

Subscribe to RSS
DOI: 10.1055/a-0851-6657
One-session combined technique for a recurrent rectal polyp: submucosal dissection and endoscopic full-thickness resection
Authors
Corresponding author
Publication History
Publication Date:
05 March 2019 (online)

The advent of endoscopic submucosal dissection (ESD) and endoscopic full-thickness resection (EFTR) have changed the treatment scenario for recurrent polyps, which represented one of the bigger challenges for endoscopists when endoscopic mucosal resection (EMR) was the only available technique. However, these two techniques have some limits: high grade fibrosis may reduce the possibility of performing ESD and increase the risk of perforation [1] [2], while the size, thickness, and rigidity of the lesion, the mobility of the wall, and the location and grade of fibrosis may limit EFTR [3] [4]. Our aim was to evaluate the feasibility, efficacy, and safety of a single-session combined technique performing ESD and EFTR for adenomatous recurrence in the rectum.
In 2014, a 65-year-old man underwent EMR of a tubulovillous adenoma with low grade dysplasia (LGD) with a diameter of 40 mm in the rectum. The 3-year follow-up colonoscopy showed an adenomatous recurrence of 25 mm, characterized by a sessile part and a flat part, positioned on the back of the second Huston’s valve. ESD appeared difficult to perform alone because of the high grade fibrosis of the sessile portion, while an approach with EFTR was unfeasible because of the size, rigidity, and back-fold position of the flat part. Therefore, we decided to perform a partial ESD of the back-fold flat portion, thereby obtaining lesion mobility to allow performance of EFTR of the whole lesion ([Video 1]).
Video 1 A recurrent rectal polyp is successfully treated in a same-session combined approach using first endoscopic submucosal dissection (ESD) and then endoscopic full-thickness resection (EFTR).
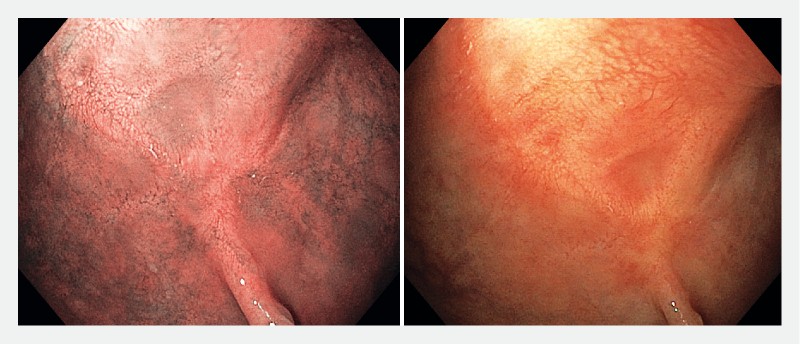
Histologic examination of the resected lesion showed an en bloc specimen of tubulovillous adenoma with LGD and free resection margins ([Fig. 1]). After 12 months of follow-up, there is no evidence of endoscopic or histologic recurrence ([Fig. 2]).

In conclusion, this one-session combined endoscopic technique could represent a valid option for the resection of “hard-to-treat” recurrent rectal polyps, thereby reducing the need for surgical treatment.
Endoscopy_UCTN_Code_TTT_1AQ_2AD
Endoscopy E-Videos is a free access online section, reporting on interesting cases and new techniques
in gastroenterological endoscopy. All papers include a high quality video and all
contributions are freely accessible online.
This section has its own submission website at https://mc.manuscriptcentral.com/e-videos
Competing interests
Vincenzo Cennamo: Olympus Italia, Olympus Europa, Euromedical, Novità Medicali.
-
References
- 1 Saito Y, Yamada M, So E. et al. Colorectal endoscopic submucosal dissection: Technical advantages compared to endoscopic mucosal re- section and minimally invasive surgery. Dig Endosc 2014; 26: 52-61
- 2 Kim ES, Cho KB, Park KS. et al. Factors predictive of perforation during endoscopic submucosal dissection for the treatment of colorectal tumors. Endoscopy 2011; 43: 573-578
- 3 Schmidt A, Bauerfeind P, Gubler C. et al. Endoscopic full-thickness resection in the colorectum with a novel over-the-scope device: first experience. Endoscopy 2015; 47: 719-725
- 4 Andrisani G, Pizzicannella M, Martino M. et al. Endoscopic full-thickness resection of superficial colorectal neoplasms using a new over-the-scope clip system: A single-centre study. Dig Liver Dis 2017; 49: 1009-1013
Corresponding author
-
References
- 1 Saito Y, Yamada M, So E. et al. Colorectal endoscopic submucosal dissection: Technical advantages compared to endoscopic mucosal re- section and minimally invasive surgery. Dig Endosc 2014; 26: 52-61
- 2 Kim ES, Cho KB, Park KS. et al. Factors predictive of perforation during endoscopic submucosal dissection for the treatment of colorectal tumors. Endoscopy 2011; 43: 573-578
- 3 Schmidt A, Bauerfeind P, Gubler C. et al. Endoscopic full-thickness resection in the colorectum with a novel over-the-scope device: first experience. Endoscopy 2015; 47: 719-725
- 4 Andrisani G, Pizzicannella M, Martino M. et al. Endoscopic full-thickness resection of superficial colorectal neoplasms using a new over-the-scope clip system: A single-centre study. Dig Liver Dis 2017; 49: 1009-1013