

Subscribe to RSS
DOI: 10.1055/a-1326-1143
Use of loop and clips to prevent migration of esophageal stent
Authors

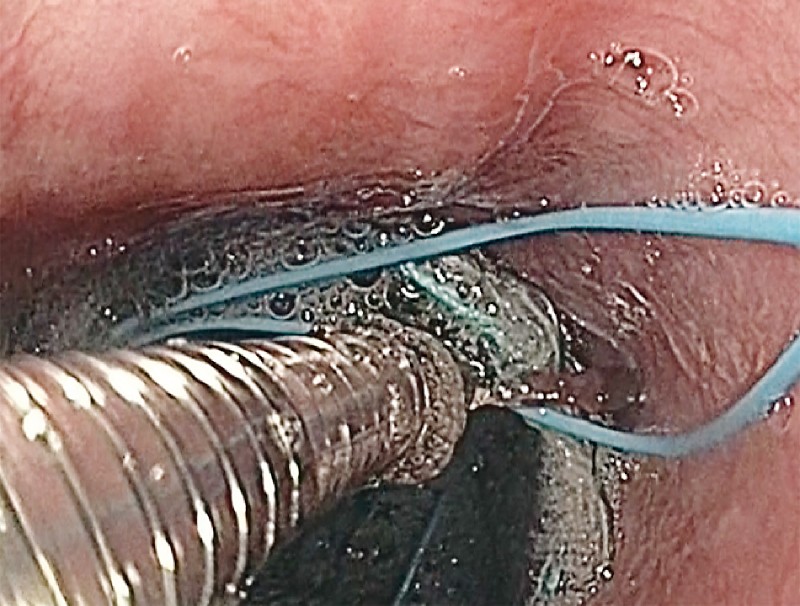
A 25-year-old gentleman presented with dysphagia for solids and liquids. He had a history of accidental ingestion of high-temperature melted iron particles 4 weeks back while working in the iron industry. Upper gastrointestinal endoscopy revealed a stricture with ulceration in the lower esophagus at 35 cm from the incisors ([Fig. 1]). The 9.8-mm diameter endoscope could not be negotiated beyond the stricture site; further examination with a 5.5-mm-diameter endoscope revealed a stricture length of 3 cm and normal gastric mucosa. The patient underwent four sessions of dilatation with Savary-Gilliard dilators up to 15 mm, but the stricture persisted. A fully covered esophageal self-expandable metal stent (18 × 100 mm; Wallflex, Boston Scientific) was deployed as a rescue treatment ([Fig. 2]). In view of the risk of migration, the stent was fixed to the esophageal wall with the help of an endoloop and clips ([Video 1]). A 30-mm endoloop (model no. MAJ-254; Olympus) was grasped with a forceps and partially pulled inside the channel ([Fig. 3]). The endoloop was released near the upper margin of the stent. One end of the loop was fixed with the help of through-the-scope clips (HX-610-090 L, Olympus) to the upper part of the stent ([Fig. 4]). Six clips were applied to fix the endoloop to the esophageal wall.


Video 1 Application of endoloop and clips to fix a self-expandable metal stent to the esophageal wall in order to prevent migration.

Fully covered metal stents are effective treatment for benign esophageal disease, but migration of the stent remains an important issue [1]. Various techniques have been used to prevent the migration of an esophageal stent. Over-the-scope clips [2], Shim technique [3], a suturing device [4], and a mucosal flap technique [5] have all been used to fix the stent. We have described a new technique using the widely available endoloop and through-the-scope clips.
Endoscopy_UCTN_Code_TTT_1AO_2AZ
Endoscopy E-Videos is a free access online section, reporting on interesting cases and new techniques
in gastroenterological endoscopy. All papers include a high
quality video and all contributions are
freely accessible online.
This section has its own submission
website at
https://mc.manuscriptcentral.com/e-videos
Publication History
Article published online:
27 January 2021
© 2021. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Thomas T, Abrams KR, Subramanian V. et al. Esophageal stents for benign refractory strictures: a meta-analysis. Endoscopy 2011; 43: 386-393
- 2 Watanabe K, Hikichi T, Nakamura J. et al. Feasibility of esophageal stent fixation with an over-the-scope-clip for malignant esophageal strictures to prevent migration. Endosc Int Open 2017; 5: E1044-E1049
- 3 Shim CS, Cho YD, Moon JH. et al. Fixation of a modified covered esophageal stent: its clinical usefulness for preventing stent migration. Endoscopy 2001; 33: 843-848
- 4 Kantsevoy SV, Bitner M. Esophageal stent fixation with endoscopic suturing device. Gastrointest Endosc 2012; 76: 1251-1255
- 5 Singla V, Arora A, Khare S. et al. A novel technique to prevent migration of esophageal stent. Endoscopy 2020; 52: 1040-1041