

Subscribe to RSS
DOI: 10.1055/a-1559-2391
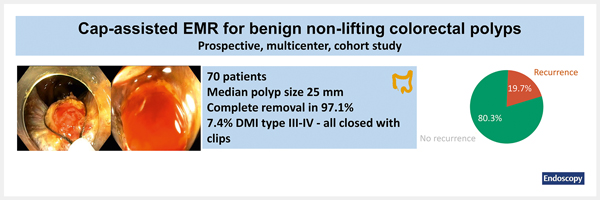
Efficacy and safety of cap-assisted endoscopic mucosal resection for treatment of nonlifting colorectal polyps
Authors


Abstract
Background Suboptimal lifting increases complexity of endoscopic mucosal resection (EMR) for benign colorectal polyps. Cap-assisted EMR (EMR-C) may allow fibrotic polyp tissue to be captured in the snare. This study evaluated the efficacy and safety of EMR-C for benign nonlifting colorectal polyps.
Methods This was a multicenter study, which prospectively registered all EMR-C procedures (2016–2018) for presumed benign nonlifting colorectal polyps.
Results 70 nonlifting polyps with a median size of 25 mm (interquartile range [IQR] 15–40) were treated with EMR-C. Complete polyp removal was achieved in 68 (97.1 %), including 47 (67.1 %) with EMR-C alone. Overall, 66 polyps showed benign histology, and endoscopic follow-up after a median of 6 months (IQR 6–10) showed recurrence in 19.7 %. First (n = 10) and second (n = 2) benign recurrences were all treated endoscopically. Deep mural injury type III–V occurred in 7.4 % and was treated successfully with clips.
Conclusion EMR-C may be an alternative therapeutic option for removal of benign nonlifting polyp tissue. Although recurrence still occurs, repeat endoscopic therapy usually leads to complete polyp clearance.
Publication History
Received: 12 November 2020
Accepted after revision: 03 July 2021
Article published online:
14 September 2021
© 2021. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Ferlitsch M, Moss A, Hassan C. et al. Colorectal polypectomy and endoscopic mucosal resection (EMR): European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy 2017; 49: 270-297
- 2 Moss A, Williams SJ, Hourigan LF. et al. Long-term adenoma recurrence following wide-field endoscopic mucosal resection (WF-EMR) for advanced colonic mucosal neoplasia is infrequent: results and risk factors in 1000 cases from the Australian Colonic EMR (ACE) study. Gut 2015; 64: 57-65
- 3 Kim HG, Thosani N, Banerjee S. et al. Effect of prior biopsy sampling, tattoo placement, and snare sampling on endoscopic resection of large nonpedunculated colorectal lesions. Gastrointest Endosc 2015; 81: 204-213
- 4 Burgess NG, Hourigan LF, Zanati SA. et al. Risk stratification for covert invasive cancer among patients referred for colonic endoscopic mucosal resection: a large multicenter cohort. Gastroenterology 2017; 153: 732-742
- 5 D’Amico F, Amato A, Iannone A. et al. Risk of covert submucosal cancer in patients with granular mixed laterally spreading tumors. Clin Gastroenterol Hepatol 2021; 19: 1395-1401
- 6 Veerappan SG, Ormonde D, Yusoff IF. et al. Hot avulsion: a modification of an existing technique for management of nonlifting areas of a polyp (with video). Gastrointest Endosc 2014; 80: 884-888
- 7 Kashani A, Lo SK, Jamil LH. Cap-assisted endoscopic mucosal resection is highly effective for nonpedunculated colorectal lesions. J Clin Gastroenterol 2016; 50: 163-168
- 8 Kato H, Haga S, Endo S. et al. Lifting of lesions during endoscopic mucosal resection (EMR) of early colorectal cancer: implications for the assessment of resectability. Endoscopy 2001; 33: 568-573
- 9 Burgess NG, Bassan MS, McLeod D. et al. Deep mural injury and perforation after colonic endoscopic mucosal resection: a new classification and analysis of risk factors. Gut 2017; 66: 1779-1789
- 10 Burgess NG, Metz AJ, Williams SJ. et al. Risk factors for intraprocedural and clinically significant delayed bleeding after wide-field endoscopic mucosal resection of large colonic lesions. Clin Gastroenterol Hepatol 2014; 12: 651-661
- 11 Tate DJ, Bahin FF, Desomer L. et al. Cold-forceps avulsion with adjuvant snare-tip soft coagulation (CAST) is an effective and safe strategy for the management of non-lifting large laterally spreading colonic lesions. Endoscopy 2018; 50: 52-62
- 12 Schmidt A, Beyna T, Schumacher B. et al. Colonoscopic full-thickness resection using an over-the-scope device: a prospective multicentre study in various indications. Gut 2018; 67: 1280-1289
- 13 Tanaka H, Oka S, Tanaka S. et al. Salvage endoscopic submucosal dissection for local residual/recurrent colorectal tumor after endoscopic resection: large multicenter 10-year study. Dig Endosc 2021; 33: 608-615
- 14 Holmes I, Kim HG, Yang DH. et al. Avulsion is superior to argon plasma coagulation for treatment of visible residual neoplasia during EMR of colorectal polyps (with videos). Gastrointest Endosc 2016; 84: 822-829
- 15 Kim HG, Thosani N, Banerjee S. et al. Underwater endoscopic mucosal resection for recurrences after previous piecemeal resection of colorectal polyps (with video). Gastrointest Endosc 2014; 80: 1094-1102