
Subscribe to RSS
DOI: 10.1055/a-2638-3159
Usefulness of bilateral traction method for endoscopic submucosal dissection of superficial pharyngeal cancer

Pharyngeal endoscopic submucosal dissection (ESD) has been increasingly performed as a minimally invasive treatment, similar to gastrointestinal ESD [1] [2]. However, the hypopharynx presents a challenging treatment area due to its complex anatomical structure and interference from the intubation tube, which limits the available working space. Various traction methods have been proposed to address these challenges [3] [4]. Previously, we reported the efficacy of the bilateral traction (BLT) method for colorectal ESD [5]. Herein, we report a case in which BLT facilitated hypopharyngeal ESD ([Video 1]).
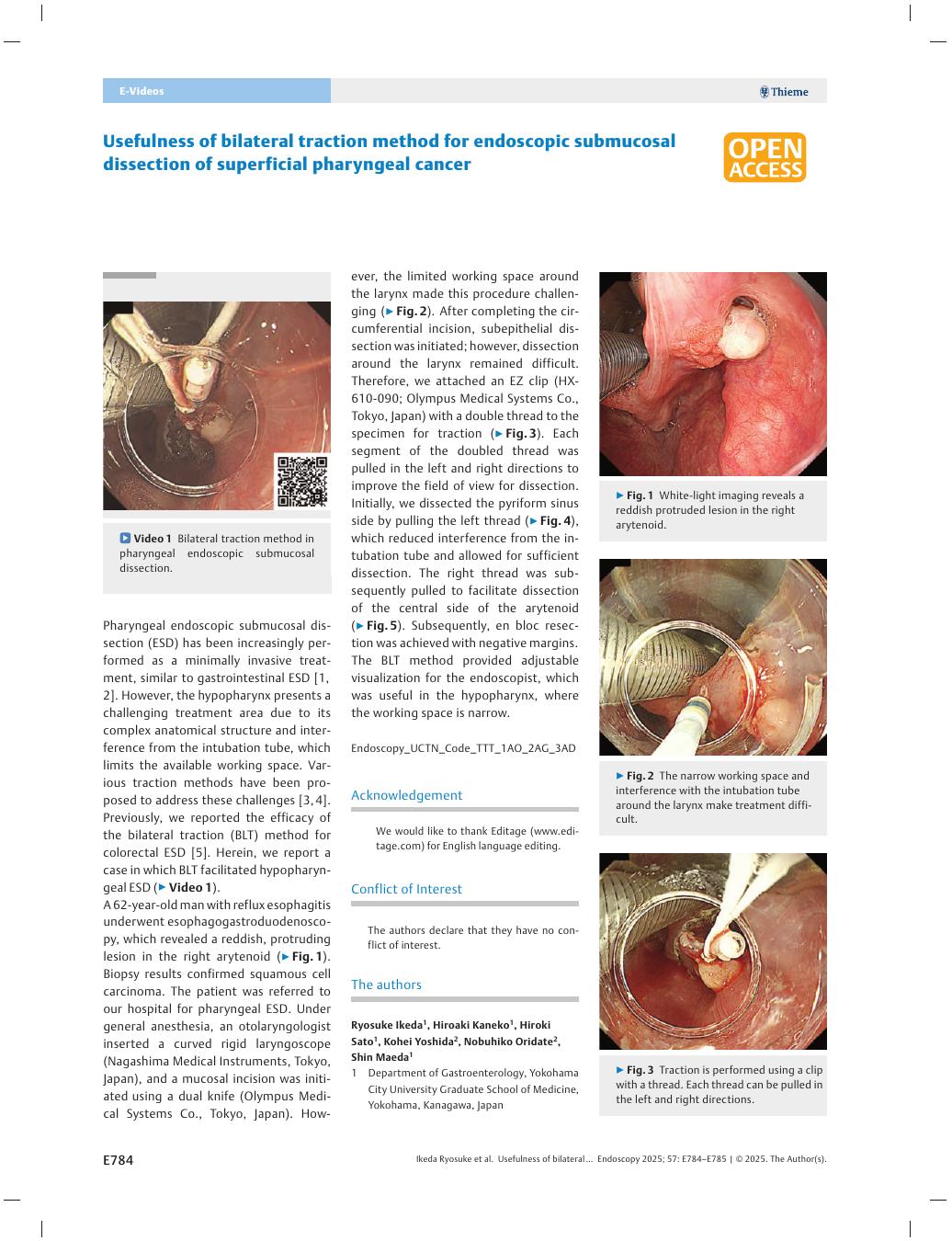
Bilateral traction method in pharyngeal endoscopic submucosal dissection.Video 1A 62-year-old man with reflux esophagitis underwent esophagogastroduodenoscopy, which revealed a reddish, protruding lesion in the right arytenoid ([Fig. 1]). Biopsy results confirmed squamous cell carcinoma. The patient was referred to our hospital for pharyngeal ESD. Under general anesthesia, an otolaryngologist inserted a curved rigid laryngoscope (Nagashima Medical Instruments, Tokyo, Japan), and a mucosal incision was initiated using a dual knife (Olympus Medical Systems Co., Tokyo, Japan). However, the limited working space around the larynx made this procedure challenging ([Fig. 2]). After completing the circumferential incision, subepithelial dissection was initiated; however, dissection around the larynx remained difficult. Therefore, we attached an EZ clip (HX-610-090; Olympus Medical Systems Co., Tokyo, Japan) with a double thread to the specimen for traction ([Fig. 3]). Each segment of the doubled thread was pulled in the left and right directions to improve the field of view for dissection. Initially, we dissected the pyriform sinus side by pulling the left thread ([Fig. 4]), which reduced interference from the intubation tube and allowed for sufficient dissection. The right thread was subsequently pulled to facilitate dissection of the central side of the arytenoid ([Fig. 5]). Subsequently, en bloc resection was achieved with negative margins.





The BLT method provided adjustable visualization for the endoscopist, which was useful in the hypopharynx, where the working space is narrow.
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AD
E-Videos is an open access online section of the journal Endoscopy, reporting on interesting cases and new techniques in gastroenterological endoscopy.
All papers include a high-quality video and are published with a Creative Commons
CC-BY license. Endoscopy E-Videos qualify for HINARI discounts and waivers and eligibility is automatically checked during the submission
process. We grant 100% waivers to articles whose corresponding authors are based in
Group A countries and 50% waivers to those who are based in Group B countries as classified
by Research4Life (see: https://www.research4life.org/access/eligibility/).
This section has its own submission website at https://mc.manuscriptcentral.com/e-videos.
Publication History
Article published online:
17 July 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Kuwabara T, Hiyama T, Oka S. et al. Clinical features of pharyngeal intraepithelial neoplasias and outcomes of treatment by endoscopic submucosal dissection. Gastrointest Endosc 2012; 76: 1095-1103
- 2 Hanaoka N, Ishihara R, Takeuchi Y. et al. Endoscopic submucosal dissection as minimally invasive treatment for superficial pharyngeal cancer: a phase II study (with video). Gastrointest Endosc 2015; 82: 1002-1008
- 3 Iizuka T, Kikuchi D, Hoteya S. et al. A new technique for pharyngeal endoscopic submucosal dissection: peroral countertraction (with video). Gastrointest Endosc 2012; 76: 1034-1038
- 4 Minami H, Tabuchi M, Matsushima K. et al. Endoscopic submucosal dissection of the pharyngeal region using anchored hemoclip with surgical thread: A novel method. Endosc Int Open 2016; 4: E828-E831
- 5 Ikeda R, Kaneko H, Sato H. et al. Bilateral traction method using a clip with thread for rectal endoscopic submucosal dissection. Endoscopy 2024; 56: E1131-E1132