

Subscribe to RSS
DOI: 10.1055/a-1333-0538
Small-caliber plastic stent for endoscopic ultrasound-guided drainage of a non-dilated pancreatic duct
Authors

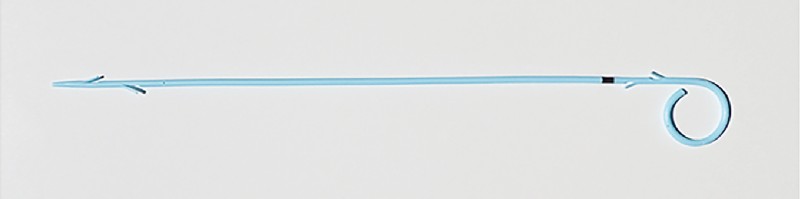
Endoscopic ultrasound (EUS)-guided pancreatic drainage is increasingly utilized in cases where endoscopic retrograde cholangiopancreatography (ERCP) is not possible [1] [2] [3]. EUS-guided pancreatic drainage for a non-dilated pancreatic duct (PD) not only poses technical challenges but also increases the risk of procedure-related pancreatitis as well as stent-induced ductal injury. A small-caliber stent might be suitable for a non-dilated PD to prevent ductal injury and upstream main duct obstruction, but there has been no report on a dedicated 5-Fr EUS-guided pancreatic drainage stent. Herein we present a newly designed 5-Fr plastic stent for EUS-guided pancreatic drainage (Through & Pass Type IT; Gadelius Medical, Tokyo, Japan) ([Fig. 1]), which is a thinner type of a previously reported stent [4].
A 75-year-old woman with a history of pancreatoduodenectomy for intraductal papillary mucinous neoplasm was hospitalized with a pancreatic fluid collection ([Fig. 2]). The fluid collection did not subside after percutaneous drainage, and therefore we decided to perform EUS-guided pancreatic drainage ([Video 1]). Under EUS guidance, we punctured the non-dilated main PD with a 19-gauge needle and inserted a 0.025-inch guidewire ([Fig. 3 a]). The needle tract was dilated using an ultra-tapered mechanical dilator (ES dilator; Zeon Medical, Tokyo, Japan) and a 4-mm-wide balloon dilator (REN; Kaneka, Osaka, Japan). Using a double-lumen catheter (Uneven Double Lumen Cannula; Piolax Medical Devices, Kanagawa, Japan), we successfully passed a 0.025-inch hydrophilic guidewire into the jejunum and additionally inserted a 0.035-inch guidewire to stabilize the scope position (“double guidewire technique”) ([Fig. 3 b]) [5]. After dilation of the pancreaticojejunostomy anastomosis using the balloon dilator, a 5-Fr stent was readily positioned from the jejunum to the stomach ([Fig. 3 c]). The postprocedural course was uneventful and the percutaneous drain was successfully removed. A follow-up CT scan 4 months later revealed the disappearance of the fluid collection without upstream ductal dilation.

Video 1 Endoscopic ultrasound-guided transmural placement of a 5-Fr plastic stent for a non-dilated pancreatic duct.

Our new 5-Fr plastic stent was feasible in the EUS-guided drainage of a non-dilated PD.
Endoscopy_UCTN_Code_TTT_1AS_2AD
Endoscopy E-Videos is a free access online section, reporting on interesting cases and new techniques
in gastroenterological endoscopy. All papers include a high
quality video and all contributions are
freely accessible online.
This section has its own submission
website at
https://mc.manuscriptcentral.com/e-videos
Competing interests
Dr. Itoi serves as a consultant of Gadelius Medical.
-
References
- 1 Kahaleh M, Artifon ELA, Perez-Miranda M. et al. EUS-guided drainage: summary of therapeutic EUS consortium meeting. Endosc Ultrasound 2019; 8: 151-160
- 2 Teoh AYB, Dhir V, Kida M. et al. Consensus guidelines on the optimal management in interventional EUS procedures: results from the Asian EUS group RAND/UCLA expert panel. Gut 2018; 67: 1209-1228
- 3 Itoi T, Kasuya K, Sofuni A. et al. Endoscopic ultrasonography-guided pancreatic duct access: techniques and literature review of pancreatography, transmural drainage and rendezvous techniques. Dig Endosc 2013; 25: 241-252
- 4 Matsunami Y, Itoi T, Sofuni A. et al. Evaluation of a new stent for EUS-guided pancreatic duct drainage: long-term follow-up outcome. Endosc Int Open 2018; 6: E505-E512
- 5 Nakai Y, Kogure H, Koike K. Double-guidewire technique for endoscopic ultrasound-guided pancreatic duct drainage. Dig Endosc 2019; 31: 65-66
Corresponding author
Publication History
Article published online:
14 January 2021
© 2021. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Kahaleh M, Artifon ELA, Perez-Miranda M. et al. EUS-guided drainage: summary of therapeutic EUS consortium meeting. Endosc Ultrasound 2019; 8: 151-160
- 2 Teoh AYB, Dhir V, Kida M. et al. Consensus guidelines on the optimal management in interventional EUS procedures: results from the Asian EUS group RAND/UCLA expert panel. Gut 2018; 67: 1209-1228
- 3 Itoi T, Kasuya K, Sofuni A. et al. Endoscopic ultrasonography-guided pancreatic duct access: techniques and literature review of pancreatography, transmural drainage and rendezvous techniques. Dig Endosc 2013; 25: 241-252
- 4 Matsunami Y, Itoi T, Sofuni A. et al. Evaluation of a new stent for EUS-guided pancreatic duct drainage: long-term follow-up outcome. Endosc Int Open 2018; 6: E505-E512
- 5 Nakai Y, Kogure H, Koike K. Double-guidewire technique for endoscopic ultrasound-guided pancreatic duct drainage. Dig Endosc 2019; 31: 65-66