blind exchange with mini-pinning technique for distal occlusion thrombectomy. J Neurointerv Surg. 2020 Apr;12(4):392-5. https://doi.org/10.1136/neurintsurg-2019-015205