

RSS-Feed abonnieren
DOI: 10.4103/ajns.AJNS_57_19
Combined transpedicular-transarticular approach for ventrally located thoracic intradural meningiomas
Autor*innen

Background: The ventrally located intradural meningiomas in the thoracic spine are still considered a challenge for all spine surgeons. Many surgical approaches were developed to excise the lesion without violating the neural structures. They differ in their invasiveness, safety, and efficacy. One of these approaches is the postero-lateral combined transpedicular-transarticular approach (TPA-TAA). Patients and Methods: From January 2016 to December 2018, all patients with ventrally located thoracic meningiomas were operated on using the combined TPA-TAA. We evaluated all the patients preoperatively, immediate postoperative, and 6 months later. Clinical and functional outcomes were assessed using the muscle strength grade and the Nurick grading system. Magnetic resonance imaging was obtained for all patients postoperative and at 6 months later. Results: After 6 months, all patients experienced clinical and functional improvement. The mean muscle strength grade rose from 3.8 preoperatively to 4.8 after 6 months. According to the Nurick grading system, the mean preoperative grade was 4.4 and dropped to 1.8 after 6 months. Minor transient complications such as superficial wound infection and the cerebrospinal fluid leak were observed in 1 patient for each. Gross total tumor excision was achieved in all patients. No cases of tumor recurrence were noted during the follow-up period. Conclusions: This combined TPA-TAA is considered a safe and effective approach in excising ventrally located intradural thoracic meningiomas with minimal postoperative morbidities.
Introduction
Meningiomas and Schwannomas represent the most commonly occurring intradural extramedullary spinal tumors. As Schwannomas arise from the dorsal root, they are located mostly laterally and posteriorly.[[1]],[[2]],[[3]],[[4]],[[5]] However, meningiomas often occur ventral to the spinal cord, whereas they represent a surgical challenge to be totally excised.[[6]] Total excision of the lesion in addition to the involved overlying dura is considered the optimal treatment option in these cases.[[7]],[[8]] Multiple surgical approaches were tailored to achieve this issue. They include extensive laminectomy, modified posterolateral, or transthoracic approaches with variable degrees of bony excisions. Some of these approaches may necessitate additional instrumentation to restore stability.[[5]],[[9]],[[10]],[[11]]
One of the approaches that offer good and safe surgical access to the ventral and lateral compartment of the thoracic spinal canal is the combined transpedicular-transarticular approach (TPA-TAA).[[6]] In this study, we evaluate the results of the TPA-TAA in excision of ventrally located intradural thoracic meningioma.
Patients and Methods
Between January 2016 and December 2018, nine patients underwent surgical resection of ventrally located intradural thoracic meningioma. The tumor level was T8-T9 in two cases, T5-T6 in two cases, T5, T7, T7-T8, T9, and T10 in each of the other cases. Gross total removal was planned for all patients. Preoperative clinical examination was carefully done, and muscle strength of the lower limbs for each patient was carefully measured according to the motor power grading system from 0 to 5. Furthermore, each patient was assigned to a clinical grade according to the Nurick functional grading system [[12]] [[Table 1]]. Neurological evaluation was performed during the immediate postoperative period and 6 months later. No mortality has been reported.

Clinical summary
The patient series consisted of six females and three males with a male:female ratio of 1:3. Age ranged from 46 to 62 years (mean 53.4 years) at the time of presentation. Duration of the complaint ranged from 3 to 24 months (mean 13.7 months). Interscapular pain was a common complaint in seven patients; four patients had associated pain radiating to the lower back. Five patients noted a sensory complaint such as numbness, paresthesia, or dysesthesia below the level of the lesion. Lower limbs heaviness was the presenting complaint in all patients. All patients experienced a slowly progressive course of the complaint. On the initial clinical examination, lower limb weakness – to various degrees – was present in all patients.
Radiological investigation
All patients were investigated using magnetic resonance imaging (MRI), which revealed an intradural extramedullary space occupying lesion with a predominantly ventral location to the thoracic spinal cord. Five lesions showed most of the tumor bulk on the right side, whereas the other four on the left side. All lesions showed homogeneous gadolinium enhancement [[Figure 1]].

Surgical technique
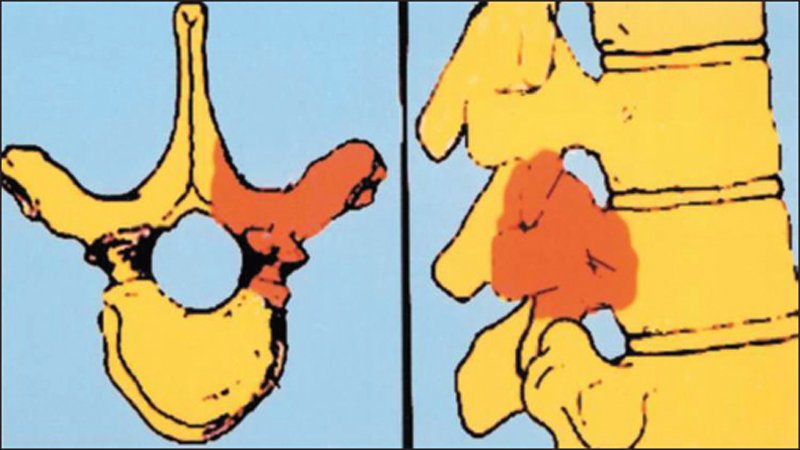
Informed consent was obtained from each patient. The approach was made from the side with more lesion bulk found on the preoperative MRI scan. We operated all patients in the prone position. After induction of general anesthesia and proper positioning of the patient, anteroposterior and lateral fluoroscopic images were obtained to verify the target level. A midline vertical skin incision was centered over the desired level, followed by paraspinal muscle dissection from the spinous process to expose the laminae of the vertebrae above and below the target level on the affected side. Dissection was continued laterally to expose the articulation and transverse process. Exposure was then started by accomplishing hemilaminectomy on the affected side followed by drilling of the facet joint, the pedicle, the articular complex, and the transverse process using a high-speed drill. Neither rib portions nor vertebral body were removed [[Figure 2]]. This created a posterolateral corridor exposing the lateral aspect of the thecal sac, where the dura was incised in a linear manner and stitched to the sides.
Under the magnification of the surgical microscope, we started careful cauterization and excision of the lesion with cauterization of the underlying dura. After ensuring gross total excision and decompression of the cord, watertight dural closure was done, followed by fascial and skin closure in layers. A dorso-lumbar brace was applied for 6 weeks postoperatively.
Results
All tumors were gross radically excised and histologically verified. No operative-related mortality was recorded. On immediate postoperative evaluation, motor power in the lower limbs remained unchanged in five patients. No patients had experienced postoperative neurological deterioration. Pathological examination revealed meningioma in all cases.
We followed the patients for 6 months after surgery. All patients showed clinical improvement at the end of follow-up period.
The preoperative muscle strength grade for all patients ranged from 1 to 4 with a mean of 3.3. At the immediate postoperative examination, the mean muscle strength grade improved to 3.8 (range 2–5). At the end of the follow-up period, improvement in the mean muscle strength grade reached 4.8 (range 4–5). According to the Nurick grading system, functional recovery was observed in all patients. The mean preoperative grade was 4.4 (range 4–5) which dropped at the end of follow-up period to 1.8 (range 0–4). There was one case of transient postoperative cerebrospinal fluid (CSF) leak, which recovered in few days with repeated lumber CSF drainages. There was a case of transient superficial wound infection which was relieved using daily wound dressing with the topical antibiotic application. Two cases of the postoperative intercostal neuralgia were observed and controlled using pain medications.
Immediate postoperative and at 6 months MRI scans were performed in all patients without any evidence of recurrence at this time [[Figure 3]]. There is no evidence of instability, either clinically or radiologically. There have been no mortalities.

Discussion
Surgery for ventrally located meningiomas in the thoracic spine is still considered of special interest due to the anatomical characteristics of the surgical field. The spinal canal is relatively narrow and is mostly occupied by the spinal cord. The corridor to the lesion is obstructed by the mediastinum and pleural cavity ventrally, spinal cord dorsally, and the thoracic cage and musculature laterally.[[5]],[[13]],[[14]],[[15]] Intraoperatively, it is crucial to try to preserve the segmental radicular artery, especially the artery of Adamkiewicz.[[5]],[[14]]
Different approaches were designed to achieve successful excision of such ventral lesions with the least possible undesirable side effects.
Regarding the usual posterior approach through the midline laminectomy, it necessitates division of the dentate ligament and various degree of spinal cord manipulation, which results usually in undesirable sequelae. As the cord is located in-between the lesion and the surgeon, this results also in incomplete surgical excision of the lesion.[[1]],[[2]],[[5]],[[15]],[[16]]
Regarding the anterior approaches, such as the trans-thoracic or the trans-sternal approaches, they offer the maximum exposure and decompression of the ventral part of the spinal canal. On the other hand, they have a lot of disadvantages resulting in extensive surgical maneuvers that are associated with high risk of side effects such as pulmonary complications or CSF pleural fistulas. They also expose the spinal cord to the risk of injury as the lesion is located in-between the cord and the surgeon.[[13]],[[15]]
The lateral approaches such as the costotransversectomy and the lateral extracavitary with their modifications have been utilized in thoracic spine lesions. They allow good exposure of the lateral and ventral compartment of the spinal canal. On the other hand, they have a lot of disadvantages such as being more invasive, high risk of pleural injury, increased incidence of postoperative spinal instability, and the risk of injury to the neurovascular bundle including the radicular artery of Adamkiewicz.[[5]],[[17]],[[18]]
The postero-lateral approaches include the TPA which was originally described by Patterson and Arbit for thoracic disc herniation,[[19]] and the TAA which was described by Richaud et al. in the treatment of posttraumatic canal stenosis.[[20]],[[21]]
They have a lot of advantages such as being less invasive than the anterior and lateral approaches, avoiding the risk of rib resection and ligature of the neurovascular bundle, and avoiding the need of spinal cord retraction or manipulation. The main disadvantage of these approaches is the limited capability to expose and excise ventrally located intradural spinal lesions.[[6]]
We have found that the combined TPA and TAA approaches might overcome the aforementioned disadvantages. The removal of the hemilamina, pedicle, articular complex, and the transverse process offers a good exposure of the central ventral spinal canal. This allows simultaneous exposure of the cord and the meningioma, without manipulation or traction of the spinal cord.
The cornerstone in this approach is the creation of a corridor that provides enough room to excise the lesion completely and to preserve neurological function. This is accomplished by adequate drilling of the facet joint, the entire pedicle flush with the vertebral body, the hemilamina, and transverse process.
We reported no cases of postoperative instability. This is because of the maintenance of the structural integrity of the ribs and the intervertebral discs which eliminate the need for spinal instrumentation. It also carries no risk of injury to the radicular artery of Adamkiewicz as it is not necessary to disrupt the content of the intervertebral foramina.
We reported no cases of tumor recurrence as this approach allows radical excision of the tumor. Incomplete removal of the spinal meningioma predisposes to tumor recurrence as reported widely in the literature.[[2]],[[4]],[[22]],[[23]],[[24]]
Conclusions
The combined (TPA-TAA) approach offers a safe and wide exposure of the lateral and ventral aspect of the spinal canal. This allows safe and complete removal of the ventrally located intradural spina meningioma in the region of the thoracic spin. It eliminates the need for cord retraction and manipulation. There is no need for spinal instrumentation. It is also could be achieved with little blood loss, and without the need for chest tube that is required in trans-thoracic approaches. It is considered a less invasive alternative, especially in elderly patients, with associated comorbidities.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Gezen F, Kahraman S, Canakci Z, Bedük A. Review of 36 cases of spinal cord meningioma. Spine (Phila Pa 1976) 2000;25:727-31.
- 2 Klekamp J, Samii M. Surgical results for spinal meningiomas. Surg Neurol 1999;52:552-62.
- 3 Sandalcioglu IE, Hunold A, Müller O, Bassiouni H, Stolke D, Asgari S. Spinal meningiomas: Critical review of 131 surgically treated patients. Eur Spine J 2008;17:1035-41.
- 4 Solero CL, Fornari M, Giombini S, Lasio G, Oliveri G, Cimino C, et al. Spinal meningiomas: Review of 174 operated cases. Neurosurgery 1989;25:153-60.
- 5 Steck JC, Dietze DD, Fessler RG. Posterolateral approach to intradural extramedullary thoracic tumors. J Neurosurg 1994;81:202-5.
- 6 Gambardella G, Gervasio O, Zaccone C. Approaches and surgical results in the treatment of ventral thoracic meningiomas. Review of our experience with a postero-lateral combined transpedicular-transarticular approach. Acta Neurochir (Wien) 2003;145:385-92.
- 7 Levy WJ, Latchaw J, Hahn JF, Sawhny B, Bay J, Dohn DF. Spinal neurofibromas: A report of 66 cases and a comparison with meningiomas. Neurosurgery 1986;18:331-4.
- 8 Peker S, Cerçi A, Ozgen S, Isik N, Kalelioglu M, Pamir MN. Spinal meningiomas: Evaluation of 41 patients. J Neurosurg Sci 2005;49:7-11.
- 9 Kawahara N, Tomita K, Abdel-Wanis ME, Fujita T, Murakami H, Demura S. Recapping T-saw laminocostotransversoplasty for ventral meningiomas in the thoracic region. J Orthop Sci 2009;14:548-55.
- 10 Yamahata H, Yamaguchi S, Mori M, Kubo F, Tokimura H, Arita K. Ventral schwannoma of the thoracolumbar spine. Asian Spine J 2013;7:339-44.
- 11 Lesoin F, Rousseaux M, Lozes G, Villette L, Clarisse J, Pruvo JP, et al. Posterolateral approach to tumours of the dorsolumbar spine. Acta Neurochir (Wien) 1986;81:40-4.
- 12 Nurick S. The pathogenesis of the spinal cord disorder associated with cervical spondylosis. Brain 1972;95:87-100.
- 13 Bennett GJ. Surgical approaches to the thoracic spine. Clin Neurosurg 1992;38:234-51.
- 14 Stillerman CB, Weiss MH. Management of thoracic disc disease. Clin Neurosurg 1992;38:325-52.
- 15 Stillerman CB, Chen TC, Couldwell WT, Zhang W, Weiss MH. Experience in the surgical management of 82 symptomatic herniated thoracic discs and review of the literature. J Neurosurg 1998;88:623-33.
- 16 Jho HD. Endoscopic microscopic transpedicular thoracic discectomy. Technical note. J Neurosurg 1997;87:125-9.
- 17 Fessler RG, Dietze DD Jr., Millan MM, Peace D. Lateral parascapular extrapleural approach to the upper thoracic spine. J Neurosurg 1991;75:349-55.
- 18 Maiman DJ, Larson SJ, Luck E, El-Ghatit A. Lateral extracavitary approach to the spine for thoracic disc herniation: Report of 23 cases. Neurosurgery 1984;14:178-82.
- 19 Patterson RH Jr., Arbit E. A surgical approach through the pedicle to protruded thoracic discs. J Neurosurg 1978;48:768-72.
- 20 Richaud J, Boetto S, Lazorthes Y. Posterolateral approach and anterior spinal canal recalibration in severe spinal injury affecting T-12, L-1: A study of seven cases. Neurosurgery 1986;19:218-27.
- 21 Richaud J, Bousquet P, Ealet G, Clamens J, Beltchika K, Lazorthes Y. Recalibration via a postero-lateral approach in recent traumatic stenosis of the dorsal and lumbar spine. Modalities and results apropos of 31 cases. Neurochirurgie 1990;36:27-38.
- 22 Roux FX, Nataf F, Pinaudeau M, Borne G, Devaux B, Meder JF. Intraspinal meningiomas: Review of 54 cases with discussion of poor prognosis factors and modern therapeutic management. Surg Neurol 1996;46:458-63.
- 23 Kim CH, Chung CK. Surgical outcome of a posterior approach for large ventral intradural extramedullary spinal cord tumors. Spine (Phila Pa 1976) 2011;36:E531-7.
- 24 Yoon SH, Chung CK, Jahng TA. Surgical outcome of spinal canal meningiomas. J Korean Neurosurg Soc 2007;42:300-4.
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
09. September 2022
© 2019. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Gezen F, Kahraman S, Canakci Z, Bedük A. Review of 36 cases of spinal cord meningioma. Spine (Phila Pa 1976) 2000;25:727-31.
- 2 Klekamp J, Samii M. Surgical results for spinal meningiomas. Surg Neurol 1999;52:552-62.
- 3 Sandalcioglu IE, Hunold A, Müller O, Bassiouni H, Stolke D, Asgari S. Spinal meningiomas: Critical review of 131 surgically treated patients. Eur Spine J 2008;17:1035-41.
- 4 Solero CL, Fornari M, Giombini S, Lasio G, Oliveri G, Cimino C, et al. Spinal meningiomas: Review of 174 operated cases. Neurosurgery 1989;25:153-60.
- 5 Steck JC, Dietze DD, Fessler RG. Posterolateral approach to intradural extramedullary thoracic tumors. J Neurosurg 1994;81:202-5.
- 6 Gambardella G, Gervasio O, Zaccone C. Approaches and surgical results in the treatment of ventral thoracic meningiomas. Review of our experience with a postero-lateral combined transpedicular-transarticular approach. Acta Neurochir (Wien) 2003;145:385-92.
- 7 Levy WJ, Latchaw J, Hahn JF, Sawhny B, Bay J, Dohn DF. Spinal neurofibromas: A report of 66 cases and a comparison with meningiomas. Neurosurgery 1986;18:331-4.
- 8 Peker S, Cerçi A, Ozgen S, Isik N, Kalelioglu M, Pamir MN. Spinal meningiomas: Evaluation of 41 patients. J Neurosurg Sci 2005;49:7-11.
- 9 Kawahara N, Tomita K, Abdel-Wanis ME, Fujita T, Murakami H, Demura S. Recapping T-saw laminocostotransversoplasty for ventral meningiomas in the thoracic region. J Orthop Sci 2009;14:548-55.
- 10 Yamahata H, Yamaguchi S, Mori M, Kubo F, Tokimura H, Arita K. Ventral schwannoma of the thoracolumbar spine. Asian Spine J 2013;7:339-44.
- 11 Lesoin F, Rousseaux M, Lozes G, Villette L, Clarisse J, Pruvo JP, et al. Posterolateral approach to tumours of the dorsolumbar spine. Acta Neurochir (Wien) 1986;81:40-4.
- 12 Nurick S. The pathogenesis of the spinal cord disorder associated with cervical spondylosis. Brain 1972;95:87-100.
- 13 Bennett GJ. Surgical approaches to the thoracic spine. Clin Neurosurg 1992;38:234-51.
- 14 Stillerman CB, Weiss MH. Management of thoracic disc disease. Clin Neurosurg 1992;38:325-52.
- 15 Stillerman CB, Chen TC, Couldwell WT, Zhang W, Weiss MH. Experience in the surgical management of 82 symptomatic herniated thoracic discs and review of the literature. J Neurosurg 1998;88:623-33.
- 16 Jho HD. Endoscopic microscopic transpedicular thoracic discectomy. Technical note. J Neurosurg 1997;87:125-9.
- 17 Fessler RG, Dietze DD Jr., Millan MM, Peace D. Lateral parascapular extrapleural approach to the upper thoracic spine. J Neurosurg 1991;75:349-55.
- 18 Maiman DJ, Larson SJ, Luck E, El-Ghatit A. Lateral extracavitary approach to the spine for thoracic disc herniation: Report of 23 cases. Neurosurgery 1984;14:178-82.
- 19 Patterson RH Jr., Arbit E. A surgical approach through the pedicle to protruded thoracic discs. J Neurosurg 1978;48:768-72.
- 20 Richaud J, Boetto S, Lazorthes Y. Posterolateral approach and anterior spinal canal recalibration in severe spinal injury affecting T-12, L-1: A study of seven cases. Neurosurgery 1986;19:218-27.
- 21 Richaud J, Bousquet P, Ealet G, Clamens J, Beltchika K, Lazorthes Y. Recalibration via a postero-lateral approach in recent traumatic stenosis of the dorsal and lumbar spine. Modalities and results apropos of 31 cases. Neurochirurgie 1990;36:27-38.
- 22 Roux FX, Nataf F, Pinaudeau M, Borne G, Devaux B, Meder JF. Intraspinal meningiomas: Review of 54 cases with discussion of poor prognosis factors and modern therapeutic management. Surg Neurol 1996;46:458-63.
- 23 Kim CH, Chung CK. Surgical outcome of a posterior approach for large ventral intradural extramedullary spinal cord tumors. Spine (Phila Pa 1976) 2011;36:E531-7.
- 24 Yoon SH, Chung CK, Jahng TA. Surgical outcome of spinal canal meningiomas. J Korean Neurosurg Soc 2007;42:300-4.