

Subscribe to RSS
DOI: 10.4103/ajns.AJNS_203_17
Lateral semi-sitting position: A novel method of patient's head positioning in suboccipital retrosigmoid approaches
Authors

Background: The most common methods of positioning patients for suboccipital approaches are the lateral, lateral oblique, sitting, semisitting, supine with the head turn, and park bench. The literature on the positioning of patients for these approaches does not mention the use of lateral semisitting position. This position allows utilization of the benefits of both semisitting and lateral position without causing any additional morbidity to the patient. Aims: The aim of the present study is to highlight the advantages of the lateral semisitting position while operating various cerebellopontine angle (CPA) and posterior fossa lesions. Materials and Methods: The position involved placing the patient in a lateral position with torso flexed to 45° and head tilted toward opposite shoulder by 20°. The most common approach taken was retrosigmoid suboccipital craniotomy. Results: The advantages of lateral semisitting position were early decompression of cisterna magna, and the surgical field remained relatively clear, due to gravity-assisted drainage of blood and irrigating fluid. We could perform all the surgeries without the use of any retractors. The position allowed better delineation of surrounding structures resulting in achieving correct dissection plane and also permitted early caudal to cranial dissection of tumor capsule, thereby increasing chances of facial nerve preservation. Importantly, there is less engorgement of the cerebellum as the venous outflow is promoted. We have not experienced any increased rate of complications, such as venous air embolism, tension pneumocephalus with this lateral semisitting position. Conclusions: Lateral semisitting position is a relatively safe modification, which combines the benefits of semisitting and lateral position, and avoids the disadvantages of sitting position in operating CPA tumors. This position can provide quick and better exposure of the CPA without any significant complications.
Introduction
A retrosigmoid approach is a conventional approach for operating cerebellopontine angle (CPA) lesions. This route may be used in a variety of surgeries, such as CPA tumor removal, microvascular decompression, posterior inferior cerebellar artery (PICA) aneurysms, vestibular neurectomy, and brainstem auditory implantation.
The most common methods of positioning patients to operate CPA lesions include lateral, lateral oblique, sitting, semisiting, supine with the head turn, and park bench. The conventional supine position with head turn and park bench is being used by many surgeons as it simple and easy. The semisitting position is also being commonly used with good results. It allows drainage of the blood and wash fluid out of the wound rather than pooling in the surgical field.
We have been recently using a novel method of position to operate CPA lesions, i.e., lateral semisitting position which combines the benefits of both semi-sitting and lateral position without causing any additional morbidity to the patient and is comfortable for the surgeon and assistant.
Materials and Methods
Patient population
All patients undergoing neurosurgical intervention at our institute were prospectively enrolled in a database. Using this database, we identified 154 cases of various CPA lesions which were operated in lateral semisitting position in our hospital from 2015 to 2017.
Data collection
Clinical information was retrospectively reconstructed using patient medical records, radiologic data, and pathologic specimens. Both the preoperative, postcontrast T1-weighted magnetic resonance imaging (MRI) and the surgeon's operative note were reviewed to confirm tumor location in the CPA. The MRI was systematically reviewed to confirm tumor location, size, and IAC or jugular foramen involvement.
Perioperative management
Preoperative evaluation of all patients included T1-weighted/T2-weighted MRI with/without contrast. The use of contrast allows visualization of the extent of the tumor while T2-weighted MRI may display the arachnoid layer around the tumor, and adjacent brain edema, the latter giving some indications of adhesion to the surrounding parenchyma.
Positioning
The lateral semisitting position involved placing the patient in a lateral position first (side of tumor up) followed by flexing the torso to 45° and tilting head toward opposite shoulder by 20°. This was done to the point where the zygomatic arch is almost parallel to the floor. The chin should be 2 finger breadths away from the sternum as extreme flexion would compromise venous return from the head. The distance was kept between the planned incision and the patient's ipsilateral shoulder, which will otherwise limit the surgeon's range of motion later in the case.
The head was fixed with pins on the Mayfield clamp. As a final check before prepping and draping, the table was airplaned toward and away from anesthesia. This ensured that the patient was stable later in the case when the table would be manipulated to facilitate dissection distally along the 7th nerve and at the internal acoustic meatus.
Results
There were 154 patients with various CPA lesions in this series which were operated between 2015 and 2017. The age at diagnosis ranged from 16 years to 70 years. All were evaluated with computed tomography and MRI preoperatively. Pathology of all tumors was verified as follows: 73 schwannomas (47.4%), 40 (25.9%) CPA meningiomas, 26 CPA epidermoids (16.8%), 12 (7.79%) microvascular decompression for trigeminal neuralgia, 2 cases of PICA aneurysm, and one case of hemangioblastoma.
Suboccipital retrosigmoid approach was taken to operate all the CPA lesions in our series. All were operated with a surgical microscope and neurophysiological monitoring. We have not used any retractors to retract cerebellum in our series. Endoscopic assistance was taken to visualize the hidden areas of cerbellopontine angle in necessary cases.
Position related complications such as air embolism, tension pneumocephalus, postural hypotension, and pressure sore was not seen in any of our patients and ulnar neuropraxia was seen in only two patients.
There were no deaths related to surgical procedures in our series. However, surgical morbidity rates were high as follows: 27 (17.53%) patients had unilateral vocal cord palsy or dysphagia; eight were noted preoperatively. All had successful removal of nasogastric feeding from 1 month to 2 years (average 6 months). The tracheostomy and G-tube were removed between 4 months and 2 years (average 14 months) in all. 32 (20.77%) patients had seventh nerve palsy and 3 patients had fifth and sixth nerve dysfunctions.
Discussion
A plethora of tumors can occur in the CPA which derive from neuroglia tissues, cranial nerve sheaths, meninges, and embryonic remnants. According to Bonneville et al., vestibular schwannoma account for 70%–80% of all CPA lesions, 10%–15% meningiomas, and 5% epidermoid in adults.[[1]] In our study, the most common pathology involving the CPA was vestibular schwanomma followed by meningioma and epidermoid cyst. A retrosigmoid approach is a conventional approach for exploring the CPA lesions. It is the oldest approach to acoustic neuromas, first developed by Cushing and then redefined by Dandy in the premicrosurgical era.[[2]] This route may be used in a variety of surgeries, such as CPA tumor removal, microvascular decompression,[[3]] PICA aneurysms, vestibular neurectomy, and brainstem auditory implantation.
Positioning for retrosigmoid approach
The positioning of the surgical patient is an important part of surgery and attention to the physical and physiological consequences of positioning can help prevent serious adverse events and complications. The most common methods of positioning patients for retrosigmoid approaches are the lateral, Fukushima's position (lateral oblique), sitting, semisitting, supine with head turn, and park bench. Ideal patient positioning involves balancing surgical comfort, against the risks related to the patient position. A brief effort is made in this article to review the various methods of positioning in retrosigmoid approaches and highlight the advantages associated with our novel lateral semisitting position. This position can be added to the armamentarium of various positions used to operate CPA lesions by retrosigmoid route.
The lateral position was popularized by Sir Victor Horsley and Krause [[Figure 1]]. The advantages of the lateral position include lesser chances of air embolism and the ability of the surgeon to rest his elbows over the ipsilateral shoulder. The disadvantages of the lateral position are a need for continuous suctioning of blood and irrigation fluid during the surgery, need for retractors to retract cerebellum, brachial plexus injuries, and ventilation-perfusion mismatch. In the lateral position, the peritumoral veins cause troublesome intraoperative bleeding and thus require hemostasis.[[4]] Lateral positioning leads to gravitational changes of ventilation-perfusion relationship in the lung.

Sitting position was first introduced by De Martel in 1913 [[Figure 2]]a. The advantages of sitting position were lowered cerebral venous pressure and intracranial pressure during the surgery. This position promotes gravity drainage of blood and irrigation fluid thus keeping the surgical field clear at all times. Simultaneously, the disadvantages of placing the patient in sitting position include a high risk of tension pneumocephalus, venous air embolism, postural hypotension compounded with increased fatigue to the hands of a surgeon.
The modified sitting (semisitting) position advocated by Madjid Samii is a slight modification of sitting position [[Figure 2]]b. It provides better venous return and less hemodynamic instability. With head-up tilt, venous drainage via internal jugular veins is improved which results in decreased intracranial pressure. However, jugular veins may also collapse in sitting position, and careful head positioning to avoid hyperflexion and hyperextension is required to prevent stretching or obstruction of the vertebral venous outflow.
Three-Quarter Prone Position (Lateral Oblique, or Semiprone) also known as Fukushima position was advocated by Fukushima [[Figure 3]]. The benefit of this position is that the risk of venous air embolism is lower compared to the sitting position. The issues with hemodynamics and ventilation in this position are similar to those with lateral positioning. The principles of three-quarter positioning resemble those for a lateral position. Risks include bleeding, brachial plexus injury, pressure sores, and macroglossia.

In supine with head turn position,[[2]],[[4]] the head is turned to the contralateral side, and a sandbag is placed under the ipsilateral shoulder to rotate chest into semi-lateral position [[Figure 4]]. The advantages of this position are that it is simple, fast, and not related to major complications. The surgeon can sit at the surgical site of the patient's head with his or her feet under the table. An armrest for the surgeon may be placed for the arm near the vertex, and the surgeon's other arm rests on the patient. Besides the risks to the cervical spine, however, the rotation of the head can lead to venous outflow impediment with resultant raised intracranial pressure and parenchymal bleeding. The disadvantages with this position include, need for cerebellar retraction and continuous suctioning of the irrigating fluid during the surgery. The inadvertent extreme turning of the head can result in brainstem ischemia and brain swelling due to vertebral compression and jugular compression, respectively.

Alternatively, the patient can be positioned in the park-bench (three-quarter lateral) position, which does not endanger the cervical spine or venous drainage [[Figure 5]]. This position was advocated by Dr. Cone.[[5]] The Park-bench position is a modification of lateral position and provides the surgeon with better access to the posterior fossa, as compared to the lateral position. The head is flexed until there is 2–3 finger-breadths thyromental distance, rotated contralaterally to the lesion, and flexed 30° laterally toward the contralateral shoulder, allowing to increase the angle between the atlas and foramen magnum. The upper arm is positioned along the lateral trunk, and the dependent arm can be positioned in hanging or may be rested on a low padded arm board, inserted between the table and head fixator. Alternatively, the forearm can be hung on a pillow and towels wrapped over the arm and forearm.

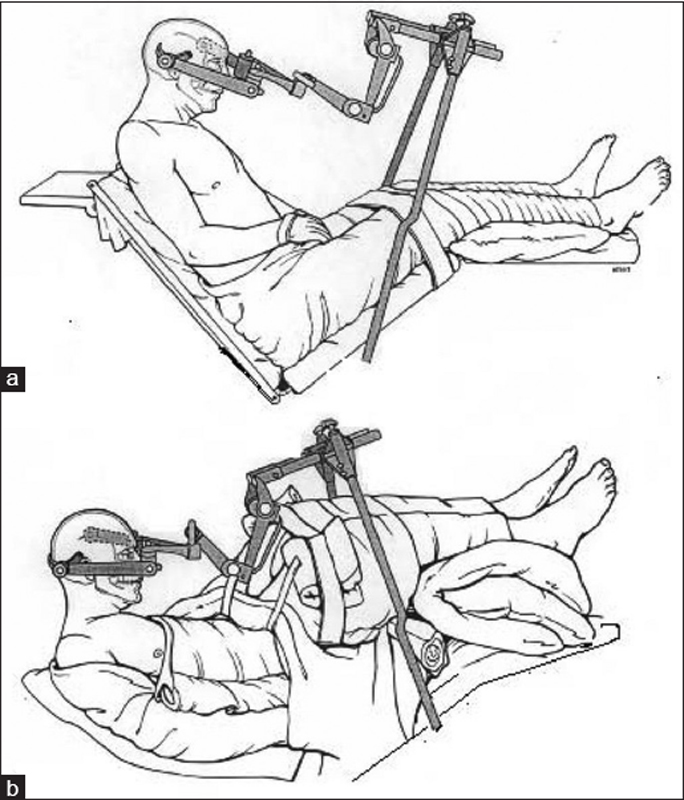
The pertinent literature on positioning patients for retrosigmoid approaches does not mention the use of lateral semisitting position. This position is different from the previously mentioned positions as it combines the advantages of both lateral and semisitting positions and avoids the disadvantages of sitting position. This position is a slight modification of the semi-sitting position in a way that the patient is placed first in dead lateral (side of tumor up) and then, the torso is flexed to 45° (semi-sitting), followed by head tilt toward opposite shoulder by 20°. This was done to the point where the zygomatic arch is almost parallel to the floor [[Figure 6]]a and [[Figure 6]]b. Then, the neck is flexed keeping in mind that the chin should be 2 finger breadths away from the sternum as extreme flexion would compromise venous return from the head.

Our lateral semisitting position allows utilization of the benefits of both sitting and lateral position without causing any additional morbidity to the patient. The surgical field remained relatively clear due to gravity assisted drainage of blood and irrigating fluid. Hence, there was no need of continuous suctioning. Cisterna magna could be drained of cerebrospinal fluid as soon the dura is opened, thus making the cerebellum lax which allowed us to carry out the whole surgery without any retractors. In the semisitting position, the reduced intracranial venous pressure shrinks the peritumoral vein, which prevents troublesome intraoperative bleeding. Ventilation in semisitting position is improved as compared to the supine position due to downward shift of the diaphragm, which improves ventilation of the dependent zones, and decreases ventilation-perfusion mismatch.
In lateral semisitting position, the surgeon can rest his forearm on the ipsilateral shoulder of the patient, thus reducing the fatigue while operating for longer duration. Many surgeons prefer the semisitting position for the retrosigmoid approach because it is more comfortable for the operator.[[6]],[[7]],[[8]] This position also permitted early caudal to cranial dissection of tumor capsule, thereby increasing chances of facial nerve preservation. Moreover, endoscopic assistance could be taken without any obstruction of the field.
We have operated CPA schwannomas, meningiomas, epidermoid cyst, microvascular decompressions, PICA aneurysms in this position. We have not experienced any increased rate of complications, such as venous air embolism, tension pneumocephalus, postural hypotension, pressure sores, brachial plexus injuries, cerebellar engorgement, and ventilation-perfusion mismatch as seen with previously described positions.
Conclusions
The lateral semisitting position is relatively a safe modification, which combines the benefits of both semisitting and lateral position without causing any additional morbidity to the patient and is comfortable for the surgeon and assistant. This method of patient positioning has allowed us to operate CPA tumors without the aid of cerebellar retractors. Neuroendoscopic assisted microneurosurgery can also be performed easily in this position.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Bonneville F, Savatovsky J, Chiras J. Imaging of cerebellopontine angle lesions: An update. Part 1: Enhancing extra-axial lesions. Eur Radiol 2007;17:2472-82.
- 2 Sampath P, Long DM. Acoustic neuromas. In: Winn RH, editor. Youmans neurological Surgery. 5th ed. Philadelphia: Saunders; 2004. p. 1147-68.
- 3 Sade B, Lee JH. Significance of the tentorial alignment in approaching the trigeminal nerve and the ventral petrous region through the suboccipital retrosigmoid technique. J Neurosurg 2007;107:932-6.
- 4 Yamakami I, Uchino Y, Kobayashi E, Yamaura A, Oka N. Removal of large acoustic neurinomas (vestibular schwannomas) by the retrosigmoid approach with no mortality and minimal morbidity. J Neurol Neurosurg Psychiatry 2004;75:453-8.
- 5 Gilbert RG, Brindle GF. Specific intracranial operations. Int Anesthesiol Clin 1966;4:829-61.
- 6 Samii M, Matthies C. Management of 1000 vestibular schwannomas (acoustic neuromas): Surgical management and results with an emphasis on complications and how to avoid them. Neurosurgery 1997;40:11-21.
- 7 Koos WT, Day JD, Matula C, Levy DI. Neurotopographic considerations in the microsurgical treatment of small acoustic neurinomas. J Neurosurg 1998;88:506-12.
- 8 Malis LI. Nuances in acoustic neuroma surgery. Neurosurgery 2001;49:337-41.
Address for correspondence
Publication History
Article published online:
09 September 2022
© 2019. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Bonneville F, Savatovsky J, Chiras J. Imaging of cerebellopontine angle lesions: An update. Part 1: Enhancing extra-axial lesions. Eur Radiol 2007;17:2472-82.
- 2 Sampath P, Long DM. Acoustic neuromas. In: Winn RH, editor. Youmans neurological Surgery. 5th ed. Philadelphia: Saunders; 2004. p. 1147-68.
- 3 Sade B, Lee JH. Significance of the tentorial alignment in approaching the trigeminal nerve and the ventral petrous region through the suboccipital retrosigmoid technique. J Neurosurg 2007;107:932-6.
- 4 Yamakami I, Uchino Y, Kobayashi E, Yamaura A, Oka N. Removal of large acoustic neurinomas (vestibular schwannomas) by the retrosigmoid approach with no mortality and minimal morbidity. J Neurol Neurosurg Psychiatry 2004;75:453-8.
- 5 Gilbert RG, Brindle GF. Specific intracranial operations. Int Anesthesiol Clin 1966;4:829-61.
- 6 Samii M, Matthies C. Management of 1000 vestibular schwannomas (acoustic neuromas): Surgical management and results with an emphasis on complications and how to avoid them. Neurosurgery 1997;40:11-21.
- 7 Koos WT, Day JD, Matula C, Levy DI. Neurotopographic considerations in the microsurgical treatment of small acoustic neurinomas. J Neurosurg 1998;88:506-12.
- 8 Malis LI. Nuances in acoustic neuroma surgery. Neurosurgery 2001;49:337-41.