

Subscribe to RSS
DOI: 10.1055/a-1264-6949
Intentional endoscopic nasopancreatic drainage to a pancreatic fistula in the treatment of disconnected pancreatic duct syndrome
Authors

Endoscopic transpapillary stenting and/or transluminal drainage is recommended for disconnected pancreatic duct syndrome (DPDS). Transpapillary stenting can be considered, preferably with the stent bridging the disruption in the main pancreatic duct (MPD) [1] [2]. Such treatment is currently feasible for patients with partial, but not complete, MPD disruption [3] [4]. If this treatment fails, surgery is an alternative in patients with either partial or complete disruption – but the majority of these patients go on to develop diabetes mellitus [5]. For this reason, if possible, endoscopic treatment is preferred in order to preserve pancreatic function. We report a successful stent bridging technique for DPDS with complete MPD disruption after intentional endoscopic insertion of a nasopancreatic drainage (ENPD) tube into a pancreatic fistula.
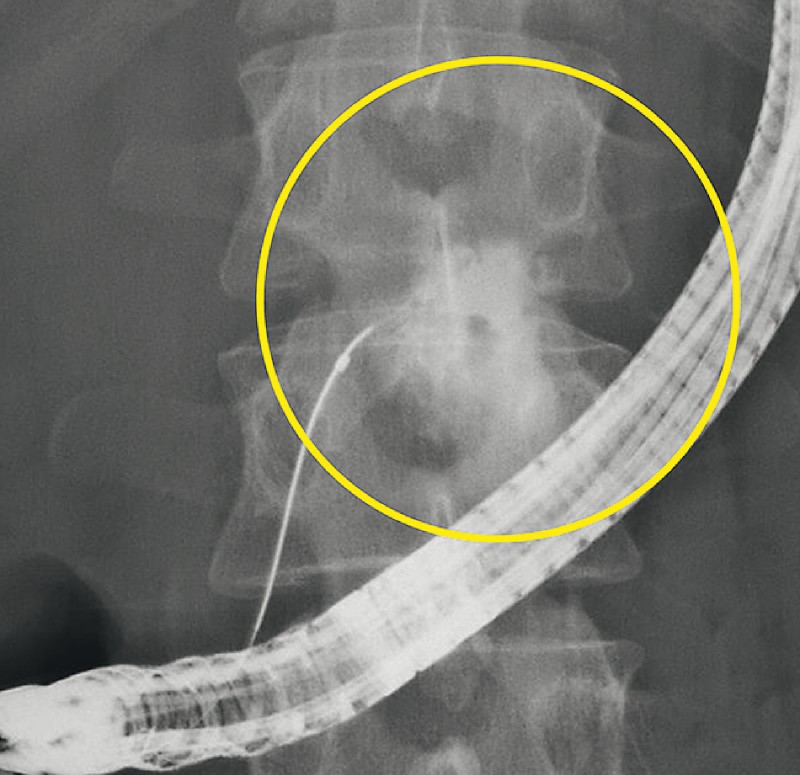
A 48-year-old man was diagnosed with DPDS caused by severe acute pancreatitis. The patient suffered from recurring unbearable pain related to a pancreatic fistula. The pancreatic fistula was not encapsulated ([Fig. 1]), so we performed transpapillary stenting rather than transluminal drainage. According to endoscopic retrograde pancreatography (ERP), the MPD in the body of the pancreas was completely disrupted ([Fig. 2]). The upstream MPD could not be visualized, and because it was difficult to bridge the disrupted MPD, we planned to temporarily place an ENPD tube in the unencapsulated pancreatic fistula. Flushing via an ENPD enabled cloudy waste fluid to be controlled, and peripancreatic fluid collection was absent ([Fig. 3]). Thereafter, we repeated ERP and identified the MPD in the tail of the pancreas beyond the disruption, which we successfully bridged ([Fig. 4]; [Video 1]). We then exchanged external for internal drainage and replaced the drain every 8 – 12 weeks. Six months later, we confirmed the absence of leakage by contrast pancreatography ([Fig. 5]) and removed the stent. The patient was cured and did not develop complications, including diabetes mellitus. The technique enables bridging of a completely disrupted MPD in patients with DPDS.



Video 1 Intentional endoscopic nasopancreatic drainage to a pancreatic fistula in the treatment of disconnected pancreatic duct syndrome.

Endoscopy_UCTN_Code_TTT_1AR_2AI
Endoscopy E-Videos is a free access online section, reporting on interesting cases and new techniques
in gastroenterological endoscopy. All papers include a high
quality video and all contributions are
freely accessible online.
This section has its own submission
website at
https://mc.manuscriptcentral.com/e-videos
Competing interests
The authors declare that they have no conflict of interest.
-
References
- 1 Varadarajulu S, Noone TC, Tutuian R. et al. Predictors of outcome in pancreatic duct disruption managed by endoscopic transpapillary stent placement. Gastrointest Endosc 2005; 61: 568-575
- 2 Hori Y, Vege SS, Chari ST. et al. Classic chronic pancreatitis is associated with prior acute pancreatitis in only 50 % of patients in a large single-institution study. Pancreatology 2019; 19: 224-229
- 3 Lawrence C, Howell DA, Stefan AM. et al. Disconnected pancreatic tail syndrome: potential for endoscopic therapy and results of long-term follow-up. Gastrointest Endosc 2008; 67: 673-679
- 4 Pelaez-Luna M, Vege SS, Petersen BT. et al. Disconnected pancreatic duct syndrome in severe acute pancreatitis: clinical and imaging characteristics and outcomes in a cohort of 31 cases. Gastrointest Endosc 2008; 68: 91-97
- 5 Pearson EG, Scaife CL, Mulvihill SJ. et al. Roux-en-Y drainage of a pancreatic fistula for disconnected pancreatic duct syndrome after acute necrotizing pancreatitis. HPB (Oxford) 2012; 14: 26-31
Corresponding author
Publication History
Article published online:
08 October 2020
© 2020. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Varadarajulu S, Noone TC, Tutuian R. et al. Predictors of outcome in pancreatic duct disruption managed by endoscopic transpapillary stent placement. Gastrointest Endosc 2005; 61: 568-575
- 2 Hori Y, Vege SS, Chari ST. et al. Classic chronic pancreatitis is associated with prior acute pancreatitis in only 50 % of patients in a large single-institution study. Pancreatology 2019; 19: 224-229
- 3 Lawrence C, Howell DA, Stefan AM. et al. Disconnected pancreatic tail syndrome: potential for endoscopic therapy and results of long-term follow-up. Gastrointest Endosc 2008; 67: 673-679
- 4 Pelaez-Luna M, Vege SS, Petersen BT. et al. Disconnected pancreatic duct syndrome in severe acute pancreatitis: clinical and imaging characteristics and outcomes in a cohort of 31 cases. Gastrointest Endosc 2008; 68: 91-97
- 5 Pearson EG, Scaife CL, Mulvihill SJ. et al. Roux-en-Y drainage of a pancreatic fistula for disconnected pancreatic duct syndrome after acute necrotizing pancreatitis. HPB (Oxford) 2012; 14: 26-31