

Subscribe to RSS
DOI: 10.1055/a-2452-5130
The “line-band closure” technique: a new endoscopic traction method for closure of a large defect
Authors
Supported by: Pre-research fund of the Second Affiliated Hospital of Soochow University SDFEYLC2345
Supported by: Project of State Key Laboratory of Radiation Medicine and Protection, Soochow University GZK1202402

We describe the case of a 55-year-old woman with a solitary, yellow, subepithelial mass found in the large curvature of the stomach body on upper gastrointestinal endoscopy ([Fig. 1] a). The lesion had a size of 8 × 6 mm and was considered a neuroendocrine tumor. Endoscopic submucosal dissection (ESD) was performed to achieve complete resection of the lesion. After the lesion was removed, a 20 × 15 mm defect was left ([Fig. 1] b). In order to prevent delayed perforation and bleeding, the defect was closed.
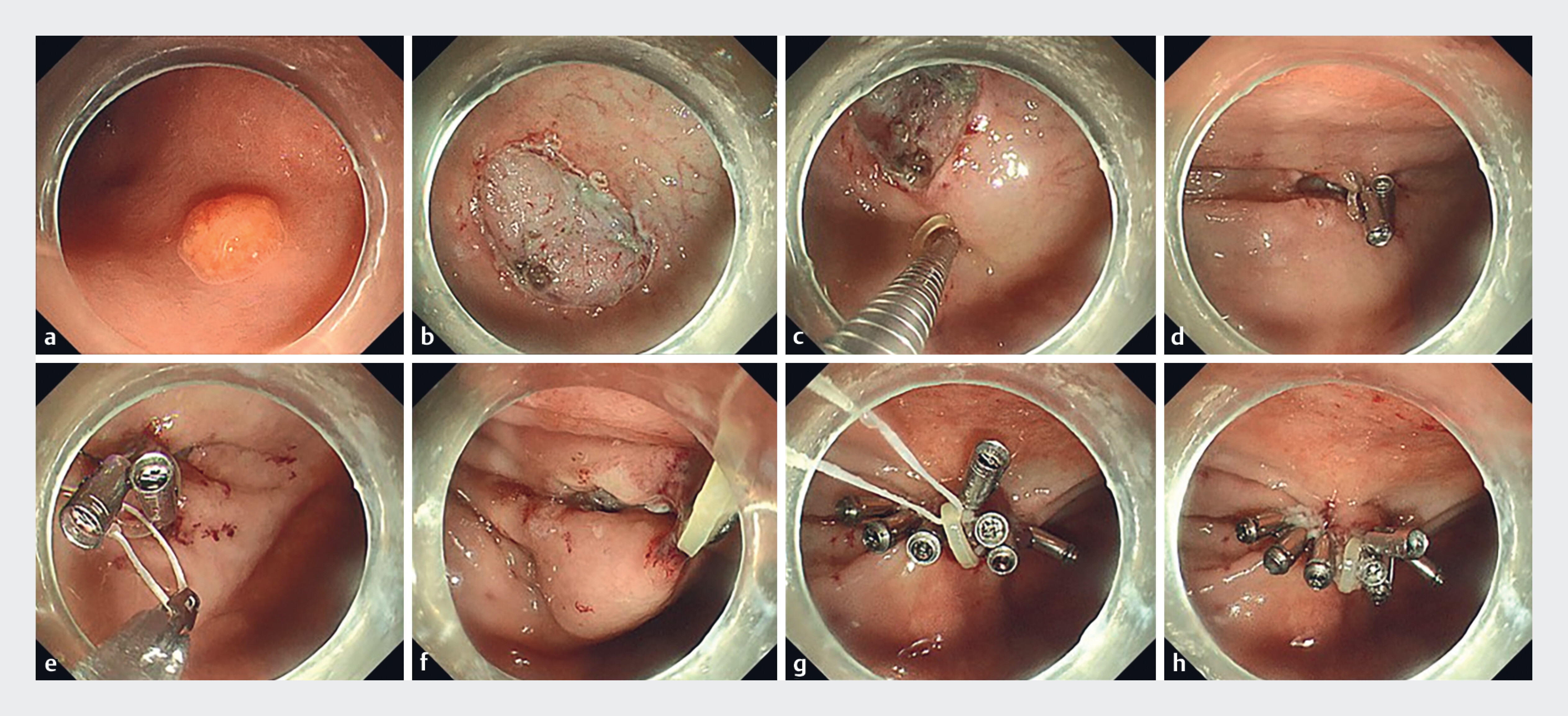
The procedure for defect closure was as follows ([Fig. 1] c–h, [Fig. 2], [Video 1]). 1) The clip with an orthodontic rubber band (5 mm in diameter; Xufei, Hangzhou, China) was attached to one side of the defect, and a second clip clamped the band and was attached to the opposite side of the defect to narrow the distance between the two sides. 2) A third clip was used to grasp a length of dental floss and pass it through the band. By extracorporeal traction, the defect was pulled up to form a tent-like peak, and the two sides of the defect were brought closer together and linearized. The defect was gradually closed from the traction point to both sides with clips. 3) After the defect was completely closed, the floss was slowly pull out.

Pathological examination revealed a neuroendocrine tumor (G1) with a negative margin. The patient had no adverse events and was discharged after 3 days.
The closure of large post-ESD mucosal defects is a challenge. Although new endoscopic closure techniques have sprung up in recent years, most of them require complex or specialized equipment and are technically challenging [1] [2] [3] [4]. In this report, we used dental floss combined with a rubber band to apply extracorporeal traction on the defect. By traction, the defect forms a tent-like peak, bringing the two sides closer together and linearizing the pseudo-suture path. In addition, traction improves and maintains the endoscopic field of view, even if there is a large perforation in the gastrointestinal wall and the stomach cavity is difficult to fill. We call this technique “line-band closure,” and it is simple, feasible, and safe, and may represent a useful new endoscopic closure technique.
Endoscopy_UCTN_Code_TTT_1AO_2AO
E-Videos is an open access online section of the journal Endoscopy, reporting on interesting cases and new techniques in gastroenterological endoscopy.
All papers include a high-quality video and are published with a Creative Commons
CC-BY license. Endoscopy E-Videos qualify for HINARI discounts and waivers and eligibility is automatically checked during the submission
process. We grant 100% waivers to articles whose corresponding authors are based in
Group A countries and 50% waivers to those who are based in Group B countries as classified
by Research4Life (see: https://www.research4life.org/access/eligibility/).
This section has its own submission website at https://mc.manuscriptcentral.com/e-videos.
Conflict of Interest
The authors declare that they have no conflict of interest.
-
References
- 1 Zhang Y, Wang X, Xiong G. et al. Complete defect closure of gastric submucosal tumors with purse-string sutures. Surg Endosc 2014; 28: 1844-1851
- 2 Liu XG, Chen ZY, Yang YC. et al. Combined preclosure technique and traction method facilitating endoscopic full-thickness resection of a gastric fundal gastrointestinal stromal tumor. Endoscopy 2020; 52: E293-E294
- 3 Aslanian HR, Sethi A. ASGE Technology Committee. et al. ASGE guideline for endoscopic full-thickness resection and submucosal tunnel endoscopic resection. VideoGIE 2019; 4: 343-350
- 4 Keihanian T, Zabad N, Khalaf M. et al. Safety and efficacy of a novel suturing device for closure of large defects after endoscopic submucosal dissection (with video). Gastrointest Endosc 2023; 98: 381-391
Correspondence
Publication History
Article published online:
13 November 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Zhang Y, Wang X, Xiong G. et al. Complete defect closure of gastric submucosal tumors with purse-string sutures. Surg Endosc 2014; 28: 1844-1851
- 2 Liu XG, Chen ZY, Yang YC. et al. Combined preclosure technique and traction method facilitating endoscopic full-thickness resection of a gastric fundal gastrointestinal stromal tumor. Endoscopy 2020; 52: E293-E294
- 3 Aslanian HR, Sethi A. ASGE Technology Committee. et al. ASGE guideline for endoscopic full-thickness resection and submucosal tunnel endoscopic resection. VideoGIE 2019; 4: 343-350
- 4 Keihanian T, Zabad N, Khalaf M. et al. Safety and efficacy of a novel suturing device for closure of large defects after endoscopic submucosal dissection (with video). Gastrointest Endosc 2023; 98: 381-391