

Subscribe to RSS
DOI: 10.4103/ajns.AJNS_43_19
Interhemispheric approach to anterior communicating artery aneurysm: A case illustration
Authors

There are two main types of approaches for anterior communicating artery (AcomA) aneurysms, namely pterional approach, and an interhemispheric (IH) approach. Pterional approach is the most common for anterior circulation aneurysms. However, this approach cannot be used without resection of gyrus rectus when aneurysm is located high within the IH fissure and directed posterosuperiorly, which is better handled with IH approach. In this article, we will describe the tricks of IH approach with a case illustration.
Key-words:
Anterior communicating artery aneurysm - distal anterior cerebral artery aneurysm - interhemispheric approachIntroduction
The pterional approach is the most common for anterior circulation aneurysms. It has certain advantages such as bilateral parent artery of the proximal side can be secured in the early stage of the process and damage to the olfactory nerve is minimal. However, this approach cannot be used without resection of gyrus rectus when aneurysm is located high within the interhemispheric (IH) fissure and directed posterosuperiorly, which is better handled with IH route. Majority of distal anterior cerebral artery aneurysms are located along the corpus callosum especially the rostrum part, so the anterior IH approach represents the most common way to reach them.[[1]] For anterior communicating artery (AcomA) aneurysm, more proximal exposure in IH fissure under the rostrum of the corpus callosum is required for better visualization which is achieved with a craniotomy placed more frontally.[[2]],[[3]],[[4]] There are some variations for the IH approach including bifrontal, unifrontal, basal IH, and transcristagalli interfalcine approaches. Each subtype will be discussed under the discussion section. In this article, we will describe the tricks of unifrontal IH approach with a case illustration.
Case Report
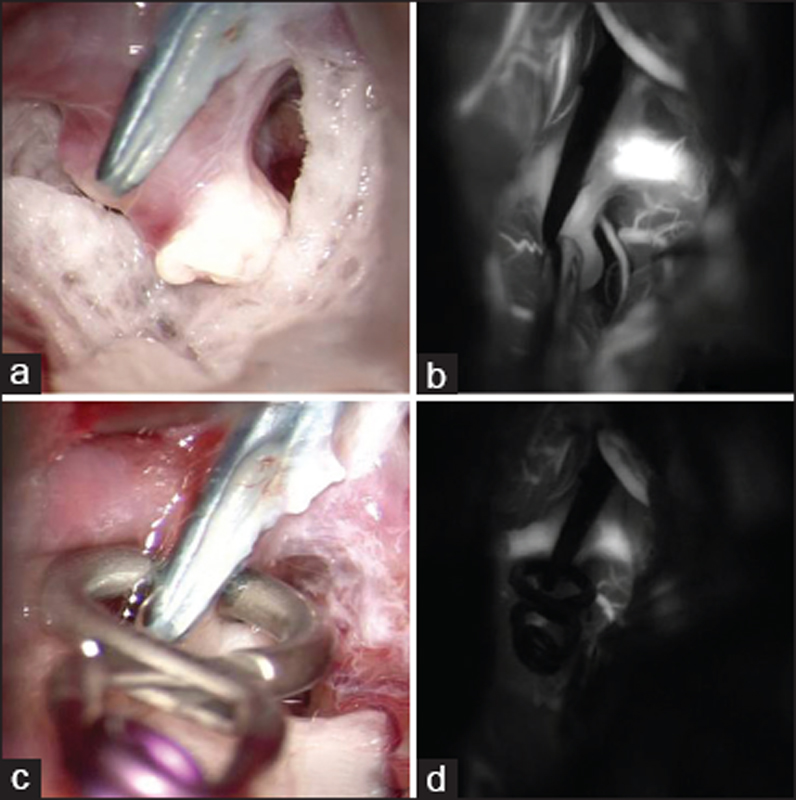
A 42-year-old female with a history of previously clipped AcomA aneurysm 1 year back, on routine follow-up, was found to have recurrence of aneurysm at previously clipped site. She was operated through pterional route for a posterosuperiorly directed AcomA aneurysm during fast surgery. Three-dimensional-rotational computed tomography angiography confirmed it to be located at previously clipped AcomA site directing posterosuperiorly [[Figure 1]]a. The computational fluid dynamic study was suggestive of impending rupture [[Figure 1]]b. An unifrontal IH approach was chosen for her. She was positioned supine with head slightly extended and fixed with a head frame. Bicoronal skin incision was given 1 cm behind hairline. Subperiosteal dissection of the skin flap was extended to the glabella and the orbital ridge. Supraorbital nerves were preserved. Four burr holes were made [[Figure 1]]c. A bifrontal craniotomy was done crossing the midline. Dura was dissected carefully not to injure sinus with blunt dissectors. Bleeding from sinus was controlled with Gelfoam and fibrin glue. The frontal sinus was opened up during craniotomy. The mucous membrane in the sinus was dissected and cauterized. The inner table of sinus and crista galli was removed with rongeur and drill [[Figure 1]]d. The right frontal dura opened with pedicle toward sinus. Arachnoid was dissected away with care to preserve bridging veins and continued along the margin of falx [[Figure 2]]a. The cerebrospinal fluid (CSF) release obtained with subarachnoid dissection allowed gradual brain relaxation and wider surgical exposure. The initial step was to identify lower margin of falx and the upper surface of corpus callosum with the help of pericallosal artery. The corpus callosum must be differentiated from cingulated gyri by its glistening surface, pearly white color and parallel running transverse fibers. Once pericallosal artery was identified, then IH dissection was continued following pericallosal artery under the rostrum of the corpus callosum up to AComA complex [[Figure 2]]b, [[Figure 2]]c, [[Figure 2]]d. [[Figure 2]]c shows the trajectory of the operative view. The aneurysm was sharply dissected from surrounding adhesions, out of previous surgery [[Figure 3]]a. In this approach, we were able to dissect bilateral A1 and A2 with AcomA aneurysm clearly [[Figure 3]]b. Fenestrated clip applied to occlude the neck of aneurysm completely [[Figure 3]]c. Complete occlusion of aneurysm neck and flow in hypothalamic perforators was confirmed with post-clipping indocyanine green video angiography and endoscopy [[Figure 3]]d and [[Figure 4]]a, [[Figure 4]]b, [[Figure 4]]c. The dura was tightly closed in a waterproof manner. Tack-up sutures were placed at the dura to the craniotomy edge, to minimize the risk of postoperative epidural hematoma. The bone flap was replaced and fixed using microplates. The postoperative period was uneventful without any neurological deficit. Till now, we have operated three cases of recurrent postsuperiorly directed AcomA aneurysm through this route with good neurological outcome.



Discussion
Unifrontal IH approach is the best approach for A2-A3 and unruptured small- and medium-size AcomA aneurysm. Posterosuperiorly, directed and recurrent aneurysms requiring wide exposure [[5]],[[6]] may need bifrontal IH approach. However, in our case, we were able to clip this aneurysm from unifrontal IH approach. This was possible because of good CSF release. The limitation of this approach is that it provides less clear proximal control on A1 portion of ACA. The damage to bridging veins is another potential complication of IH approach. It can be minimized by selecting the wider space between two bridging veins as the entry point to the IH fissure. We use dual image video angiography to localize bridging veins before opening the dura. Brain contusion due to retraction is an issue, which can be avoided by applying gentle traction with appropriate subarachnoid dissection and CSF release. A modification of this approach is basal IH approach. In this approach, sinus is ligated and transected at its most anterior part in proximity to crista galli.[[5]] Both olfactory tracts are dissected and both A1 segments of ACA are identified early by subfrontal route.[[5]],[[6]] The IH fissure is then dissected and A2 segment are followed from distal portion toward the AcomA complex. The subfrontal route provides early proximal control of bilateral A1, for which this approach is best for ruptured AcomA. The removal of SAH blood clots from IH fissure to prevent postoperative vasospasm is better in basal IH approach as compared to pterional approach. The limitations of this basal IH approach are open frontal sinus and olfactory tract sacrificing.[[5]] In large series, the authors have described 80% preservation of olfaction by dissecting olfactory tract from the orbital surface of frontal lobe bilaterally as far as the olfactory trigonal region.[[5]],[[6]] By dissecting olfactory tract, traction will not be applied to it, even if the frontal lobe is elevated during surgery. Another modification of IH approach is transcristagalli interfalcine approach. In this approach, basal portion of the falx which is visible after the removal of the crista galli is split into two leaves with a back side of the knife. Venous bleeding from the superior sagittal sinus is controlled by packing with oxidized cellulose and fibrin glue. The advantage of this approach is that both olfactory nerves and bridging veins that lead into the sagittal sinus are protected by the split basal leaves of the falx. This approach provides easy access to the prechiasmatic cistern. If the space is too small for approaching the aneurysm, then one side of falx can be cut to enlarge the operative field as in a unilateral basal IH approach.[[4]]
Conclusion
Unifrontal IH approach is a safe and efficient approach for AcomA aneurysm located deep within the IH fissure, directed posterosuperiorly. Under the surgical microscope with good CSF release, this corridor provides wide exposure and all the flexibility for surgical maneuver. Although early proximal control on A1, venous infarction due to damage of bridging veins is a limitation; on the other hand, it has an added advantage of minimal brain retraction and less risk on olfactory nerve damage. This approach should be the part of the armamentarium of vascular surgeons.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Lehecka M, Dashti R, Hernesniemi J, Niemelä M, Koivisto T, Ronkainen A, et al. Microneurosurgical management of aneurysms at the A2 segment of anterior cerebral artery (proximal pericallosal artery) and its frontobasal branches. Surg Neurol 2008;70:232-46.
- 2 Takaji Y. Fundamental techniques of interhemispheric approach. Jpn J Neurosurg 2015;24:745-50.
- 3 Feletti A, Mamadaliev D, Mewada T, Kei Y, Yamada Y, Kawase T, et al. Interhemispheric approach. Neurovasc Surg eBook, 2019;29-33.
- 4 Sano H, Kato Y, Hayakawa M, Akashi K, Kanno T. A transcrista galli, translamina terminalis approach for highly placed basilar bifurcation aneurysms. Acta Neurochir (Wien) 1997;139:1020-4.
- 5 Suzuki J, Mizoi K, Yoshimoto T. Bifrontal interhemispheric approach to aneurysms of the anterior communicating artery. J Neurosurg 1986;64:183-90.
- 6 Suzuki J, Yoshimoto T, Mizoi K. Preservation of the olfactory tract in bifrontal craniotomy for anterior communicating artery aneurysms, and the functional prognosis. J Neurosurg 1981;54:342-5.
Address for correspondence
Publication History
Article published online:
09 September 2022
© 2019. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Lehecka M, Dashti R, Hernesniemi J, Niemelä M, Koivisto T, Ronkainen A, et al. Microneurosurgical management of aneurysms at the A2 segment of anterior cerebral artery (proximal pericallosal artery) and its frontobasal branches. Surg Neurol 2008;70:232-46.
- 2 Takaji Y. Fundamental techniques of interhemispheric approach. Jpn J Neurosurg 2015;24:745-50.
- 3 Feletti A, Mamadaliev D, Mewada T, Kei Y, Yamada Y, Kawase T, et al. Interhemispheric approach. Neurovasc Surg eBook, 2019;29-33.
- 4 Sano H, Kato Y, Hayakawa M, Akashi K, Kanno T. A transcrista galli, translamina terminalis approach for highly placed basilar bifurcation aneurysms. Acta Neurochir (Wien) 1997;139:1020-4.
- 5 Suzuki J, Mizoi K, Yoshimoto T. Bifrontal interhemispheric approach to aneurysms of the anterior communicating artery. J Neurosurg 1986;64:183-90.
- 6 Suzuki J, Yoshimoto T, Mizoi K. Preservation of the olfactory tract in bifrontal craniotomy for anterior communicating artery aneurysms, and the functional prognosis. J Neurosurg 1981;54:342-5.