Subscribe to RSS
DOI: 10.1055/a-1996-2980
Sonographic Monitoring of Growth of Uterine Myomas in Untreated Women and Respective Influence Factors
Article in several languages: English | deutschAuthors

Abstract
Research Question What are the growth patterns of uterine myomas in untreated premenopausal women? Which factors influence the growth rate of uterine myomas in premenopausal women?
Method All premenopausal women who presented to the outpatient myoma consultation clinic between January 2005 and March 2022 at least twice were screened. Exclusion criteria were hormonal therapy, pregnancy, and postmenopausal status.
Results A total of 189 patients were included in our study which focused on the respective largest uterine myoma of each woman. An ideal linear growth over time was assumed. Most myomas (82%) increased in size. The mean annual growth of these myomas was 68.42 cm3. The most important prognostic factor for growth was the initial size of the myoma. The absolute annual growth of myomas measuring > 50 cm3 at first presentation was higher compared to smaller myomas (p < 0.001). The relative annual growth rate was highest for myomas measuring between 20 and 50 cm3 at the initial presentation (p = 0.003). The relative annual growth rate in women older than 40 years was significantly lower than that in women below the age of 40 years (p = 0.003).
Conclusion Overall, it is difficult to make an individual prognosis about the growth pattern of a uterine myoma in a specific patient. It should be noted especially in asymptomatic patients that spontaneous regression of myoma size can also occur in premenopausal women.
Introduction
In most cases, uterine fibroids are asymptomatic (80%), but they can nevertheless severely reduce the quality of life of affected women [1], [2]. Myoma-related symptoms which should be investigated and treated include bleeding disorders, dysmenorrhea, and a feeling of pressure in the lesser pelvis as well as fertility disorders [3], [4]. Although in some patients the myoma can be quite large, expectant management is almost always possible for asymptomatic well-informed patients. Many patients have unfounded fears about their myoma findings which are often based on their own internet searches. It is important to first inform myoma patients that myomas are common at a certain age and are “normal”, that they are always benign and, according to current scientific knowledge, do not transform into malignant lesions. Myomas are often asymptomatic and therefore only constitute a finding, not a disease per se. Moreover, myomas are easily treatable and there are several different treatments.
Myomas tend to increase in size over the entire reproductive life span of a woman. However, there are currently no prospective studies on long-term myoma growth patterns over several years nor has there been a scientific evaluation of growth prognoses. There are only a few studies in the literature which have considered the natural growth patterns of fibroids in a narrow or wider sense. Some working groups use MRI images to monitor the progress of the fibroid [5] – [8]. A few working groups use vaginal ultrasound as it is less expensive and more commonly used in clinical gynecological practice [9], [10], [11], [12], [13]. Even though MRI findings are more reproducible compared to vaginal ultrasound, [14], MRI is still more expensive and complex in clinical practice.
Even now, a “myoma with a rapid increase in size” or a “rapidly growing myoma” is considered to indicate a developing sarcoma [15], but the criterion “rapid” (an increase in size by how many cm or cm3 per unit of time?) has not been properly defined. More than a decade ago, the American College of Obstetricians and Gynecologists already stated that this clinical diagnosis must not be the sole indication for myoma enucleation or hysterectomy [16], [17], [18], [19]. The German Society for Gynecology and Obstetrics has also pointed out in its appropriate guideline that no definition of what constitutes “rapid growth” of a sarcoma exists and that data about the significance of such changes is controversial [20]. Despite various attempts, there are still no clinical or imaging procedures which can unambiguously exclude sarcoma [21]. In clinical practice, patients are often upset if they present with a growing myoma, even though this type of growth is normal.
We recorded and analyzed the growth patterns of myomas in a large group of untreated premenopausal patients using ultrasound to obtain evidence for use in clinical practice.
Patient Cohort and Method
Inclusion criteria
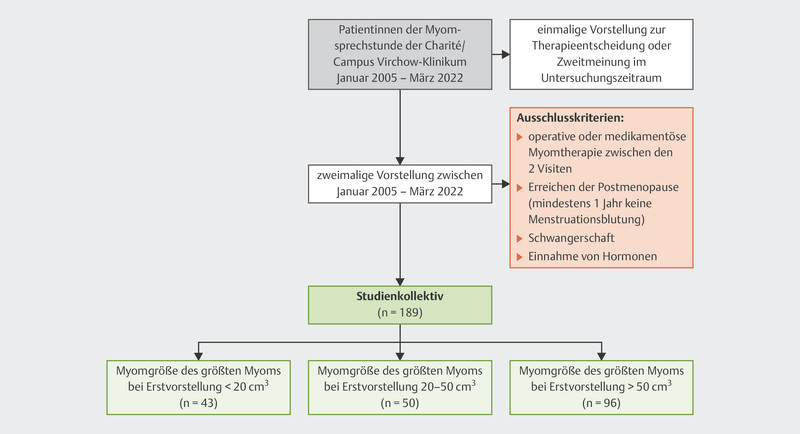
The data evaluation included all patients who presented to the outpatient myoma consultation clinic of Charité/Campus Virchow-Klinikum at least twice between January 2005 and March 2022. Additional inclusion criteria were: no surgical treatment or medication to treat the myoma between the two examinations, no postmenopausal status (no menstruation for at least one year), no pregnancy and no hormone treatment. The data of the largest myoma was recorded ([Fig. 1]). The vaginal ultrasound examinations to measure the myoma were all carried out by the same investigator (M. D.). If the fibroid was very big or imaging of the myoma was difficult using vaginal ultrasound, abdominal ultrasound was additionally carried out. The location (submucosal, subserous, transmural) and size (diameter in all three planes) of every fibroid was determined. The calculation of the myoma volume was done using a formula based on that of Ichimura et al. (1998) which is similar to the formula used to calculate the volume of ellipsoid shapes. If only two diameters were recorded, the third diameter was approximated by taking the mean value of the other two diameters.

Statistical evaluation
The statistical program SPSS 18.0 (SPSS Inc., Chicago, IL, USA) was used for data evaluation. The results were characterized using mean, median, standard deviation (SD) and interquartile range (IQR). Differences between selected characteristics were analyzed using non-parametric Mann-Whitney test. Linear and multiple regression analysis was carried out, using absolute difference in size, daily and annual growth rate and annual growth rate in percent as the dependent variables and age, initial size of the myoma, and location of the myoma as independent variables. Results were considered significant if the significance level was less than 5%. Because of the explorative nature of the study, no adjustment was done for multiple testing.
The anonymized data evaluation was discussed and approved by the Institutional Board of the hospital. The Statute of the Charité on Ensuring Good Scientific Practice and the stipulations of the Berlin law on data protection were complied with.
Results
Study cohort
A total of 189 women with myomas were included in the evaluation, although in each case only the differences in size of the patientʼs largest or dominant myoma were analyzed. The second visit to the myoma consultation clinic was unsystematic and was often initiated by the patient herself; the intervals between the two examinations therefore differed in length (mean 641 days, SD 501 days). [Table 1] shows information about the age distribution of the women included in the analysis, as well as whether they reported myoma-related symptoms and the location and size of the myoma.
|
Characteristics |
n |
% |
|
|---|---|---|---|
|
Age of the myoma patients (grouped) |
≤ 40 years |
104 |
55 |
|
> 40 years |
85 |
45 |
|
|
Myoma-related symptoms |
no |
74 |
39 |
|
yes |
115 |
61 |
|
|
Location (site of the myoma) |
submucosal |
6 |
3 |
|
subserous |
49 |
26 |
|
|
intramural |
133 |
71 |
|
|
Size of the myoma at first presentation |
< 20 cm3 |
43 |
23 |
|
20 – 50 cm3 |
50 |
26 |
|
|
> 50 cm3 |
96 |
51 |
Absolute difference in size over time
In 81.5% of examined cases, the myomas showed an increase in size. No significant differences were found between shrinking myomas and growing myomas with regard to the location of the myoma, the size of the myoma at first presentation, and the patientʼs age group. However, there was an important difference between the difference in size of shrinking myomas and growing myomas: the mean increase in size for growing myomas was 68.42 cm3, whereas the mean change in the size of shrinking myomas was only 17.03 cm3 (p < 0.001). As the interval between first and second examinations varied considerably and was random, the mean difference in size per day was calculated, using the formula

The mean difference per day for myomas increasing in size was 0.17 cm3 and the mean difference for shrinking myomas was 0.054 cm3 (p < 0.001). It should be noted that this assumes an ideal continual change in growth per unit of time.
When analyzing growing myomas, two additional time-corrected variables were calculated in addition to the primary endpoints “absolute growth of the myoma” (V2−V1) and “growth per day”: myoma growth per year (growthday × 365), using the formula

and relative annual growth (relative to the size of the myoma at the first examination) using the formula

Factor “myoma size at first examination”
We investigated whether the parameters “myoma size at first examination” and “age” affected myoma growth patterns. “Myoma size” was subdivided into three categories (< 20 cm3, 20 – 50 cm3, > 50 cm3) and “age” was divided into the groups ≤ 40 years and > 40 years. It was found that myoma size had a significant effect with regard to both the absolute and the relative increase in size. Myomas which were larger at the initial examination grew faster ([Table 2]). The biggest absolute annual growth was found for myomas which were > 50 cm3 at the first examination (mean: 99.3 cm3/year) compared to myomas which were smaller at the initial presentation (p < 0.001). However, the relative annual growth was greatest for myomas between 20 and 50 cm3 at the first examination (102%, p = 0.033).
|
Myoma size at first examination |
Absolute increase in size (V2−V1) (cm3) |
P value |
Annual growth (cm3/365 d) |
P value |
Relative growth/year (%) |
P value |
|
|---|---|---|---|---|---|---|---|
|
< 20 cm3 |
< 0.001 |
< 0.001 |
0.033 |
||||
|
N |
33 |
||||||
|
Mean |
13.0 |
8.4 |
81.5 |
||||
|
Median |
11.0 |
6.9 |
51.8 |
||||
|
SD |
11.1 |
7.7 |
90.4 |
||||
|
IQR |
11.0 |
8.3 |
59.0 |
||||
|
20 – 50 cm3 |
N |
38 |
|||||
|
Mean |
46.5 |
30.4 |
102.0 |
||||
|
Median |
26.0 |
22.5 |
85.4 |
||||
|
SD |
57.9 |
29.0 |
91.6 |
||||
|
IQR |
40.2 |
29.9 |
105.4 |
||||
|
> 50 cm3 |
N |
83 |
|||||
|
Mean |
100.5 |
99.3 |
73.4 |
||||
|
Median |
78.7 |
45.6 |
45.9 |
||||
|
SD |
94.1 |
152.4 |
88.5 |
||||
|
IQR |
117.0 |
89.0 |
75.2 |
Factors “age” and “location”
When age was taken into consideration, the relative myoma growth per year was significantly lower in women over the age of 40 years (mean 68.5%) compared to women up to the age of 40 years (mean 94.2%, p = 0.003) ([Table 3]). A significant difference with regard to myoma location was only found for V2−V1 (p = 0.025).
|
Age (grouped) |
Absolute increase in size (V2−V1) (cm3) |
P value |
Annual growth (cm3/365 d) |
P value |
Relative growth/year (%) |
P value |
|
|---|---|---|---|---|---|---|---|
|
≤ 40 years |
0.852 |
0.705 |
0.003 |
||||
|
N |
82 |
||||||
|
Mean |
69.9 |
71.4 |
94.2 |
||||
|
Median |
29.3 |
22.5 |
72.8 |
||||
|
SD |
89.0 |
121.9 |
82.6 |
||||
|
IQR |
67.8 |
59.3 |
103.7 |
||||
|
> 40 years |
N |
72 |
|||||
|
Mean |
67.7 |
53.1 |
68.5 |
||||
|
Median |
38.5 |
24.9 |
36.6 |
||||
|
SD |
76.7 |
116.8 |
96.3 |
||||
|
IQR |
93.0 |
49.4 |
69.4 |
Multivariate analysis
To predict myoma size over time, regression analysis was done to identify a linear association between the dependent variable “increase in size (volume)” and “time” between the two visits to the outpatient myoma consultation clinic ([Fig. 2]).

The prognostic values for growing myomas can be obtained using the following formula:
myoma size = 50.27 + 0.03 × time between the examinations (in days)
Multiple regression analysis confirmed the main result of univariate analysis. Myoma size at initial examination in 2 categories (≤ 50 cm3 versus > 50 cm3) had a significant and biggest impact on all studied endpoints (“V2−V1”, “growthday”, “growthyear” and “relative annual growthyear”; p < 0.001). Age and location played no significant role in multiple regression analysis.
Discussion
Many existing studies on myoma growth are based on MRI and therefore not particularly suitable for clinical practice [5], [7], [8], [22]. Although transvaginal ultrasound is slightly more inaccurate than MRI to detect and measure myomas [12], transvaginal ultrasound is a useful diagnostic procedure for investigating myomas and can be easily integrated into every gynecological examination; it also offers a high level of reproducibility and sufficient accuracy for daily clinical practice. In 2002, De Waay et al. published study results from a case series of asymptomatic women examined using vaginal ultrasound. The aim of their investigation was to determine the incidence and rate of regression of endometrial polyps and myomas. Only 18% had myomas (n = 18). At 2.5 years after the first examination, the mean myoma growth was found to be 1.2 cm (0.9 – 6.8 cm). In four women no myomas were visible at the second examination [10]. In 2010, Mavrelos et al. published another retrospective longitudinal study which used vaginal ultrasound to monitor myoma growth patterns. They were able to follow up 122 myoma patients between the ages of 27 and 45 years over an 8-year period. During the study period, the largest myoma of each patient increased by 35.2% per year. However, 21.3% of myomas investigated using vaginal ultrasound showed a significant reduction in size of at least 5% compared to the initial measurement within the space of one year [11].
The figures for our study cohort were similar: out of a total of 189 measured myomas, 35 (18.5%) shrank while 154 (81.5%) of the myomas increased in size. Peddada et al. (2008) also reported a regression rate of 7% after a relatively short observation period of 6 months for their cohort of 72 women investigated using MRI, with myoma shrinkage rates of more than 20% found in some of the women.
In our observational ultrasound-based study of myoma growth patterns in untreated women presented here, myomas which were large (> 50 cm3) at the first examination were found to show the greatest absolute growth per year, whereas myomas between 20 – 50 cm3 showed the greatest percentage growth. It is possible that a “critical” myoma size exists after which vascularization can no longer sustain the increase in size over the longer term. The literature on this is contradictory: one (MRI-based) study was able to show that larger myomas showed significantly fewer changes in terms of their short-term growth than smaller myomas [22]. Peddada et al. (2008) found that myoma location and myoma size, BMI of the woman, and parity had no impact [6]. According to Mavrelos et al. (2010), myoma size is an independent predictor for myoma growth. However, in the respective study small myomas (diameters of < 20 mm) were found to grow the fastest [11]. Mavrelos et al. examined all myomas of one of the women included in their study cohort. A study carried out in African-American women also found that the small myomas in particular tended to grow the most. At the same time, 23% of the small myomas also disappeared spontaneously [23]. In contrast, our analysis which only investigated the largest myoma in each woman, found that the greatest growth occurred in the group of medium-sized myomas (between 20 – 50 cm3). It is possible that if several myomas are present, this may affect the growth rate of individual myomas. The relative myoma growth per year was significantly higher in women up to the age of 40 years compared to women older than 40 years. This could reflect the gradual changes in hormone levels occurring before the onset of clinical symptoms of menopause. A decrease in inhibin-B and a consequent increase in FSH levels, particularly in the early follicular phase, is known to occur even before the occurrence of perimenopausal symptoms [24].
This attempt at predicting size over a period of time may be useful when counselling affected women in clinical practice, although it should also always be mentioned that some myomas may spontaneously shrink.
Limitations
-
The cohort was non-randomized but was randomly constituted.
-
The time which elapsed between examinations was not standardized.
-
There were very few submucosal myomas in the cohort.
-
Other factors influencing fibroid growth patterns such as pregnancy [25], hormonal influences [26], and genetic and molecular factors [27] were not included in the analysis.
Strengths and conclusions
-
Overall, it is difficult to make an individual prognosis about the growth behavior of myomas for a specific patient. This once again underscores the importance of following the current recommendations which state that tumor growth patterns should not be used if the suspected diagnosis is uterine sarcoma.
-
Our analysis provides a basis for discussing treatment with patients, particularly when caring for asymptomatic patients with myomas. The information about the natural growth patterns of myomas could reassure many women and persuade them to agree to a conservative approach. When planning therapy, it is also important to be aware that natural myoma regression can, in principle, occur in every premenopausal woman.
Conflict of Interest/Interessenkonflikt
The authors declare that they have no conflict of interest./Die Autorinnen/Autoren geben an, dass kein Interessenkonflikt besteht.
-
References/Literatur
- 1 Downes E, Sikirica V, Gilabert-Estelles J. et al. The burden of uterine fibroids in five European countries. Eur J Obstet Gynecol Reprod Biol 2010; 152: 96-102
- 2 Utz-Billing I, Rothmann K, Kentenich H. et al. Prätherapeutische Ängste, Erwartungen, Wünsche und Informiertheit von Frauen mit Uterus myomatosus. Geburtshilfe Frauenheilkd 2006; 66: 763-768
- 3 Segars JH, Parrott EC, Nagel JD. et al. Proceedings from the Third National Institutes of Health International Congress on Advances in Uterine Leiomyoma Research: comprehensive review, conference summary and future recommendations. Hum Reprod Update 2014; 20: 309-333
- 4 Istre O. Management of symptomatic fibroids: conservative surgical treatment modalities other than abdominal or laparoscopic myomectomy. Best Pract Res Clin Obstet Gynaecol 2008; 22: 735-747
- 5 Ichimura T, Kawamura N, Ito F. et al. Correlation between the growth of uterine leiomyomata and estrogen and progesterone receptor content in needle biopsy specimens. Fertil Steril 1998; 70: 967-971
- 6 Peddada SD, Laughlin SK, Miner K. et al. Growth of uterine leiomyomata among premenopausal black and white women. Proc Natl Acad Sci U S A 2008; 105: 19887-19892
- 7 Davis BJ, Haneke KE, Miner K. et al. The fibroid growth study: determinants of therapeutic intervention. J Womens Health (Larchmt) 2009; 18: 725-732
- 8 Kasai M, Ichimura T, Kawamura N. et al. Prediction of the shrinking rate of uterine leiomyoma nodules using needle biopsy specimens. Fertil Steril 2012; 98: 440-443
- 9 Tsuda H, Kawabata M, Nakamoto O. et al. Clinical predictors in the natural history of uterine leiomyoma: preliminary study. J Ultrasound Med 1998; 17: 17-20
- 10 DeWaay DJ, Syrop CH, Nygaard IE. et al. Natural history of uterine polyps and leiomyomata. Obstet Gynecol 2002; 100: 3-7
- 11 Mavrelos D, Ben-Nagi J, Holland T. et al. The natural history of fibroids. Ultrasound Obstet Gynecol 2010; 35: 238-242
- 12 Moshesh M, Peddada SD, Cooper T. et al. Intraobserver variability in fibroid size measurements: estimated effects on assessing fibroid growth. J Ultrasound Med 2014; 33: 1217-1224
- 13 Nieuwenhuis L, Keizer A, Stoelinga B. et al. Fibroid vascularisation assessed with three-dimensional power Doppler ultrasound is a predictor for uterine fibroid growth: a prospective cohort study. BJOG 2018; 125: 577-584
- 14 Levens ED, Wesley R, Premkumar A. et al. Magnetic resonance imaging and transvaginal ultrasound for determining fibroid burden: implications for research and clinical care. Am J Obstet Gynecol 2009; 200: 537.e1-537.e7
- 15 Diehl K, Alkatout I, Kanzow M. et al. Gutartige Tumoren des Uterus. Gynäkologe 2021; 54: 435-446
- 16 ACOG. ACOG practice bulletin. Alternatives to hysterectomy in the management of leiomyomas. Obstet Gynecol 2008; 112: 387-400
- 17 Parker WH. Uterine myomas: management. Fertil Steril 2007; 88: 255-271
- 18 Schwartz PE, Kelly MG. Malignant transformation of myomas: myth or reality?. Obstet Gynecol Clin North Am 2006; 33: 183-198 xii
- 19 Parker WH. Uterine Fibroids: clinical Features. In: Tinelli A, Malvasi A. eds. Uterine Myoma, Myomectomy and minimally invasive Treatments. Cham: Springer International Publishing; 2015: 39-52
- 20 Denschlag D, Ackermann S, Battista MJ. et al. Sarcoma of the Uterus. Guideline of the DGGG and OEGGG (S2k Level, AWMF Register Number 015/074, February 2019). Geburtshilfe Frauenheilkd 2019; 79: 1043-1060
- 21 Testa AC, Di Legge A, Bonatti M. et al. Imaging techniques for evaluation of uterine myomas. Best Pract Res Clin Obstet Gynaecol 2016; 34: 37-53
- 22 Day Baird D, Garrett TA, Laughlin SK. et al. Short-term change in growth of uterine leiomyoma: tumor growth spurts. Fertil Steril 2011; 95: 242-246
- 23 Baird DD, Patchel SA, Saldana TM. et al. Uterine fibroid incidence and growth in an ultrasound-based, prospective study of young African Americans. Am J Obstet Gynecol 2020; 223: 402.e1-402.e18
- 24 Burger HG, Dudley EC, Robertson DM. et al. Hormonal changes in the menopause transition. Recent Prog Horm Res 2002; 57: 257-276
- 25 Ghosh S, Naftalin J, Imrie R. et al. Natural History of Uterine Fibroids: A Radiological Perspective. Curr Obstet Gynecol Rep 2018; 7: 117-121
- 26 Müller A, Thiel F, Binder H. et al. Myome – Teil 1. Geburtshilfe Frauenheilkd 2004; 64: R229-R244
- 27 Müller A, Thiel F, Binder H. et al. Benigne Tumoren. Myome – Entstehung, Diagnostik und Klinik. Geburtshilfe Frauenheilkd 2012; 72: 705-707
Correspondence/Korrespondenzadresse
Publication History
Received: 09 September 2022
Accepted after revision: 01 December 2022
Article published online:
05 April 2023
© 2023. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References/Literatur
- 1 Downes E, Sikirica V, Gilabert-Estelles J. et al. The burden of uterine fibroids in five European countries. Eur J Obstet Gynecol Reprod Biol 2010; 152: 96-102
- 2 Utz-Billing I, Rothmann K, Kentenich H. et al. Prätherapeutische Ängste, Erwartungen, Wünsche und Informiertheit von Frauen mit Uterus myomatosus. Geburtshilfe Frauenheilkd 2006; 66: 763-768
- 3 Segars JH, Parrott EC, Nagel JD. et al. Proceedings from the Third National Institutes of Health International Congress on Advances in Uterine Leiomyoma Research: comprehensive review, conference summary and future recommendations. Hum Reprod Update 2014; 20: 309-333
- 4 Istre O. Management of symptomatic fibroids: conservative surgical treatment modalities other than abdominal or laparoscopic myomectomy. Best Pract Res Clin Obstet Gynaecol 2008; 22: 735-747
- 5 Ichimura T, Kawamura N, Ito F. et al. Correlation between the growth of uterine leiomyomata and estrogen and progesterone receptor content in needle biopsy specimens. Fertil Steril 1998; 70: 967-971
- 6 Peddada SD, Laughlin SK, Miner K. et al. Growth of uterine leiomyomata among premenopausal black and white women. Proc Natl Acad Sci U S A 2008; 105: 19887-19892
- 7 Davis BJ, Haneke KE, Miner K. et al. The fibroid growth study: determinants of therapeutic intervention. J Womens Health (Larchmt) 2009; 18: 725-732
- 8 Kasai M, Ichimura T, Kawamura N. et al. Prediction of the shrinking rate of uterine leiomyoma nodules using needle biopsy specimens. Fertil Steril 2012; 98: 440-443
- 9 Tsuda H, Kawabata M, Nakamoto O. et al. Clinical predictors in the natural history of uterine leiomyoma: preliminary study. J Ultrasound Med 1998; 17: 17-20
- 10 DeWaay DJ, Syrop CH, Nygaard IE. et al. Natural history of uterine polyps and leiomyomata. Obstet Gynecol 2002; 100: 3-7
- 11 Mavrelos D, Ben-Nagi J, Holland T. et al. The natural history of fibroids. Ultrasound Obstet Gynecol 2010; 35: 238-242
- 12 Moshesh M, Peddada SD, Cooper T. et al. Intraobserver variability in fibroid size measurements: estimated effects on assessing fibroid growth. J Ultrasound Med 2014; 33: 1217-1224
- 13 Nieuwenhuis L, Keizer A, Stoelinga B. et al. Fibroid vascularisation assessed with three-dimensional power Doppler ultrasound is a predictor for uterine fibroid growth: a prospective cohort study. BJOG 2018; 125: 577-584
- 14 Levens ED, Wesley R, Premkumar A. et al. Magnetic resonance imaging and transvaginal ultrasound for determining fibroid burden: implications for research and clinical care. Am J Obstet Gynecol 2009; 200: 537.e1-537.e7
- 15 Diehl K, Alkatout I, Kanzow M. et al. Gutartige Tumoren des Uterus. Gynäkologe 2021; 54: 435-446
- 16 ACOG. ACOG practice bulletin. Alternatives to hysterectomy in the management of leiomyomas. Obstet Gynecol 2008; 112: 387-400
- 17 Parker WH. Uterine myomas: management. Fertil Steril 2007; 88: 255-271
- 18 Schwartz PE, Kelly MG. Malignant transformation of myomas: myth or reality?. Obstet Gynecol Clin North Am 2006; 33: 183-198 xii
- 19 Parker WH. Uterine Fibroids: clinical Features. In: Tinelli A, Malvasi A. eds. Uterine Myoma, Myomectomy and minimally invasive Treatments. Cham: Springer International Publishing; 2015: 39-52
- 20 Denschlag D, Ackermann S, Battista MJ. et al. Sarcoma of the Uterus. Guideline of the DGGG and OEGGG (S2k Level, AWMF Register Number 015/074, February 2019). Geburtshilfe Frauenheilkd 2019; 79: 1043-1060
- 21 Testa AC, Di Legge A, Bonatti M. et al. Imaging techniques for evaluation of uterine myomas. Best Pract Res Clin Obstet Gynaecol 2016; 34: 37-53
- 22 Day Baird D, Garrett TA, Laughlin SK. et al. Short-term change in growth of uterine leiomyoma: tumor growth spurts. Fertil Steril 2011; 95: 242-246
- 23 Baird DD, Patchel SA, Saldana TM. et al. Uterine fibroid incidence and growth in an ultrasound-based, prospective study of young African Americans. Am J Obstet Gynecol 2020; 223: 402.e1-402.e18
- 24 Burger HG, Dudley EC, Robertson DM. et al. Hormonal changes in the menopause transition. Recent Prog Horm Res 2002; 57: 257-276
- 25 Ghosh S, Naftalin J, Imrie R. et al. Natural History of Uterine Fibroids: A Radiological Perspective. Curr Obstet Gynecol Rep 2018; 7: 117-121
- 26 Müller A, Thiel F, Binder H. et al. Myome – Teil 1. Geburtshilfe Frauenheilkd 2004; 64: R229-R244
- 27 Müller A, Thiel F, Binder H. et al. Benigne Tumoren. Myome – Entstehung, Diagnostik und Klinik. Geburtshilfe Frauenheilkd 2012; 72: 705-707