

Subscribe to RSS
DOI: 10.4103/ajns.AJNS_191_18
Extensive pulmonary metastases 13 years after initial resection of intracranial meningioma
Authors

Background: Extracranial metastasis from intracranial meningioma is a very rare condition. A current literature review reveals that only few cases are documented with extensive pulmonary involvement >10 years after initial intracranial meningioma resection. Diagnosis of pulmonary meningioma is often confirmed by computed tomography chest-guided core biopsies. The prognosis of extensive metastatic pulmonary meningioma, however, is unknown and there is no gold standard treatment option. Case Description: We present a case of multiple pulmonary meningioma metastases developing 13 years after initial resection of left occipital parafalcine World Health Organization Grade I intracranial meningioma. Conclusion: There are no established guidelines for the optimal management or surveillance of extensive pulmonary metastatic meningioma. In patients with high-grade meningioma and multiple cannonball pulmonary lesions, metastatic meningioma should be considered as part of the differential diagnosis. Metastatic meningioma may occur even a decade after initial tumour resection.
Key-words:
Meningioma - metastatic meningioma - pulmonary metastases - recurrent meningioma - Rosai–Dorfman diseaseIntroduction
Extracranial metastasis from intracranial meningioma is a very rare condition. The current literature review reveals that only few cases are documented with extensive pulmonary involvement >10 years after initial intracranial meningioma resection. This is a rare case of extensive pulmonary meningioma metastases in a patient 13 years after resection of initial World Health Organization (WHO) Grade I intracranial meningioma.
Case Report
A 52-year-old gentleman was admitted electively for his third redo debulking of right occipital parafalcine meningioma in November 2017. At the time of anesthetic induction, he desaturated and required high ventilator pressure support and high FiO2 requirements to maintain oxygen saturation over 90%. An urgent chest X-ray (CXR) revealed that the endotracheal tube was appropriately positioned, and an incidental large well-delineated left upper lobe nodule was noted. The lung fields were otherwise clear, and there was no associated lung parenchymal abnormality. The following day, a formal CXR was performed [[Figure 1]], the patient was back to his baseline and the surgery was postponed. A CXR performed in 2016 revealed no lung lesions.

A subsequent chest computed tomography (CT) was arranged and confirmed the presence of a 19-mm left upper lobe nodule and a total of five other smaller bilateral pulmonary nodules ranging from 4 to 13 mm, giving a cannonball appearance [[Figure 2]] and [[Figure 3]]. As these nodules were very well circumscribed and appeared benign, the respiratory and multidisciplinary teams felt that the best course of action in this patient would be a repeat chest CT in 6 months.


This patient's medical history included right occipital parafalcine meningioma diagnosed in 1994 which was surgically resected in Auckland, New Zealand. This was followed by the insertion of a left-sided ventriculoperitoneal shunt for postoperative hydrocephalus. Histopathology confirmed WHO Grade I meningioma. On surveillance imaging in Melbourne, Australia, in 2013, he was found to have a recurrence, leading to the first redo craniotomy and debulking. Histopathology in this instance revealed transformation to atypical WHO Grade II meningioma. In February 2016, he developed intractable seizures which lead to his second redo debulking at the same unit. The histopathology remained unchanged.
This patient's third redo debulking procedure was rescheduled to February 2018, approximately 3 months after the diagnosis of the multiple pulmonary lesions. A Simpson Grade 2 resection of recurrent right occipital parafalcine meningioma was performed. Histopathology again showed features consistent with atypical WHO Grade II meningioma [[Figure 4]]; however, although it did not fulfill criteria for anaplastic WHO Grade III meningioma, the higher Ki-67 proliferation index suggested that it may behave more aggressively than the conventional WHO Grade II meningioma. Postoperatively, he developed no new focal neurology and had significant improvement in seizure-free periods. He was treated with postoperative radiation therapy 60 Gy in 30 fractions and had no symptoms to suggest residual acute radiation toxicity.

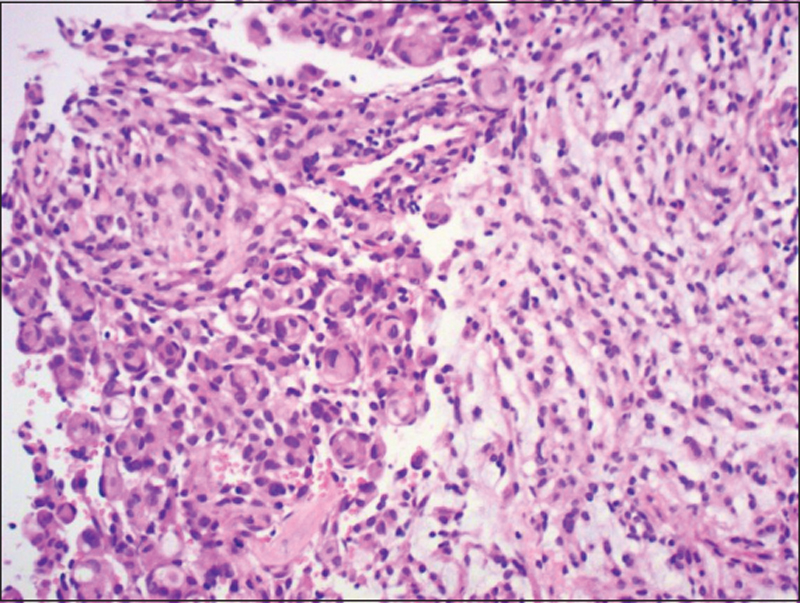
A repeat chest CT was performed in May 2018 and revealed all six lung lesions with interval increase in size, the largest now measuring 27 mm. A chest CT-guided core biopsy of the largest lesion was performed. This confirmed histopathological features consistent with metastatic meningioma [[Figure 5]].
Discussion
Meningioma is one of the most common central nervous system (CNS) tumors and generally originates from arachnoidal cap cells.[[1]],[[2]] Meningiomas are classified into three grades by the WHO. Most are considered benign with good prognosis (WHO Grade I), while more uncommonly, they may be atypical (WHO Grade II) or anaplastic (WHO Grade III) meningiomas which are characterized by a more aggressive biological behavior and greater risk of recurrence and metastases.[[3]],[[4]]
Metastatic meningioma outside the CNS is a very rare entity with <0.1% metastasizing.[[5]] These metastasize to the lung and pleura most commonly, followed by liver, lymph node, and bone.[[6]],[[7]],[[8]],[[9]] They generally occur through hematogenous, lymphogenous, or cerebrospinal fluid spread and mostly occur in atypical or anaplastic (WHO Grade II or III) meningiomas.[[5]] Patients with recurrent meningioma are identified as higher risk of metastases and generally have a relatively higher proliferation-associated antigen Ki-67 index.[[10]] Treatment option for this group of patients includes reoperation, radiotherapy, and stereotactic radiosurgery. Further, in patients with atypical and anaplastic meningioma, treatment is unlikely to be curative with 10-year disease-free survival rates of 13–0%, respectively.[[6]]
The time frame from initial surgical excision to diagnosis of metastases can range from few months to 15 years, and a large proportion of metastases will only be diagnosed after recurrence of the primary tumor.[[5]] Only few case reports in the English literature have discussed patients with extensive pulmonary involvement >10 years after initial intracranial meningioma resection despite recurrences in the interim.[[11]]
Differential diagnosis to consider in patients with multiple meningeal-appearing nodules on imaging is Rosai–Dorfman disease, often referred to as a mimicker of meningioma.[[12]] Patients with this rare disease often have significant lymphadenopathy and diagnosis is only confirmed by histopathology.
To date, there are no established guidelines for optimal treatment of extensive pulmonary metastatic meningioma. In these cases where there is extensive disease, the morbidity of surgery makes it difficult to justify. Radiotherapy and chemotherapy are generally the only options, despite their limited efficacy in overall survival. In cases of solitary meningioma metastases with well-controlled primary disease, surgical resection is recommended in an attempt to improve overall survival.
Conclusion
There are no established guidelines for the optimal management or surveillance of extensive pulmonary metastatic meningioma. In patients with a history of recurrent or high-grade meningioma that has multiple cannonball pulmonary lesions, this case report highlights the importance of considering metastatic pulmonary meningioma as a differential diagnosis. This case also emphasizes that metastatic meningioma may occur even a decade after initial tumor resection.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Frydrychowicz C, Holland H, Hantmann H, Gradistanac T, Hoffmann KT, Mueller W, et al. Two cases of atypical meningioma with pulmonary metastases: A comparative cytogenetic analysis of chromosomes 1p and 22 and a review of the literature. Neuropathology 2015;35:175-83.
- 2 Mei Y, Bi WL, Greenwald NF, Agar NY, Beroukhim R, Dunn GP, et al. Genomic profile of human meningioma cell lines. PLoS One 2017;12:e0178322.
- 3 Forest F, Berremila SA, Gyenes C, Ginguéné C, Kassir R, Sulaiman A, et al. Metastatic meningiomas: An unusual clinical and pathological diagnosis with highly variable outcome. J Neurooncol 2014;120:411-21.
- 4 Mutnuru PC, Ahmed SF, Uppin SG, Lachi PK. Pulmonary metastases from intracranial meningioma. Lung India 2015;32:661-3.
- 5 Nakano M, Tanaka T, Nakamura A, Watanabe M, Kato N, Arai T, et al. Multiple pulmonary metastases following total removal of a bilateral parasagittal meningioma with complete occlusion of the superior sagittal sinus: Report of a case. Case Rep Neurol Med 2012;2012:121470.
- 6 Alexandru D, Glantz MJ, Kim L, Chamberlain MC, Bota DA. Pulmonary metastases in patients with recurrent, treatment-resistant meningioma: Prognosis and identification by 111Indium-octreotide imaging. Cancer 2011;117:4506-11.
- 7 Aumann JL, van den Bosch JM, Elbers JR, Wagenaar SJ. Metastatic meningioma of the lung. Thorax 1986;41:487-8.
- 8 Incarbone M, Ceresoli GL, Di Tommaso L, Cappuzzo F, Inzirillo F, Infante M, et al. Primary pulmonary meningioma: Report of a case and review of the literature. Lung Cancer 2008;62:401-7.
- 9 Kaminski JM, Movsas B, King E, Yang C, Kronz JD, Alli PM, et al. Metastatic meningioma to the lung with multiple pleural metastases. Am J Clin Oncol 2001;24:579-82.
- 10 Pramesh CS, Saklani AP, Pantvaidya GH, Heroor AA, Naresh KN, Sharma S, et al. Benign metastasizing meningioma. Jpn J Clin Oncol 2003;33:86-8.
- 11 Psaras T, Pantazis G, Steger V, Meyermann R, Honegger J, Beschorner R, et al. Benign meningioma developing late lung metastases: Case report and review of the literature. Clin Neuropathol 2009;28:453-9.
- 12 Kattner KA, Stroink AR, Roth TC, Lee JM. Rosai-Dorfman disease mimicking parasagittal meningioma: Case presentation and review of literature. Surg Neurol 2000;53:452-7.
Address for correspondence
Publication History
Article published online:
09 September 2022
© 2019. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Frydrychowicz C, Holland H, Hantmann H, Gradistanac T, Hoffmann KT, Mueller W, et al. Two cases of atypical meningioma with pulmonary metastases: A comparative cytogenetic analysis of chromosomes 1p and 22 and a review of the literature. Neuropathology 2015;35:175-83.
- 2 Mei Y, Bi WL, Greenwald NF, Agar NY, Beroukhim R, Dunn GP, et al. Genomic profile of human meningioma cell lines. PLoS One 2017;12:e0178322.
- 3 Forest F, Berremila SA, Gyenes C, Ginguéné C, Kassir R, Sulaiman A, et al. Metastatic meningiomas: An unusual clinical and pathological diagnosis with highly variable outcome. J Neurooncol 2014;120:411-21.
- 4 Mutnuru PC, Ahmed SF, Uppin SG, Lachi PK. Pulmonary metastases from intracranial meningioma. Lung India 2015;32:661-3.
- 5 Nakano M, Tanaka T, Nakamura A, Watanabe M, Kato N, Arai T, et al. Multiple pulmonary metastases following total removal of a bilateral parasagittal meningioma with complete occlusion of the superior sagittal sinus: Report of a case. Case Rep Neurol Med 2012;2012:121470.
- 6 Alexandru D, Glantz MJ, Kim L, Chamberlain MC, Bota DA. Pulmonary metastases in patients with recurrent, treatment-resistant meningioma: Prognosis and identification by 111Indium-octreotide imaging. Cancer 2011;117:4506-11.
- 7 Aumann JL, van den Bosch JM, Elbers JR, Wagenaar SJ. Metastatic meningioma of the lung. Thorax 1986;41:487-8.
- 8 Incarbone M, Ceresoli GL, Di Tommaso L, Cappuzzo F, Inzirillo F, Infante M, et al. Primary pulmonary meningioma: Report of a case and review of the literature. Lung Cancer 2008;62:401-7.
- 9 Kaminski JM, Movsas B, King E, Yang C, Kronz JD, Alli PM, et al. Metastatic meningioma to the lung with multiple pleural metastases. Am J Clin Oncol 2001;24:579-82.
- 10 Pramesh CS, Saklani AP, Pantvaidya GH, Heroor AA, Naresh KN, Sharma S, et al. Benign metastasizing meningioma. Jpn J Clin Oncol 2003;33:86-8.
- 11 Psaras T, Pantazis G, Steger V, Meyermann R, Honegger J, Beschorner R, et al. Benign meningioma developing late lung metastases: Case report and review of the literature. Clin Neuropathol 2009;28:453-9.
- 12 Kattner KA, Stroink AR, Roth TC, Lee JM. Rosai-Dorfman disease mimicking parasagittal meningioma: Case presentation and review of literature. Surg Neurol 2000;53:452-7.