

RSS-Feed abonnieren
DOI: 10.4103/ajns.AJNS_28_20
Expandable titanium cages in the emergent treatment of severe spinal deformity secondary to osteomyelitis: A series of three complex cases
Autor*innen

The literature lacks robust evidence on the benefits versus risks of instrumenting and fusing the spinal column in the setting of active osteomyelitis. We report three patients with vertebral osteomyelitis and subsequent severe and complex kyphotic deformities. Patients 1 and 2 had previous instrumentation that required revision because of hardware failure in the thoracic and thoracolumbar regions, respectively. Patient 3 developed a severe cervical kyphotic deformity at 2 months after being diagnosed and treated with antibiotics for osteomyelitis, necessitating emergent instrumentation and fusion. All the three patients are doing very well so far. Spinal instrumentation and fusion for correction of kyphotic deformity is sometimes necessary in the context of active osteomyelitis and should be done emergently and without hesitation when spinal cord injury from spinal instability is of concern.
Introduction
Deep infection of the spine is not an uncommon disease with various routes of dissemination such as hematogenous seeding,[[1]],[[2]] adjacent spread,[[3]] or iatrogenic inoculation from spinal procedures.[[4]] Current treatment algorithms often involve a prolonged course of antibiotics[[5]] and surgical debridement with or without instrumentation of the affected spine.[[6]] Instrumentation in patients with spinal infections complicated by spinal deformities has been an area of controversy given the treatment paradigm of refraining from implant use in the infected patient population.[[7]],[[8]],[[9]],[[10]],[[11]],[[12]] There is always the theoretical risk of pathogen seeding into the implants, rendering the infection more difficult to treat.
Spinal infections can be categorized into pyogenic and nonpyogenic.[[7]] Pyogenic infections typically respond well to conservative management, although more advanced conditions such as mechanical spinal instability usually require surgical intervention. The main concern with these pyogenic pathogens is the formation of biofilms.[[10]] Although this concern has been confirmed in appendicular arthroplasty surgery,[[11]] it has not been shown to be conclusive in spinal instrumentation.[[12]] In contrary to appendicular arthroplasty, spinal instrumentation actually confers advantages to the patient when the stability of the spine is a concern despite the risk of biofilm formation.[[7]],[[8]],[[13]],[[14]],[[15]],[[16]] Therefore, there has been a paradigm shift in the field of spinal surgery over the past two decades, prioritizing the placement and preservation of instrumentation whenever indicated.[[17]],[[18]]
The main indications for surgical debridement/irrigation and instrumentation include spinal cord compression, neurologic compromise, significant deformity, spinal instability, and failure of medical management.[[19]],[[20]],[[21]],[[22]],[[23]] Surgical intervention with radial debridement and instrumentation allows for maintenance of sagittal alignment, reduction in prolonged periods of bed rest, and stabilization of the spine. We present three cases of patients with severe and complex spinal deformities in the setting of active osteomyelitis. The objective of this article is to highlight the management of patients with impending or worsening spinal instability requiring instrumentation in the setting of an active infection.
Case Series
Patient 1
Patient 1 is a 31-year-old female with a known history of intravenous drug use (IVDU), bipolar disorder, and hepatitis C, who presented to our institution on January 10, 2018, for the evaluation of back pain. She has had T5-9 laminectomies performed at another institution in 2016 for spinal epidural abscesses. Workup at our hospital showed findings concerning for T5-6 osteomyelitis with significant kyphotic deformity [[Figure 1]]. The patient was neurologically intact on examination. At that time, infectious markers were elevated with a C-reactive protein (CRP) of 5.1 and erythrocyte sedimentation rate (ESR) of 74, and the patient was started on empiric antibiotic therapy. Her current condition was very concerning for the progression of spinal deformity; thus, the decision was made to proceed with stabilization in the setting of active osteomyelitis. She underwent transpedicular corpectomies at T5-6 with instrumentation and fusion from T1 to T11 [[Figure 2]]. The patient remained neurologically intact postoperatively, although she was involved in several incidents of drug paraphernalia during her hospital stay. She was discharged on February 13, 2018, with upright X-ray images showing a stable spinal alignment [[Figure 3]].



The patient was lost to follow-up until December 7, 2019. In the interim, she presented to another hospital on April 30, 2019, for osteomyelitis and kyphotic deformity at T10–11, for which she had an extension of her hardware to L4 [[Figure 4]] and [[Figure 5]]. She also endorsed noncompliance with her oral antibiotic regimen and IVDU. The patient returned to our care because of purulent discharge from exposed hardware at the proximal end of her construct that she noticed 1–2 weeks earlier [[Figure 6]]. Imaging during this hospital admission showed worsening of the kyphotic deformity and complete spondyloptosis of T9 over T11 [[Figure 7]], with a surprisingly intact neurological examination. Her body mass index was 14. The patient was presented at our spine conference, and the decision was made to proceed with surgery, again for concern of a catastrophic event if spinal stability is not attained promptly.

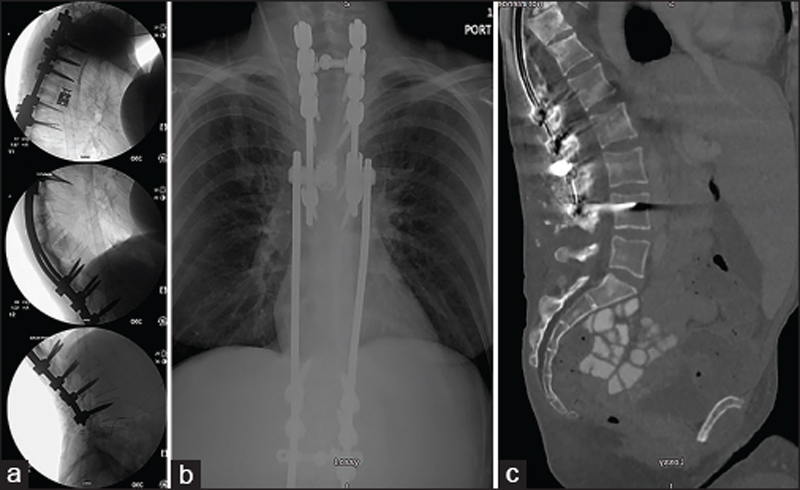


She then underwent removal of previous hardware and a T10–11 transpedicular corpectomy. An expandable cage with large endcaps spanning the full width and resting on the epiphyseal rings of the vertebral bodies was placed in the corpectomy defect [[Figure 8]]. During the reduction of kyphosis, intraoperative monitoring showed a decrease in the right lower extremity motor-evoked potential signals. The signals, however, returned to normal by increasing the mean arterial pressure (MAP) >90 mmHg. The plastic surgery team assisted with the closure of the incision.

Postoperatively, the MAP was kept at >90 mmHg for 5 days, after which she returned to baseline function in the lower extremities and was able to ambulate on postoperative day (POD) 13. Upright X-ray images were performed in a brace and are shown in [[Figure 9]]. We hope that she will continue to follow-up at our clinic for continued care and monitoring of spinal stability.

Patient 2
Patient 2 is a 55-year-old male with a known history of IVDU and chronic low back pain after a motor vehicle accident in 2016, who presented to our care for the evaluation of worsening lower back pain and a protrusion in his back when he bends forward. The patient had a previous L1 kyphoplasty for a compression fracture in early 2017, after which he continued to have pain, failed conservative management, and opted for surgical intervention. In May 2017, the patient underwent a T10–L3 fusion with laminectomies between T12 and L1 at another institution. He was then lost to follow-up.
On January 4, 2018, the patient presented to our hospital with complaints of back pain and protruded hardware. Imaging studies revealed proximal junctional kyphosis/hardware failure with a new compression fracture at T12 and almost complete resorption of L1. The construct was dislocated out of the vertebral body at the cranial end on the right. A rod fracture was also noted on the contralateral side at the inferior end of the instrumentation [[Figure 10]]. There was also a concern for an underlying infection at T12, L1, and L2 vertebral bodies, and the patient was started on broad-spectrum antibiotics at that time.

The decision was made to perform a two-staged procedure. The first stage included irrigation and debridement of infected tissue, removal of all previous hardware, attainment of better spinal alignment with Ponte osteotomies, and placement of new posterior instrumentation for fusion from T8 to the iliac bones. The second stage was performed through a minimally invasive lateral retropleural/retroperitoneal approach for a 3-level corpectomy between T12-L2 and placement of an expandable cage and a lateral plate [[Figure 11]]. Hemovac drains were placed posteriorly to help with drainage of the infection.

Although the intraoperative neuromonitoring signals were stable throughout the surgery, the patient woke up with a transient lower extremity weakness. Intraoperative cultures were positive for Staphylococcus epidermidis. He was discharged from the hospital on POD 6 on long-term antibiotic suppression therapy. He did not come back for follow-up until May 30, 2018, where new imaging studies showed a stable construct [[Figure 12]]. His last office visit was at 20 months after the surgery, during which he reported no back or leg pain, and standing scoliosis X-rays again showed stable hardware [[Figure 13]].


Patient 3
Patient 3 is a 36-year-old male with a known history of IVDU and hepatitis C who presented to our care with neck pain and fatigue. He was diagnosed with a C2–T1 epidural abscess and C6–7 osteomyelitis in August 2019. Blood cultures were consistently positive for Staphylococcus epidermidis. He received intravenous antibiotics at a skilled nursing facility for 4 weeks, after which the he discontinued his oral antibiotic regime without consulting his physician.
On presentation in October 2019, the patient was complaining of intermittent lower extremity weakness with C8 dermatomal numbness that progressed over several weeks. Neurological examination showed hyperreflexia in the lower extremities as well as positive Babinski sign bilaterally. Imaging studies revealed a significant kyphotic deformity at C6–7 [[Figure 14]]. Infectious disease markers were normal, with a CRP of 0.09 and ESR of 2.

He was taken to the operating room and placed in traction under intraoperative fluoroscopy to obtain appropriate alignment before proceeding with surgery. We were not able to reduce the kyphosis with an initial traction. The patient was then placed in prone positioning and pedicle screws were placed between C3–5 and T1–2 bilaterally. Bilateral Ponte osteotomies were also performed at C6–7. The patient was then flipped to the supine positioning, a C6–7 corpectomy was performed, an expandable cage was placed in the corpectomy defect, a plate was fixed anteriorly between C5 and C8, and the kyphotic deformity was corrected. Then, the patient was flipped back to the prone positioning, and the rods were applied posteriorly. Prior to all instrumentation, cultures were taken, and the surgical sites were irrigated with copious amounts of warm saline and bacitracin. Closed-suction hemovac drains were placed both anteriorly and posteriorly.
X-ray images of the final construct in place were obtained [[Figure 15]], and the patient was started on vancomycin and ceftriaxone. None of the cultures showed any growth. The patient had improvement in his lower extremities at discharge with a resolution of the C8 dermatomal numbness. He is scheduled to follow-up at our clinic in the coming months for postoperative care.

Discussion
The three patients of this series represent typical cases of the dilemma that surgeons usually face in the decision-making process of whether to instrument and fuse a patient with active spinal osteomyelitis, the goal of which is to preserve spinal alignment or correct deformity, mitigate unrelenting pain, and prevent neurological deterioration. In patients with primary spinal infections, there is a universal belief that instrumented stabilization should be performed when indications are met. Contrary to guidelines followed by other surgical fields,[[11]],[[24]],[[25]],[[26]],[[27]],[[28]] retaining, revising, or placing instrumentation in the setting of primary spinal infection is becoming more common.[[6]],[[7]],[[8]],[[9]],[[12]],[[13]],[[14]],[[15]],[[19]],[[20]],[[21]],[[23]],[[29]],[[30]]
Epidemiologic data for spinal infections revealed an increasing incidence that appears to coincide with an increase in IVDU and the use of immunosuppressive therapy.[[29]],[[31]],[[32]] The ever-changing antimicrobial resistance patterns and an increasingly sick patient population may all play a significant role in this clinical problem. From an economic standpoint, the cost associated with the diagnostic studies, surgical therapies, and lost productivity time remains significant. From a patient perspective, delays in diagnosis and care can lead to significant disability or even death.[[33]] Guidelines for the diagnosis and treatment of de novo spine infections are still absent due to the lack of larger supportive studies with significant power.[[34]] Currently, the literature supports spinal instrumentation in immunocompromised patients with pyogenic vertebral osteomyelitis as it is associated with a low risk of long-term or recurrent infection.[[29]]
Patients 1 and 2 had previous instrumentation that required revision because of hardware failure. However, the lesson learned from patient three who developed a cervical kyphotic deformity is that appropriate antibiotic therapy may be able to treat the infection, but it may not be able to prevent the development of mechanical instability. For some patients, therefore, the benefits of spinal stabilization outweigh the potential risks of infection relapse, reoperation, or increased overall morbidity and mortality.[[14]] In all the three patients, dynamic X-ray images are contraindicated preoperatively due to the obvious instability and high risk of spinal cord injury. However, we do obtain dynamic X-rays in these patients routinely at 3 months of follow-up to confirm the stability of the construct. Close follow-up with ESR and/or CRP is also recommended in the postoperative period, especially in patients with persistent infection, as confirmed by cultures from intraoperative samples. New inflammatory markers may be helpful in cases of inconclusive ESR and CRP levels and high clinical suspicion of continued infection or potential sepsis.[[35]]
For a long time, the dogma in surgery has been to remove the hardware in the setting of an active infection for fear of biofilm formation and the subsequent inability to eradicate the infection; placement of new instrumentation in the setting of an active infection at the surgical site is even less likely to be pursued.[[36]],[[37]],[[38]] These beliefs primarily evolved in the literature of other surgical subspecialties.[[11]],[[24]],[[25]],[[26]],[[27]],[[28]] Nevertheless, a dissenting opinion throughout the spinal surgery community has made these two concepts controversial, where hardware removal in early infections can cause instability and progressive deformity.[[30]],[[37]] Removing the hardware without new instrumentation would not have been appropriate or feasible in the three patients of this series due to the severity of their deformities and impending spinal cord injury. These three patients were fortunate to present with the intact neurological examination; otherwise, spinal cord injury might have been irreversible at the time of presentation. In recent years, direct spinal fixation following debridement of both pyogenic and nonpyogenic infections has been conducted, where fixation in conjunction with aggressive antibiotic regimens resulted in the healing of many spinal infections.[[6]],[[7]],[[8]],[[9]],[[12]],[[13]],[[14]],[[15]],[[19]],[[20]],[[21]],[[23]],[[29]],[[30]] It is also worth noting that despite the presence of a fusion mass on imaging, there have been cases of patients losing their spinal corrections after hardware removal.[[30]],[[37]]
Conclusion
Spinal instrumentation and fusion for correction of kyphotic deformity is sometimes necessary in the context of active osteomyelitis and should be done emergently and without hesitation when spinal cord injury from spinal instability is of concern. The benefits of spinal stabilization outweigh the potential risks of infection relapse, reoperation, or increased overall morbidity and mortality. Large controlled studies are dearly needed to establish evidence-based guidelines related to this topic, especially that microbial flora patterns and biofilm formation vary from center to center and region to region, which may have some influence in the decision-making process.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Batson OV. The function of the vertebral veins and their role in the spread of metastases. Ann Surg 1940;112:138-49.
- 2 Wiley AM, Trueta J. The vascular anatomy of the spine and its relationship to pyogenic vertebral osteomyelitis. J Bone Joint Surg Br 1959;41-B:796-809.
- 3 Darouiche RO. Spinal epidural abscess. N Engl J Med 2006;355:2012-20.
- 4 Nussbaum ES, Rigamonti D, Standiford H, Numaguchi Y, Wolf AL, Robinson WL. Spinal epidural abscess: A report of 40 cases and review. Surg Neurol 1992;38:225-31.
- 5 Savage K, Holtom PD, Zalavras CG. Spinal epidural abscess: Early clinical outcome in patients treated medically. Clin Orthop Relat Res 2005;439:56-60.
- 6 Karikari IO, Powers CJ, Reynolds RM, Mehta AI, Isaacs RE. Management of a spontaneous spinal epidural abscess: A single-center 10-year experience. Neurosurgery 2009;65:919-23.
- 7 Lee MC, Wang MY, Fessler RG, Liauw J, Kim DH. Instrumentation in patients with spinal infection. Neurosurg Focus 2004;17:E7.
- 8 Rayes M, Colen CB, Bahgat DA, Higashida T, Guthikonda M, Rengachary S, et al. Safety of instrumentation in patients with spinal infection. J Neurosurg Spine 2010;12:647-59.
- 9 Dennis Hey HW, Nathaniel Ng LW, Tan CS, Fisher D, Vasudevan A, Liu KG, et al. Spinal Implants Can Be Inserted in Patients With Deep Spine Infection: Results From a Large Cohort Study. Spine (Phila Pa 1976) 2017;42:E490-5.
- 10 Brady RA, Leid JG, Calhoun JH, Costerton JW, Shirtliff ME. Osteomyelitis and the role of biofilms in chronic infection. FEMS Immunol Med Microbiol 2008;52:13-22.
- 11 Tattevin P, Crémieux AC, Pottier P, Huten D, Carbon C. Prosthetic joint infection: When can prosthesis salvage be considered? Clin Infect Dis 1999;29:292-5.
- 12 Kowalski TJ, Berbari EF, Huddleston PM, Steckelberg JM, Mandrekar JN, Osmon DR. The management and outcome of spinal implant infections: Contemporary retrospective cohort study. Clin Infect Dis 2007;44:913-20.
- 13 Rezai AR, Woo HH, Errico TJ, Cooper PR. Contemporary management of spinal osteomyelitis. Neurosurgery 1999;44:1018-25.
- 14 Dimar JR, Carreon LY, Glassman SD, Campbell MJ, Hartman MJ, Johnson JR. Treatment of pyogenic vertebral osteomyelitis with anterior debridement and fusion followed by delayed posterior spinal fusion. Spine (Phila Pa 1976) 2004;29:326-32.
- 15 Redfern RM, Miles J, Banks AJ, Dervin E. Stabilisation of the infected spine. J Neurol Neurosurg Psychiatry 1988;51:803-7.
- 16 Broner FA, Garland DE, Zigler JE. Spinal infections in the immunocompromised host. Orthop Clin North Am 1996;27:37-46.
- 17 Atesok K, Vaccaro A, Stippler M, Striano BM, Carr M, Heffernan M, et al. Fate of hardware in spinal infections. Surg Infect (Larchmt) 2019. doi.org/10.1089/sur.2019.206.
- 18 Kalfas F, Severi P, Scudieri C. Infection with spinal instrumentation: A 20-year, single-institution experience with review of pathogenesis, diagnosis, prevention, and management. Asian J Neurosurg 2019;14:1181-9.
- 19 Nagashima H, Tanishima S, Tanida A. Diagnosis and management of spinal infections. J Orthop Sci 2018;23:8-13.
- 20 Shenoy K, Singla A, Krystal JD, Razi AE, Kim YH, Sharan AD. Discitis in adults. JBJS Rev 2018;6:e6.
- 21 Duarte RM, Vaccaro AR. Spinal infection: State of the art and management algorithm. Eur Spine J 2013;22:2787-99.
- 22 Mylona E, Samarkos M, Kakalou E, Fanourgiakis P, Skoutelis A. Pyogenic vertebral osteomyelitis: A systematic review of clinical characteristics. Semin Arthritis Rheum 2009;39:10-7.
- 23 Rutges JP, Kempen DH, van Dijk M, Oner FC. Outcome of conservative and surgical treatment of pyogenic spondylodiscitis: A systematic literature review. Eur Spine J 2016;25:983-99.
- 24 Rasouli MR, Viola J, Maltenfort MG, Shahi A, Parvizi J, Krieg JC. Hardware removal due to infection after open reduction and internal fixation: Trends and predictors. Arch Bone Jt Surg 2015;3:184-92.
- 25 Shah MQ, Zardad MS, Khan A, Ahmed S, Awan AS, Mohammad T. Surgical site infection in orthopaedic implants and its common bacteria with their sensitivities to antibiotics, in open reduction internal fixation. J Ayub Med Coll Abbottabad 2017;29:50-3.
- 26 Romanos GE, Javed F, Delgado-Ruiz RA, Calvo-Guirado JL. Peri-implant diseases: A review of treatment interventions. Dent Clin North Am 2015;59:157-78.
- 27 Lawrenz JM, Frangiamore SJ, Rane AA, Cantrell WA, Vallier HA. Treatment approach for infection of healed fractures after internal fixation. J Orthop Trauma 2017;31:e358-e363.
- 28 Feihl S, Renz N, Schütz M, Müller M. Antibiotic strategies in trauma surgery: Treatment of implant-associated infections. Unfallchirurg 2017;120:486-93.
- 29 Carragee E, Iezza A. Does acute placement of instrumentation in the treatment of vertebral osteomyelitis predispose to recurrent infection: Long-term follow-up in immune-suppressed patients. Spine (Phila Pa 1976) 2008;33:2089-93.
- 30 Lall RR, Wong AP, Lall RR, Lawton CD, Smith ZA, Dahdaleh NS. Evidence-based management of deep wound infection after spinal instrumentation. J Clin Neurosci 2015;22:238-42.
- 31 Issa K, Diebo BG, Faloon M, Naziri Q, Pourtaheri S, Paulino CB, et al. The epidemiology of vertebral osteomyelitis in the United States from 1998 to 2013. Clin Spine Surg 2018;31:E102-8.
- 32 Blecher R, Yilmaz E, Ishak B, Drazin D, Oskouian RJ, Chapman JR. Recent increase in the rate of spinal infections may be related to growing substance-use disorder in the state of Washington: Wide population-based analysis of the Comprehensive Hospital Abstract Reporting System (CHARS) Database. Spine (Phila Pa 1976) 2019;44:291-7.
- 33 Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: Risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J 2014;14:326-30.
- 34 Farber SH, Murphy KR, Suryadevara CM, Babu R, Yang S, Feng L, et al. Comparing outcomes of early, late, and non-surgical management of intraspinal abscess. J Clin Neurosci 2017;36:64-71.
- 35 da Silva GG, da Gomes Cunha DM, Hamasaki MY. New biomarkers of sepsis with clinical relevance. Clinical Management of Shock-The Science and Art of Physiological Restoration. Lodon: IntechOpen; 2019.
- 36 Darouiche RO, Hamill RJ, Greenberg SB, Weathers SW, Musher DM. Bacterial spinal epidural abscess. Review of 43 cases and literature survey. Medicine (Baltimore) 1992;71:369-85.
- 37 Kasliwal MK, Tan LA, Traynelis VC. Infection with spinal instrumentation: Review of pathogenesis, diagnosis, prevention, and management. Surg Neurol Int 2013;4:S392-403.
- 38 Rigamonti D, Liem L, Sampath P, Knoller N, Namaguchi Y, Schreibman DL, et al. Spinal epidural abscess: Contemporary trends in etiology, evaluation, and management. Surg Neurol 1999;52:189-96.
Address for correspondence
Publikationsverlauf
Eingereicht: 21. Januar 2020
Angenommen: 11. März 2020
Artikel online veröffentlicht:
16. August 2022
© 2020. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Batson OV. The function of the vertebral veins and their role in the spread of metastases. Ann Surg 1940;112:138-49.
- 2 Wiley AM, Trueta J. The vascular anatomy of the spine and its relationship to pyogenic vertebral osteomyelitis. J Bone Joint Surg Br 1959;41-B:796-809.
- 3 Darouiche RO. Spinal epidural abscess. N Engl J Med 2006;355:2012-20.
- 4 Nussbaum ES, Rigamonti D, Standiford H, Numaguchi Y, Wolf AL, Robinson WL. Spinal epidural abscess: A report of 40 cases and review. Surg Neurol 1992;38:225-31.
- 5 Savage K, Holtom PD, Zalavras CG. Spinal epidural abscess: Early clinical outcome in patients treated medically. Clin Orthop Relat Res 2005;439:56-60.
- 6 Karikari IO, Powers CJ, Reynolds RM, Mehta AI, Isaacs RE. Management of a spontaneous spinal epidural abscess: A single-center 10-year experience. Neurosurgery 2009;65:919-23.
- 7 Lee MC, Wang MY, Fessler RG, Liauw J, Kim DH. Instrumentation in patients with spinal infection. Neurosurg Focus 2004;17:E7.
- 8 Rayes M, Colen CB, Bahgat DA, Higashida T, Guthikonda M, Rengachary S, et al. Safety of instrumentation in patients with spinal infection. J Neurosurg Spine 2010;12:647-59.
- 9 Dennis Hey HW, Nathaniel Ng LW, Tan CS, Fisher D, Vasudevan A, Liu KG, et al. Spinal Implants Can Be Inserted in Patients With Deep Spine Infection: Results From a Large Cohort Study. Spine (Phila Pa 1976) 2017;42:E490-5.
- 10 Brady RA, Leid JG, Calhoun JH, Costerton JW, Shirtliff ME. Osteomyelitis and the role of biofilms in chronic infection. FEMS Immunol Med Microbiol 2008;52:13-22.
- 11 Tattevin P, Crémieux AC, Pottier P, Huten D, Carbon C. Prosthetic joint infection: When can prosthesis salvage be considered? Clin Infect Dis 1999;29:292-5.
- 12 Kowalski TJ, Berbari EF, Huddleston PM, Steckelberg JM, Mandrekar JN, Osmon DR. The management and outcome of spinal implant infections: Contemporary retrospective cohort study. Clin Infect Dis 2007;44:913-20.
- 13 Rezai AR, Woo HH, Errico TJ, Cooper PR. Contemporary management of spinal osteomyelitis. Neurosurgery 1999;44:1018-25.
- 14 Dimar JR, Carreon LY, Glassman SD, Campbell MJ, Hartman MJ, Johnson JR. Treatment of pyogenic vertebral osteomyelitis with anterior debridement and fusion followed by delayed posterior spinal fusion. Spine (Phila Pa 1976) 2004;29:326-32.
- 15 Redfern RM, Miles J, Banks AJ, Dervin E. Stabilisation of the infected spine. J Neurol Neurosurg Psychiatry 1988;51:803-7.
- 16 Broner FA, Garland DE, Zigler JE. Spinal infections in the immunocompromised host. Orthop Clin North Am 1996;27:37-46.
- 17 Atesok K, Vaccaro A, Stippler M, Striano BM, Carr M, Heffernan M, et al. Fate of hardware in spinal infections. Surg Infect (Larchmt) 2019. doi.org/10.1089/sur.2019.206.
- 18 Kalfas F, Severi P, Scudieri C. Infection with spinal instrumentation: A 20-year, single-institution experience with review of pathogenesis, diagnosis, prevention, and management. Asian J Neurosurg 2019;14:1181-9.
- 19 Nagashima H, Tanishima S, Tanida A. Diagnosis and management of spinal infections. J Orthop Sci 2018;23:8-13.
- 20 Shenoy K, Singla A, Krystal JD, Razi AE, Kim YH, Sharan AD. Discitis in adults. JBJS Rev 2018;6:e6.
- 21 Duarte RM, Vaccaro AR. Spinal infection: State of the art and management algorithm. Eur Spine J 2013;22:2787-99.
- 22 Mylona E, Samarkos M, Kakalou E, Fanourgiakis P, Skoutelis A. Pyogenic vertebral osteomyelitis: A systematic review of clinical characteristics. Semin Arthritis Rheum 2009;39:10-7.
- 23 Rutges JP, Kempen DH, van Dijk M, Oner FC. Outcome of conservative and surgical treatment of pyogenic spondylodiscitis: A systematic literature review. Eur Spine J 2016;25:983-99.
- 24 Rasouli MR, Viola J, Maltenfort MG, Shahi A, Parvizi J, Krieg JC. Hardware removal due to infection after open reduction and internal fixation: Trends and predictors. Arch Bone Jt Surg 2015;3:184-92.
- 25 Shah MQ, Zardad MS, Khan A, Ahmed S, Awan AS, Mohammad T. Surgical site infection in orthopaedic implants and its common bacteria with their sensitivities to antibiotics, in open reduction internal fixation. J Ayub Med Coll Abbottabad 2017;29:50-3.
- 26 Romanos GE, Javed F, Delgado-Ruiz RA, Calvo-Guirado JL. Peri-implant diseases: A review of treatment interventions. Dent Clin North Am 2015;59:157-78.
- 27 Lawrenz JM, Frangiamore SJ, Rane AA, Cantrell WA, Vallier HA. Treatment approach for infection of healed fractures after internal fixation. J Orthop Trauma 2017;31:e358-e363.
- 28 Feihl S, Renz N, Schütz M, Müller M. Antibiotic strategies in trauma surgery: Treatment of implant-associated infections. Unfallchirurg 2017;120:486-93.
- 29 Carragee E, Iezza A. Does acute placement of instrumentation in the treatment of vertebral osteomyelitis predispose to recurrent infection: Long-term follow-up in immune-suppressed patients. Spine (Phila Pa 1976) 2008;33:2089-93.
- 30 Lall RR, Wong AP, Lall RR, Lawton CD, Smith ZA, Dahdaleh NS. Evidence-based management of deep wound infection after spinal instrumentation. J Clin Neurosci 2015;22:238-42.
- 31 Issa K, Diebo BG, Faloon M, Naziri Q, Pourtaheri S, Paulino CB, et al. The epidemiology of vertebral osteomyelitis in the United States from 1998 to 2013. Clin Spine Surg 2018;31:E102-8.
- 32 Blecher R, Yilmaz E, Ishak B, Drazin D, Oskouian RJ, Chapman JR. Recent increase in the rate of spinal infections may be related to growing substance-use disorder in the state of Washington: Wide population-based analysis of the Comprehensive Hospital Abstract Reporting System (CHARS) Database. Spine (Phila Pa 1976) 2019;44:291-7.
- 33 Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: Risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J 2014;14:326-30.
- 34 Farber SH, Murphy KR, Suryadevara CM, Babu R, Yang S, Feng L, et al. Comparing outcomes of early, late, and non-surgical management of intraspinal abscess. J Clin Neurosci 2017;36:64-71.
- 35 da Silva GG, da Gomes Cunha DM, Hamasaki MY. New biomarkers of sepsis with clinical relevance. Clinical Management of Shock-The Science and Art of Physiological Restoration. Lodon: IntechOpen; 2019.
- 36 Darouiche RO, Hamill RJ, Greenberg SB, Weathers SW, Musher DM. Bacterial spinal epidural abscess. Review of 43 cases and literature survey. Medicine (Baltimore) 1992;71:369-85.
- 37 Kasliwal MK, Tan LA, Traynelis VC. Infection with spinal instrumentation: Review of pathogenesis, diagnosis, prevention, and management. Surg Neurol Int 2013;4:S392-403.
- 38 Rigamonti D, Liem L, Sampath P, Knoller N, Namaguchi Y, Schreibman DL, et al. Spinal epidural abscess: Contemporary trends in etiology, evaluation, and management. Surg Neurol 1999;52:189-96.