
RSS-Feed abonnieren
DOI: 10.4103/ijmbs.ijmbs_45_19
Retropharyngeal soft-tissue mass with multiple cranial neuropathies

Retropharyngeal lesions have different spectrum of presentations. We herein present a case with step-wise progression of ambiguous symptoms and signs of polycraniopathy, caused by a soft-tissue mass in the retropharyngeal space extending into the cavernous sinus, as detected by magnetic resonance imaging. Initially, he was presented with hemifacial pain and lately progress rapidly to involve all cranial nerves; 3rd through 12th cranial nerves. The differential diagnosis was malignant tumor or aggressive infectious mass, which were excluded by histopathological examination. The diagnosis of inflammatory pseudotumor was a diagnosis of exclusion and decided based on a combination of clinical profile, blood test, radiological, and histopathological results.
#
Introduction
Soft-tissue masses, other than malignant masses, of the head and neck rarely present with invasion of the base of the skull.[[1]] Inflammatory pseudotumor should be considered, while dealing with soft-tissue mass in the retropharyngeal area as it may mimic malignant neoplasm. Previous report showed four cases of nasopharyngeal inflammatory pseudotumor with skull base invasion in diabetic patients.[[2]]
We describe a case of soft-tissue mass infiltrating the nasopharynx and extending up to the cavernous sinus. Knowledge about diversity of such case increases the awareness of neurologists, otolaryngologists, and radiologists and help in directing the appropriate management protocol.
#
Case Report
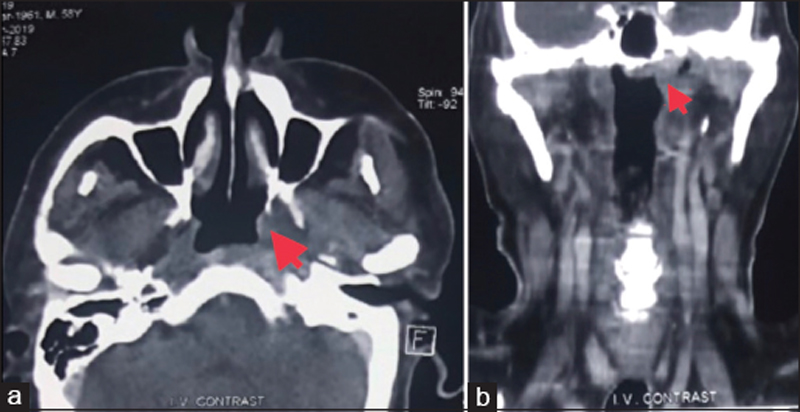
A 57-year-old male, diabetic, presents with a 2 months history of left-sided facial pain involving the temporal, periorbital, preauricular, and mandibular area. He also had pain during chewing. He was treated by otolaryngologist with carbamazepine on assumptive diagnosis of trigeminal neuralgia. There was a minimal improvement of the pain. Magnetic resonance image (MRI) of the cerebellopontine angle reveals no structural lesion. As his symptoms persist, despite adequate analgesia, the patient referred to the neurology clinic and then admitted to neurology unit of our hospital. Neurologic examination on day of admission, revealed mild proptosis of the left eye with full range of movement of extraocular muscles, hyperesthesia in the distribution of the three divisions of left trigeminal nerve, with maximal intensity at the left frontal and temporal areas, other cranial nerves were normal, and the motor system is of normal tone and power. Otherwise, the patient was in severe pain and irritable. He has anemia and markedly elevated inflammatory markers (erythrocyte sedimentation rate and C-reactive protein). Other laboratory data including antinuclear antibody are within normal. Chest radiograph and ultrasound scan of the neck were unrevealing. MRI of the brain and cavernous sinus was ordered. The patient decided to perform the brain image as outpatient and come back on follow-up. In 2 weeks, he develops severe bulbar palsy with drooling of saliva and chocking. He has marked proptosis with limitation of left lateral gaze and diplopia [[Figure 1]], left lower motor neuron facial palsy, and left hypoglossal nerve palsy [[Figure 2]]. The MRI of the brain shows evidence of small left-sided retropharyngeal-infiltrating soft-tissue mass with apparent perineural extension to the left foramen ovale and sparing of the left Meckel's cave [[Figure 3]] single arrow] with invasion of the left cavernous sinus from its inferior aspect [[Figure 3]] double arrows]. High-dose steroid therapy (Dexamethasone 12 mg/day) was initiated. Computed tomography of the neck and base of skull [[Figure 4]]a and [[Figure 4]]b was performed which shows asymmetry of the nasopharynx. The differential diagnosis included nasopharyngeal carcinoma, lymphoma, sarcoidosis, tuberculosis, and other aggressive infectious diseases. He has no history of fever throughout his illness. Examination by otolaryngologist revealed normal oropharynx and intact mucosal lining of nasopharynx and Rosenmüller fossa, the soft-tissue mass was evident through nasopharynx, and biopsy was undertaken. The histopathology shows severe inflammatory reaction with extensive fibrosis, with no evidence of malignancy. According to the histopathology results, we assume that this is a case of inflammatory pseudotumor of the retropharynx infiltrating base of skull and extending to the cavernous sinus. The treatment continued with parenteral steroid in addition to broad-spectrum antibiotics and low-molecular-weight heparin. There was substantial improvement at the initial course. After 2 weeks, the symptoms reappear, with marked chocking and dyspnea. He developed aspiration pneumonia and eventually died.



#
Discussion
We herein report a rare case of retropharyngeal mass invading the base of skull and steadily engulfing the cranial nerves from 3rd to 12th. The ambiguous presentation as hemifacial pain directed the management toward relieving of the neuropathic pain, as there was no obvious pathology seen initially, making the diagnosis enigmatic and confusing clinically. There have been some published cases with inhomogeneous symptoms of the diseases of retropharyngeal space which includes single or multiple cranial nerve neuropathy and pain.[[3]],[[4]] Indiscriminate diagnosis of inflammatory pseudotumor of the retropharyngeal space was applied to our case. The diagnosis of inflammatory pseudotumor was considered likely on the basis of patient clinical profile and results of the available tests.
In the head and neck, inflammatory pseudotumor most commonly involves the orbit.[[5]] Although rare, there are some reports of extraorbital involvement which includes the maxillary sinus, nasopharynx (including parapharyngeal space), and the major salivary glands.[[6]],[[7]],[[8]] Involvement of nasopharynx with extension to cavernous sinus has also been reported.[[9]]
In our case, it was very difficult to decide clinically as well as radiologically about an infiltrating soft-tissue mass whether it is a malignant neoplasm or severe infection. However, severe extensive involvement of the lower cranial nerves with sparing of the bony structures of the base of skull makes the possibility of malignant neoplasm unlikely. Furthermore, examination through nasopharynx showed normal mucosal lining of the nasopharynx with sparing of Rosenmüller fossa. In addition, there were no signs or symptoms of infectious process such as fever. Biopsy from the mass showed only chronic inflammatory cells with severe fibrosis, no malignant cells, and there was no evidence of caseating or noncaseating granulomas. Based on these findings and on reviewing previous reports, the diagnosis of inflammatory pseudotumor was considered. The patient was treated with high-dose corticosteroid therapy together with broad-spectrum antibiotics and low-molecular-weight heparin. Although the patient showed dramatic improvement in the 1st week, he subsequently deteriorated, developed aspiration pneumonia with severe respiratory distress, and eventually died. The cause of death in our case is not attributed to the nature of the lesion, but likely to the development of serious complications of respiratory distress in the absence of assisted mechanical ventilation. In previous reports, the follow-up of such cases shows good outcome.[[10]]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient's guardian has given his consent for his child's images and other clinical information to be reported in the journal. The patient's guardian understands that his child's name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
#
Authors' contributions
All authors contributed to the care of the patient, drafting of the case report, revision, and approval of its final version.
#
Compliance with ethical principles
No prior ethical approval is usually required for single case reports. However, the parents of the patient provided consent for publication as stated above.
Reviewers:
Mohamed El-Fikki (Alexandria, Egypt)
Enver Ozer (Columbus OH, USA)
Editors:
Elmahdi A Elkhammas (Columbus OH, USA)
#
#
#
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Garg V, Temin N, Hildenbrand P, Silverman M, Catalano PJ. Inflammatory pseudotumor of the skull base. Otolaryngol Head Neck Surg 2010;142:129-31.
- 2 Chwang WB, Jain R, Narayan A, McHugh J, Ghanem T, Seidman M, et al. Inflammatory pseudotumor of the nasopharynx and skull base: Mimicking an aggressive neoplasm or infection. Arch Otolaryngol Head Neck Surg 2012;138:765-9.
- 3 Gadde J, Franck B, Liu X, Teixido M, Rizk H. Inflammatory pseudotumor of the nasopharynx with spread along the trigeminal nerve. Am J Otolaryngol 2013;34:252-4.
- 4 Olmos PR, Falko JM, Rea GL, Boesel CP, Chakeres DW, McGhee DB. Fibrosing pseudotumor of the sella and parasellar area producing hypopituitarism and multiple cranial nerve palsies. Neurosurgery 1993;32:1015-21.
- 5 Kansara S, Bell D, Johnson J, Zafereo M. Head and neck inflammatory pseudotumor: Case series and review of the literature. Neuroradiol J 2016;29:440-6.
- 6 Maldjian JA, Norton KI, Groisman GM, Som PM. Inflammatory pseudotumor of the maxillary sinus in a 15-year-old boy. AJNR Am J Neuroradiol 1994;15:784-6.
- 7 Nakayama K, Inoue Y, Aiba T, Kono K, Wakasa K, Yamada R. Unusual CT and MR findings of inflammatory pseudotumor in the parapharyngeal space: Case report. AJNR Am J Neuroradiol 2001;22:1394-7.
- 8 Williams SB, Foss RD, Ellis GL. Inflammatory pseudotumors of the major salivary glands. Clinicopathologic and immunohistochemical analysis of six cases. Am J Surg Pathol 1992;16:896-902.
- 9 McCall T, Fassett DR, Lyons G, Couldwell WT. Inflammatory pseudotumor of the cavernous sinus and skull base. Neurosurg Rev 2006;29:194-200.
- 10 Swamy BN, McCluskey P, Nemet A, Crouch R, Martin P, Benger R, et al. Idiopathic orbital inflammatory syndrome: Clinical features and treatment outcomes. Br J Ophthalmol 2007;91:1667-70.
Corresponding author
Publikationsverlauf
Eingereicht: 27. August 2019
Angenommen: 22. Oktober 2019
Artikel online veröffentlicht:
07. Juli 2022
© 2019. The Libyan Authority of Scientific Research and Technologyand the Libyan Biotechnology Research Center. All rights reserved. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License,permitting copying and reproductionso long as the original work is given appropriate credit. Contents may not be used for commercial purposes, oradapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Garg V, Temin N, Hildenbrand P, Silverman M, Catalano PJ. Inflammatory pseudotumor of the skull base. Otolaryngol Head Neck Surg 2010;142:129-31.
- 2 Chwang WB, Jain R, Narayan A, McHugh J, Ghanem T, Seidman M, et al. Inflammatory pseudotumor of the nasopharynx and skull base: Mimicking an aggressive neoplasm or infection. Arch Otolaryngol Head Neck Surg 2012;138:765-9.
- 3 Gadde J, Franck B, Liu X, Teixido M, Rizk H. Inflammatory pseudotumor of the nasopharynx with spread along the trigeminal nerve. Am J Otolaryngol 2013;34:252-4.
- 4 Olmos PR, Falko JM, Rea GL, Boesel CP, Chakeres DW, McGhee DB. Fibrosing pseudotumor of the sella and parasellar area producing hypopituitarism and multiple cranial nerve palsies. Neurosurgery 1993;32:1015-21.
- 5 Kansara S, Bell D, Johnson J, Zafereo M. Head and neck inflammatory pseudotumor: Case series and review of the literature. Neuroradiol J 2016;29:440-6.
- 6 Maldjian JA, Norton KI, Groisman GM, Som PM. Inflammatory pseudotumor of the maxillary sinus in a 15-year-old boy. AJNR Am J Neuroradiol 1994;15:784-6.
- 7 Nakayama K, Inoue Y, Aiba T, Kono K, Wakasa K, Yamada R. Unusual CT and MR findings of inflammatory pseudotumor in the parapharyngeal space: Case report. AJNR Am J Neuroradiol 2001;22:1394-7.
- 8 Williams SB, Foss RD, Ellis GL. Inflammatory pseudotumors of the major salivary glands. Clinicopathologic and immunohistochemical analysis of six cases. Am J Surg Pathol 1992;16:896-902.
- 9 McCall T, Fassett DR, Lyons G, Couldwell WT. Inflammatory pseudotumor of the cavernous sinus and skull base. Neurosurg Rev 2006;29:194-200.
- 10 Swamy BN, McCluskey P, Nemet A, Crouch R, Martin P, Benger R, et al. Idiopathic orbital inflammatory syndrome: Clinical features and treatment outcomes. Br J Ophthalmol 2007;91:1667-70.