

Subscribe to RSS
DOI: 10.4103/jdep.jdep_6_19
Secondary Oral Anti-hyperglycemic Drugs Failure in Type 2 Diabetes Patients Infected with Hepatitis C Virus
Authors

Background and Objective: Chronic hepatitis C infection can affect glycemic control in patients with diabetes mellitus (DM). This study was done to assess the influence of hepatitis C viral infection compared to hepatitis B viral infection and noninfected cases on the occurrence of secondary oral anti-hyperglycemic drugs (OADs) failure in type 2 diabetes mellitus (T2DM) patients. Patients and Methods: This prospective study was conducted on 1293 T2DM patients who had their hepatitis B and C status checked by the enzyme-linked immunosorbent assay method. Glycemic management was done according to the standard guidelines, and glycemic control was reviewed after 6 months of enrollment. Patients who had hemoglobin HbA1c >7.5% in spite of taking >75% of the maximum dosage of three OADs, that is, metformin, sulfonylurea, and thiazolidinediones were selected. Those who were already taking insulin therapy regardless of HbA1c were also considered as secondary OADs failure. The status of secondary OADs failure was analyzed in three groups: hepatitis C virus (HCV) positive, hepatitis B virus (HBV) positive, or noninfected patients. Results: Of selected 1293 cohorts, DM with HCV positive was 152 (11.7%), and DM with HBV positive was 111 (8.5%). Among 152 HCV-positive patients, secondary OADs failure was detected in 64 (42.1%), and in those with 111 HBV-positive patients, it was detected in 30 patients (27.02%), whereas it was 177 of 1030 noninfected patients (17.1%). Conclusion: Hepatitis C infection is more common than hepatitis B infection among diabetes patients. Secondary OADs failure is significantly associated with HCV-infected diabetes patients compared to other groups, and timely consideration of insulin initiation is important in these cases.
Introduction
In Myanmar, diabetes is common and affects approximately HbA1c 10.5% of the adult population.[[1]] The seroprevalence rate of hepatitis C in the general population is 2.7%[[2]] and 20% in diabetes.[[3]] The effect of hepatitis C on hyperglycemia is still unclear. Increased insulin resistance plays an important role.[[4]] A significant beta-cell dysfunction has also been proposed.[[5]]. Type 2 diabetes mellitus (T2DM) is characterized by a progressive decline of beta-cell function leading to secondary oral anti-hyperglycemic drugs (OADs) failure.[[6]] This study was aimed to evaluate the association of secondary OADs failure in hepatitis C virus (HCV)-infected (T2DM).
Patients and Methods
This was a prospective study to measure the secondary OADs failure in T2DM patients who have viral hepatitis C infection compared to hepatitis B and noninfection in type 2 diabetes patients. Participants were recruited from two diabetes outpatient clinics from August 2009 to March 2012. A total of 1303 type 2 diabetes patients had been tested for hepatitis B and C virus. Their hepatitis B and C status were checked by the enzyme-linked immunosorbent assay method.
In this study, patients with secondary OADs failure were operationally defined as those of any age who had hemoglobin HbA1c >7.5% in spite of having more than >75% of maximum dosages of three OADs, that is, metformin, sulfonylurea, and thiazolidinediones. Those who had already taking insulin therapy due to OADs failure were also selected irrespective of the current HbA1c. Those with type 1 diabetes, gestational diabetes, end-stage kidney disease, advanced cirrhosis of the liver and acute, or other comorbidities such as tuberculosis were excluded. Patients who were positive for both hepatitis B virus (HBV) and HCV coinfection (n = 10) were also excluded. All the participants involved in this study have given written informed consent.
After obtaining written informed consent, patients were interviewed according to the pro forma. A series of questionnaire included demographic characteristics such as age, sex, duration of diabetes, and body mass index were recorded. Risk factors for hepatitis infection such as history of blood transfusion, previous use of nondisposable syringe, tattooing, family history of diabetes mellitus, and viral hepatitis B and C infection; details about diabetes including medical therapy were asked. Glycemic management was done according to the standard guidelines with a personalized approach, and each patient was reviewed at 6 months after the enrollment.
Their status of secondary OADs failure was analyzed in three groups: HCV positive, HBV positive, and noninfected patients. [[Figure 1]] shows the flow of the study design.

Statistical analysis
Data collection was checked for completeness, errors, and inconsistencies.
Data coding and analysis were carried out using SPSS (Statistical Package for the Social Sciences version 16.0, IBM Crop., NewYork, USA) Categorical variables were analyzed with Chi-square test or Fisher's exact test, and ANOVA as appropriate. The significant level (α = 0.05) was used for all the statistical analyses (95% confidence interval [CI]).
Results
The study included 1293 participants, including 152 HCV, 111 HBV, and 1030 noninfected patients with diabetes. Following the 6-month period of standard and individualized treatment, glycemic status was reassessed.
[[Table 1]] presents the baseline demographic and clinical characteristics of those with secondary OADs failure in respective groups. The mean age of patients with HCV-positive group was younger than HBV-positive group with OADs failure. There were no significant differences in gender and body mass index among these three groups.

Comparing to other groups, those with HCV-positive group were found out to be the shortest duration of diabetes. No significant difference was found regarding microvascular complications among three groups [[Table 2]].

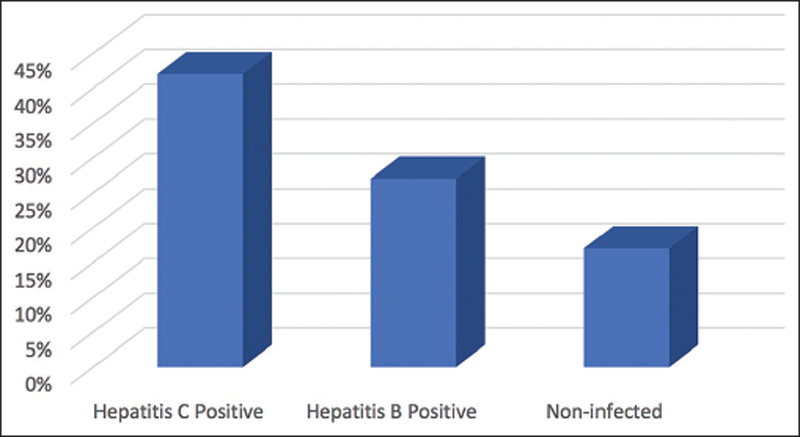
Regarding the occurrence of secondary OADs failure, 64 out of 152 HCV-positive patients (42.1%), 30 out of 111 HBV-positive patients (27.02%), and 177 out of 1030 noninfected diabetes patients (17.1%) were detected (P < 0.001) [[Figure 2]].
Discussion
In this study, out of 1293 type-2 diabetes patients, there were 152 hepatitis C patients (11.7%) and 111 hepatitis B patients (8.5%). In the Myanmar population, HCV infection is 2.7% and HBV infection is 6.5%, respectively.[[7]] The current study indicates that HCV infection is more than HBV infection in type 2 diabetes. The similar findings were also shown by the two meta-analysis studies (odds ratio [OR] =1.63; 95% CI: 1.11–2.39 in White et al. and OR = 1.92; 95% CI: 1.41–2.62 in Naing et al. studies).[[8]],[[9]]
In Lecube et al.'s study, the prevalence of HCV antibodies in T2DM patients was in the range between 1.78% and 12.1% worldwide.[[10]] According to Ni et al.'s study in Myanmar, HCV infection was detected in around one-fifth of diabetic patients.[[3]] On the other hand, it was also noted that the prevalence of diabetes is around two- to three-fold increase in patients with HCV than in those with HBV[[4]],[[11]],[[12]],[[13]],[[14]],[[15]],[[16]],[[17]],[[18]] and this was first reported by Allison et al. in 1994.[[19]]
There have been few clinical studies regarding the effect of hepatitis C on secondary OADs failure in real clinical practice. It was clearly shown in this study that hepatitis C has a significant effect on glycemic control. The secondary OADs failure in hepatitis C-positive group occurred at a younger age and shorter duration of diabetes than those with hepatitis B-positive groups. This could be attributed to both factors of insulin resistance as well as beta-cell dysfunction in hepatitis C infection. The insulin requirements were not compared among these groups in this study. However, a higher requirement of insulin therapy was reported by Allison et al. in 1994[[19]] and Gulcan et al.[[20]] in Turkey, in 2008.
Conclusion
This study has emphasized the presence of hepatitis C in type 2 diabetes as a cause of poor glycemic control. It is mandatory to do screening for HCV infection in all type 2 diabetes patients who are living in area of high prevalence. This study provides the knowledge of early secondary OADs failure in hepatitis C-positive diabetes patients and encourages the clinicians for pre-emptive timely initiation and intensification of insulin therapy to achieve optimal glycemic control.
Limitations of the study
There are some limitations in the present study. First, this study was done before the availability of new OADs medications in Myanmar, we had operationally defined and calculated the maximum tolerable dosage on three medications: metformin, sulfonylurea, and pioglitazone. Second, this study did not measure the genotype of HCV infection and viral load for each and every case. Finally, this study did not include those who had received antiviral therapy (ribavirin and interferon) or not. We did not assess the degree of hepatic steatosis and fibrosis which itself could be the contributing factor for insulin resistance.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Self.
-
References
- 1 Latt TS, KK, Aye TT, Ko K. Report on National Survey of Diabetes Mellitus and Risk Factors for Non communicable Diseases in Myanmar in 2014. Myanmar: Ministry of Health; 2014.
- 2 World Health Organization | World Hepatitis Day 2017: Eliminate Hepatitis. World Health Organization; 2017.
- 3 Ni H, Moe S, Htet A. Hepatitis C virus infection in diabetes mellitus patients. Int J Collab Res Intern Med Public Health 2012;5:599-606.
- 4 Hammerstad SS, Grock SF, Lee HJ, Hasham A, Sundaram N, Tomer Y. Diabetes and hepatitis C: A two-way association. Front Endocrinol (Lausanne) 2015;6:134.
- 5 Masini M, Campani D, Boggi U, Menicagli M, Funel N, Pollera M, et al. Hepatitis C virus infection and human pancreatic beta-cell dysfunction. Diabetes Care 2005;28:940-1.
- 6 Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998;352:854-65.
- 7 Razavi H, Elkhoury AC, Elbasha E, Estes C, Pasini K, Poynard T, et al. Chronic hepatitis C virus (HCV) disease burden and cost in the United States. Hepatology 2013;57:2164-70.
- 8 White DL, Ratziu V, El-Serag HB. Hepatitis C infection and risk of diabetes: A systematic review and meta-analysis. J Hepatol 2008;49:831-44.
- 9 Naing C, Mak JW, Ahmed SI, Maung M. Relationship between hepatitis C virus infection and type 2 diabetes mellitus: Meta-analysis. World J Gastroenterol 2012;18:1642-51.
- 10 Lecube A, Hernández C, Genescà J, Simó R. Glucose abnormalities in patients with hepatitis C virus infection: Epidemiology and pathogenesis. Diabetes Care 2006;29:1140-9.
- 11 Fraser GM, Harman I, Meller N, Niv Y, Porath A. Diabetes mellitus is associated with chronic hepatitis C but not chronic hepatitis B infection. Isr J Med Sci 1996;32:526-30.
- 12 Mason AL, Lau JY, Hoang N, Qian K, Alexander GJ, Xu L, et al. Association of diabetes mellitus and chronic hepatitis C virus infection. Hepatology 1999;29:328-33.
- 13 Tai TY, Lu JY, Chen CL, Lai MY, Chen PJ, Kao JH, et al. Interferon-alpha reduces insulin resistance and beta-cell secretion in responders among patients with chronic hepatitis B and C. J Endocrinol 2003;178:457-65.
- 14 Caronia S, Taylor K, Pagliaro L, Carr C, Palazzo U, Petrik J, et al. Further evidence for an association between non-insulin-dependent diabetes mellitus and chronic hepatitis C virus infection. Hepatology 1999;30:1059-63.
- 15 Ozyilkan E, Erbaş T, Simşek H, Telatar F, Kayhan B, Telatar H. Increased prevalence of hepatitis C virus antibodies in patients with diabetes mellitus. J Intern Med 1994;235:283-4.
- 16 Grimbert S, Valensi P, Lévy-Marchal C, Perret G, Richardet JP, Raffoux C, et al. High prevalence of diabetes mellitus in patients with chronic hepatitis C. A case-control study. Gastroenterol Clin Biol 1996;20:544-8.
- 17 Ryu JK, Lee SB, Hong SJ, Lee S. Association of chronic hepatitis C virus infection and diabetes mellitus in Korean patients. Korean J Intern Med 2001;16:18-23.
- 18 Antonelli A, Ferri C, Fallahi P, Pampana A, Ferrari SM, Goglia F, et al. Hepatitis C virus infection: Evidence for an association with type 2 diabetes. Diabetes Care 2005;28:2548-50.
- 19 Allison ME, Wreghitt T, Palmer CR, Alexander GJ. Evidence for a link between hepatitis C virus infection and diabetes mellitus in a cirrhotic population. J Hepatol 1994;21:1135-9.
- 20 Gulcan A, Gulcan E, Toker A, Bulut I, Akcan Y. Evaluation of risk factors and seroprevalence of hepatitis B and C in diabetic patients in Kutahya, Turkey. J Investig Med 2008;56:858-63.
Address for correspondence
Publication History
Received: 20 April 2019
Accepted: 07 December 2019
Article published online:
16 June 2022
© 2020. Gulf Association of Endocrinology and Diabetes (GAED). All rights reserved. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Latt TS, KK, Aye TT, Ko K. Report on National Survey of Diabetes Mellitus and Risk Factors for Non communicable Diseases in Myanmar in 2014. Myanmar: Ministry of Health; 2014.
- 2 World Health Organization | World Hepatitis Day 2017: Eliminate Hepatitis. World Health Organization; 2017.
- 3 Ni H, Moe S, Htet A. Hepatitis C virus infection in diabetes mellitus patients. Int J Collab Res Intern Med Public Health 2012;5:599-606.
- 4 Hammerstad SS, Grock SF, Lee HJ, Hasham A, Sundaram N, Tomer Y. Diabetes and hepatitis C: A two-way association. Front Endocrinol (Lausanne) 2015;6:134.
- 5 Masini M, Campani D, Boggi U, Menicagli M, Funel N, Pollera M, et al. Hepatitis C virus infection and human pancreatic beta-cell dysfunction. Diabetes Care 2005;28:940-1.
- 6 Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998;352:854-65.
- 7 Razavi H, Elkhoury AC, Elbasha E, Estes C, Pasini K, Poynard T, et al. Chronic hepatitis C virus (HCV) disease burden and cost in the United States. Hepatology 2013;57:2164-70.
- 8 White DL, Ratziu V, El-Serag HB. Hepatitis C infection and risk of diabetes: A systematic review and meta-analysis. J Hepatol 2008;49:831-44.
- 9 Naing C, Mak JW, Ahmed SI, Maung M. Relationship between hepatitis C virus infection and type 2 diabetes mellitus: Meta-analysis. World J Gastroenterol 2012;18:1642-51.
- 10 Lecube A, Hernández C, Genescà J, Simó R. Glucose abnormalities in patients with hepatitis C virus infection: Epidemiology and pathogenesis. Diabetes Care 2006;29:1140-9.
- 11 Fraser GM, Harman I, Meller N, Niv Y, Porath A. Diabetes mellitus is associated with chronic hepatitis C but not chronic hepatitis B infection. Isr J Med Sci 1996;32:526-30.
- 12 Mason AL, Lau JY, Hoang N, Qian K, Alexander GJ, Xu L, et al. Association of diabetes mellitus and chronic hepatitis C virus infection. Hepatology 1999;29:328-33.
- 13 Tai TY, Lu JY, Chen CL, Lai MY, Chen PJ, Kao JH, et al. Interferon-alpha reduces insulin resistance and beta-cell secretion in responders among patients with chronic hepatitis B and C. J Endocrinol 2003;178:457-65.
- 14 Caronia S, Taylor K, Pagliaro L, Carr C, Palazzo U, Petrik J, et al. Further evidence for an association between non-insulin-dependent diabetes mellitus and chronic hepatitis C virus infection. Hepatology 1999;30:1059-63.
- 15 Ozyilkan E, Erbaş T, Simşek H, Telatar F, Kayhan B, Telatar H. Increased prevalence of hepatitis C virus antibodies in patients with diabetes mellitus. J Intern Med 1994;235:283-4.
- 16 Grimbert S, Valensi P, Lévy-Marchal C, Perret G, Richardet JP, Raffoux C, et al. High prevalence of diabetes mellitus in patients with chronic hepatitis C. A case-control study. Gastroenterol Clin Biol 1996;20:544-8.
- 17 Ryu JK, Lee SB, Hong SJ, Lee S. Association of chronic hepatitis C virus infection and diabetes mellitus in Korean patients. Korean J Intern Med 2001;16:18-23.
- 18 Antonelli A, Ferri C, Fallahi P, Pampana A, Ferrari SM, Goglia F, et al. Hepatitis C virus infection: Evidence for an association with type 2 diabetes. Diabetes Care 2005;28:2548-50.
- 19 Allison ME, Wreghitt T, Palmer CR, Alexander GJ. Evidence for a link between hepatitis C virus infection and diabetes mellitus in a cirrhotic population. J Hepatol 1994;21:1135-9.
- 20 Gulcan A, Gulcan E, Toker A, Bulut I, Akcan Y. Evaluation of risk factors and seroprevalence of hepatitis B and C in diabetic patients in Kutahya, Turkey. J Investig Med 2008;56:858-63.