
Subscribe to RSS
DOI: 10.1055/a-2521-0084
Endoscopic transpapillary gallbladder stenting vs percutaneous cholecystostomy for managing acute cholecystitis: Nationwide propensity score study

Abstract
Background and study aims
Cholecystectomy is the standard treatment for acute cholecystitis, but it may not be suitable for all patients. For those who cannot undergo surgery, a percutaneous cholecystostomy tube (PCT) and ERCP-guided transpapillary gallbladder drainage are viable options. We aimed to perform a nationwide study to assess 30-day readmission rates, adverse events (AEs), and mortality rates in these two cohorts.
Patients and methods
We conducted a nationwide cohort study using data from the Nationwide Readmissions Database (NRD) from 2016 to 2019. We identified patients with acute cholecystitis during the index admission who underwent either PCT or ERCP-guided gallbladder drainage. Propensity score matching along with multivariable regression was used to compare cohorts.
Results
During the study period, 3,592 patients (average age 63.0 years) underwent endoscopic drainage, whereas 80,372 patients (average 70.8 years) underwent Interventional Radiology drainage. Utilizing multivariate Cox regression analysis, compared with ERCP, PCT had a higher risk for 30-day readmission (adjusted hazard ratio [aHR] 1.47; 95% confidence interval [CI] 1.27 to 1.71; P < 0.001). The PCT group had a significantly higher rate of readmission for acute cholecystitis compared with the ERCP group (2.72% vs 0.86%; P < 0.005). Cox proportional hazard ratio showed a 3.41-fold increased risk (95% CI 1.99 to 5.84) for readmission in the PCT group. ERCP was consistently associated with lower rates of post-procedural AEs compared with PCT including acute hypoxemic respiratory failure (P < 0.001), acute renal failure (P < 0.001), shock (P < 0.001), and need for blood transfusions (P < 0.001).
Conclusions
Our nationwide analysis revealed that ERCP-guided gallbladder drainage should be the preferred approach for managing acute cholecystitis when unfit for surgery.
Introduction
Acute cholecystitis is a common condition that typically requires surgical intervention. However, in high-risk patients who are poor surgical candidates, alternative drainage methods are necessary [1]. Two primary techniques for non-surgical gallbladder drainage include endoscopic retrograde cholangiopancreatography (ERCP)-guided transpapillary gallbladder drainage and percutaneous cholecystostomy (PTC) [2].
PTC has long been the standard approach for non-surgical management of acute cholecystitis, offering high technical success rates and immediate symptom relief [3]. However, it requires external drainage, which can lead to patient discomfort and complications such as drain dislodgement or infection. ERCP-guided drainage is a minimally invasive alternative, allowing for internal drainage without need for external catheters [4] [5]. Although endoscopic ultrasound-guided drainage (EUS-GB) has grown in popularity in the last few years, it is limited to tertiary clinical centers and expert endoscopists. Thus, ERCP-guided drainage is an appealing clinical option in areas with limited resources.
Although both techniques have demonstrated efficacy in managing acute cholecystitis, comparative outcomes between ERCP-guided drainage and PTC remain unclear, particularly in terms of population-level readmission rates, mortality, and procedure complications. Previous studies have been limited by small sample sizes or single-center designs, potentially limiting their generalizability [2] [6] [7].
Despite use of ERCP-guided gallbladder drainage and PTC for acute cholecystitis in high-risk patients, large-scale comparative data on their outcomes remain limited. This study aimed to evaluate 30-day readmission rates, in-hospital mortality, and complications associated with these two techniques using the Nationwide Readmissions Database (NRD). By employing propensity score matching, we seek to provide a comprehensive, nationally representative assessment of these gallbladder drainage methods to inform clinical decision-making.
Patients and methods
Study design and data source
We conducted a retrospective cohort study using data from the NRD for the years 2016 to 2019. The NRD, developed and maintained by the Healthcare Cost and Utilization Project (HCUP) from the Agency for Healthcare Research and Quality, is the largest publicly available, nationally representative all-payer database for inpatient care in the United States. In 2019, the NRD included approximately 18 million discharges from 2,430 hospitals across 28 states, representing 60% of the total US resident population and 57% of all hospitalizations in the country.
The NRD collects data on patient demographics, diagnoses, procedures, and resource utilization from all HCUP hospital partners. Hospitals are stratified by ownership/control, bed size (small, medium, and large), teaching status, urban/rural location, and patient location according to National Center for Health Statistics (NCHS) Urban-Rural destination. Each discharge is weighted to ensure that the NRD is nationally representative. The NRD is a unique resource for studying hospital readmissions because it allows researchers to track patients across different hospitalizations within the same state and year. To allow for unbiased analysis of unplanned all-cause 30-day readmissions, we excluded patients who died during the index admission and whose discharges occurred in December because they would not have a full 30-day follow-up period.
Study population and variables
We identified patients with acute cholecystitis during index admission who underwent either ERCP-guided gallbladder drainage or PTC using ICD-10-CM and ICD-10-PCS codes (K81.0, K80.63, K80.62, K80.43, K80.42, K80.00, K80.01 for acute cholecystitis; 0F9480Z, 0F948ZX, 0F948ZZ, 0F954ZX, 0F957ZX, 0F958ZX, 0F964ZX, 0F967ZX, 0F968ZX, 0F977ZX, 0F978ZX, 0F988ZX, 0F997ZX, 0F998ZX, 0F9C80Z, 0F9980Z, 0FC58ZZ, 0FC68ZZ, 0FC78ZZ, 0FR58JZ, 0FR68JZ, 0FR78JZ, 0FR88JZ, 0FR98JZ for ERCP-guided gallbladder drainage; 0F9430Z, 0F943ZX, 0F943ZZ, 0F753DZ, 0F753ZZ, 0F763DZ, 0F763ZZ, 0F773DZ, 0F773ZZ, 0F783DZ, 0F783ZZ, 0F793DZ, 0F793ZZ, 0F993ZZ, 0F994ZZ, 0FC53ZZ, 0FC54ZZ, 0FC63ZZ, 0FC64ZZ, 0FC73ZZ, 0FC74ZZ, 0FC83ZZ, 0FC84ZZ, 0FC93ZZ for PTC). Patient-level data included age, sex, income in patient zip code, procedures, discharge disposition, length of stay, and total hospitalization charges. Hospital-level data included teaching status, bed size, and urban/rural location. The Elixhauser comorbidity score was calculated for each patient.
Outcomes
The primary outcome was the 30-day all-cause readmission rate, defined as a second admission to the same or another hospital within 30 days of index admission discharge. If multiple readmissions occurred within 30 days, only the first was captured. Secondary outcomes included procedures performed during the index admission, in-hospital mortality rates of index admission, length of stay, total hospitalization charges, and independent predictors of 30-day readmission. Additional secondary outcomes included rates of post-procedure adverse events (AEs) such as acute hypoxemic respiratory failure, acute renal failure, shock, need for blood transfusions, need for mechanical intubation, and lower gastrointestinal bleeding. In addition, we evaluated specific biliary-related events such as acute cholecystitis, biliary pancreatitis, choledocholithiasis, and acute cholangitis.
In addition, we performed a sensitivity analysis using propensity score matching to ensure comparability between treatment groups. We employed the nearest-neighbor matching method, matching patients on key variables including age, gender, hospital characteristics (such as teaching status and bed size), and Charlson Comorbidity Index. This approach allowed us to balance covariates between groups and reduce potential confounding, ensuring that compared groups had similar baseline characteristics and a more robust estimation of treatment effects. Covariates were visualized using the two-way plot (Supplementary Fig. 1).
Statistical analysis
Descriptive statistics were used to summarize patient and hospital characteristics. Categorical variables were compared using Chi-square or Fisher's exact test, whereas continuous variables were compared using Student's t-test. Multivariable Cox regression analysis was performed to identify independent predictors of 30-day readmission, controlling for potential confounders. Multivariable regression models were used to adjust for confounders and were built using the following method. Univariable regression analyses on possible confounding factors were used to calculate the unadjusted hazard ratio. Those with P ≤ 0.2 were chosen as potential confounding factors. These potential confounding factors were then added to the final multivariable regression model. Similarly, multivariable logistic regression analysis was used to analyze index admission mortality. Kaplan-Meier curves were constructed to visualize readmission rates over the 30-day follow-up period. All analyses accounted for the complex sampling design and weighting of the NRD to produce nationally representative estimates. Two-sided P < 0.05 was considered statistically significant. Analyses were performed using Stata (Version 17.0, College Station, Texas, United States).
Results
Baseline study population characteristics
Baseline demographics and hospital characteristics differed between the two groups ([Table 1]). Patients undergoing ERCP-guided drainage were more likely to be female (51.60% vs 40.62%; P < 0.001), have private insurance (26.81% vs. 15.50%; P < 0.001), and have certain comorbidities such as hypertension (42.2% vs. 38.02%; P < 0.001), liver disease (8.04% vs. 5.64%; P < 0.001), and peptic ulcer disease (3.35% vs. 1.34%; P < 0.001). In contrast, the PTC group was older (mean age 70.97 vs. 63.01 years; P < 0.001) with higher rates of congestive heart failure (25.79% vs. 11.77%; P < 0.001) and peripheral vascular disease (5.02% vs. 2.42%; P < 0.001). The number of procedures increased over the study period, with ERCP-guided drainage rising from 798 cases in 2016 to 1,208 in 2019, and PTC increasing from 18,833 to 22,479 cases.
Hospital readmission
In our study cohort, the PTC group had a significantly higher 30-day readmission rate compared with ERCP-guided drainage (20.67% vs. 12.76%; P < 0.001). Utilizing multivariable Cox regression analysis, compared with ERCP-guided gallbladder drainage, PTC had a higher 30-day readmission risk (adjusted hazard ratio 1.47; 95% confidence interval [CI] 1.27–1.71; P < 0.001) ([Fig. 1] and [Fig. 2]). Other notable clinical predictors for 30-day readmission included higher Elixhauser comorbidity index, alcoholic liver disease, and congestive heart failure.


Our propensity score-matched cohort compared patients who underwent PTC and ERCP-guided gallbladder drainage. The Charlson Comorbidity Index was also comparable, with no significant differences observed (P = 0.932) (Supplementary Table 1). In this analysis, we observed that the all-cause readmission rate for the PTC group was 17.88% (95% CI 14.70–21.57), whereas the readmission rate for the ERCP-guided gallbladder drainage group was 12.47% (95% CI 9.78–15.78) (Supplementary Fig. 2).
Morbidity and mortality
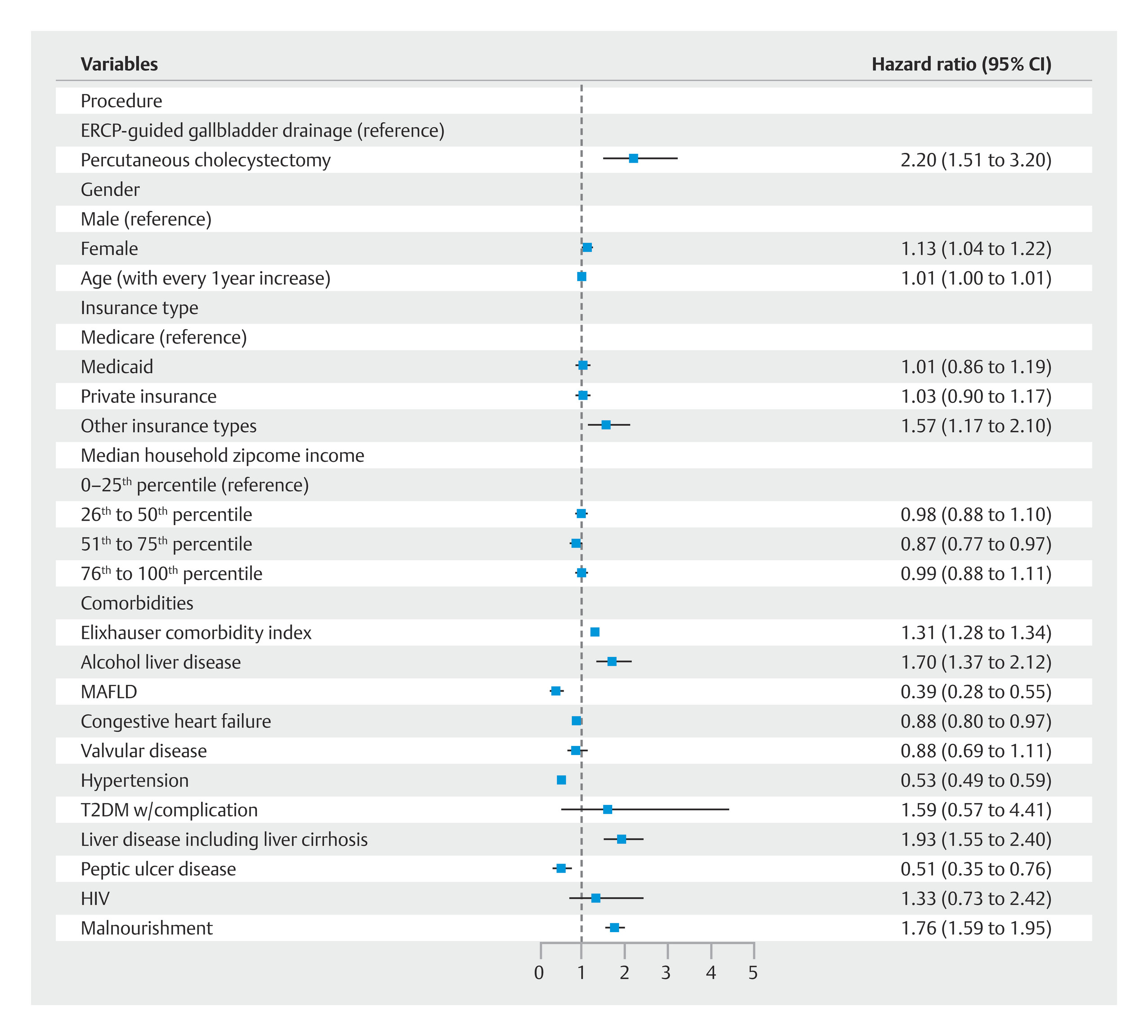
During index admission, PTC was associated with a higher mortality rate (8.15% vs 2.50%; P < 0.001). Using multivariate logistic regression analysis, we observed PTC had higher odds for index admission mortality (adjusted odds ratio: 2.20; 95% CI: 1.51 to 3.20; P < 0.001). Other predictors for index admission mortality are shown in [Fig. 3]. ERCP-guided drainage was consistently associated with lower rates of in-hospital AEs compared with PTC. These included acute hypoxemic respiratory failure (6.69% vs 18.48%; P < 0.001), acute renal failure (18.22% vs 40.91%; P < 0.001), shock (0.47% vs 1.15%; P < 0.001), and need for blood transfusions (3.27% vs 8.13%; P < 0.001), vasopressors (1.25% vs 4.08%; P < 0.001), and mechanical ventilation (1.25% vs 4.08%; P < 0.001). The exception was a similar occurrence of lower gastrointestinal bleeding (11.98% vs 11.02%; P = 0.226) ([Table 2]).
Readmission causes were analyzed for both ERCP-guided procedures and PTC. The overall rate of biliary-related readmissions was 2.78% (95% CI 2.10%-3.68%) for ERCP procedures and 3.62% (95% CI 3.42%-3.83%) for PTC. When examining specific conditions, cholangitis accounted for 1.16% of ERCP readmissions (95% CI 0.72–1.89%) and 0.36% of PTC readmissions (95% CI 0.30–0.43%). Acute biliary pancreatitis was responsible for 0.28% of ERCP readmissions (95% CI 0.13%-0.64%) and 0.24% of PTC readmissions (95% CI 0.19%-0.29%). Choledocholithiasis led to readmission in 0.56% of ERCP cases (95% CI 0.32%-1.00%) and 0.48% of PTC cases (95% CI 0.41%-0.57%). For acute cholecystitis, the readmission rate was 1.06% (95% CI 0.44%-2.52%) in the ERCP group compared with 3.53% (95% CI 2.20%-5.62%) in the PTC group, with Cox proportional hazards analysis showing a 3.41-fold increased risk (95% CI 1.99%-5.84) in the PTC group in reference to the ERCP-guided group ([Fig. 4]).

In the propensity score-matched analysis, the 30-day readmission rate for acute cholecystitis was significantly different between the two procedures. For the ERCP-guided procedure, the readmission rate was 1.06% (95% CI 0.44–2.52). In contrast, the PTC group had a higher readmission rate of 3.53% (95% CI 2.20–5.62). These findings indicate a higher likelihood of 30-day readmissions for patients undergoing PTC compared with those receiving the ERCP-guided approach.
Discussion
Our nationwide cohort study comparing ERCP-guided gallbladder drainage and PTC in patients with acute cholecystitis revealed several significant clinical findings. ERCP-guided drainage was associated with substantially lower 30-day readmission rates compared with PTC (12.76% vs. 20.67%, P < 0.001). After adjusting for potential confounders, PTC carried a 47% higher risk of 30-day readmission. In addition, ERCP-guided drainage demonstrated lower index admission mortality (2.50% vs. 8.15%, P < 0.001) and reduced rates of several inpatient AEs, including acute hypoxemic respiratory failure, acute renal failure, shock, and need for blood transfusions, vasopressors, and mechanical ventilation (P < 0.001 for all comparisons). The overall rate of biliary-related readmissions was 2.78% (95% CI 2.10%-3.68%) for ERCP procedures and 3.62% (95% CI 3.42%-3.83%) for PTC. Notably, the PTC group had a significantly higher rate of readmission specifically for acute cholecystitis compared with the ERCP-guided drainage group (2.72% vs. 0.86%, P < 0.005), with a 3.41-fold increased risk as shown by Cox proportional hazards analysis.
These findings extend the existing literature on gallbladder drainage techniques for acute cholecystitis in high-risk patients. Our study addressed baseline differences between the two groups including multivariate analysis and propensity score matching. Notably, in the propensity-matched analysis, mean age of the two cohorts was not significantly different, suggesting that the observed outcome differences are less likely to be driven by age-related factors. This careful adjustment for baseline characteristics enhances the robustness of our results and supports the possibility that ERCP-guided drainage may offer superior clinical outcomes compared with PTC. Our results are consistent with some studies [5] [8], which reported significantly lower readmission rates with ERCP-guided drainage—a finding similar to our observations. However, they contrast with other studies [9] [10], which found no significant difference in readmission rates between endoscopic and percutaneous approaches. Despite these variations, there is a consistent trend across the literature showing lower reintervention rates associated with endoscopic approaches [7] [11] [12].
The lower readmission rates for recurrent acute cholecystitis in the ERCP-guided group can be attributed to fundamental differences between the procedures. Percutaneous drainage typically involves an external catheter, prone to complications such as dislodgement, infection, and bile leakage [13]. In contrast, ERCP-guided transpapillary drainage creates an internal drainage pathway, eliminating issues associated with external tubes and allowing for more physiologic bile flow [14]. Siddiqui et al [8]. reported significantly lower unplanned hospital readmission rates with transpapillary drainage (3.2%) compared with percutaneous drainage (19.8%). This is supported by a recent meta-analysis [15], which found a recurrent cholecystitis rate of only 3% for transpapillary drainage, compared with published rates of 22% for percutaneous drainage in other studies [16].
In addition, transpapillary drainage requires fewer additional interventions. Siddiqui et al [8] found that only 11% of transpapillary drainage patients needed additional surgical intervention, versus 49% in the percutaneous group. The internal nature of transpapillary drainage also allows for longer-term management in poor surgical candidates. Studies have noted that plastic stents used in transpapillary drainage can remain patent for extended periods, with bile flowing both through and around the stent, potentially reducing recurrent cholecystitis risk [17]. These factors collectively contribute to better outcomes and lower unplanned readmission rates observed with ERCP-guided transpapillary drainage, making it a viable option for gallbladder drainage in high-risk patients with acute cholecystitis.
The clinical implications of our study are significant for management of acute cholecystitis in high-risk surgical candidates. To this end, patients with a higher comorbidity index were found to be at a higher risk for hospital readmission. Lisotti et al. reported a similar finding where patients with higher Charlson Comorbidity Index were found to be at a higher risk for long-term mortality after EUS-guided drainage [18]. Interestingly, the study found that this was independent from the clinical success rate for the procedure. Moreover, an Italian nationwide study of 116 patients found that despite a relatively high clinical success (87.1%) and low rate of AEs (10%), 30-day mortality was 19.8% (21/106) and the overall mortality rate during follow-up was 36.8% (39/106) [19]. The authors reported that most patients died due to underlying comorbidities including advanced malignancies, heart failure, renal and liver impairments. The aforementioned studies underscore the importance of accounting for patient comorbidities prior to procedure planning as well as the consent process.
Patient selection for ERCP-guided gallbladder drainage should consider comorbidities, risk of readmission, anesthesia tolerance, and potential for future cholecystectomy. Our findings of lower 30-day readmission rates and reduced AEs with ERCP-guided drainage suggest that patients at higher risk for readmission or recurrent cholecystitis, in particular, may benefit from this approach. Although those unable to tolerate general anesthesia might still require PTC under local anesthesia, ERCP-guided drainage offers potential advantages for subsequent surgical management.
Furthermore, literature indicates that endoscopic drainage techniques can lead to faster resolution of cholecystitis [20]. This may facilitate easier gallbladder dissection during future cholecystectomy, potentially reducing operative time and lowering risk of conversion to open surgery [20] [21]. Implementation of ERCP-guided drainage requires a multidisciplinary approach and clinical providers should be aware of the learning curve associated with this technique [22]. Because our study demonstrates the benefits of ERCP-guided drainage in terms of reduced readmissions and complications, these additional surgical considerations further support its potential advantages in comprehensive patient care for acute cholecystitis.
Our study has several limitations inherent in its retrospective design and use of the NRD, which may impact interpretation of our main findings in several important ways. First, reliance on ICD-10 codes for identifying procedures and outcomes may lead to misclassification bias. Accuracy of coding can vary between institutions and may not capture the full clinical picture or procedure details, potentially leading to under-estimation or over-estimation of procedure rates and outcomes. This could affect the reported differences between ERCP-guided drainage and PTC. Second, the NRD lacks granular clinical data such as laboratory values, imaging findings, and severity scores for acute cholecystitis. This limitation means we cannot fully account for disease severity, which could confound the relationship between procedure choice and outcomes. Furthermore, such population-level studies do not account for multiple, repeat, or failed attempts at cannulating the cystic duct or concomitantly treating bile duct stones.
Patients with more severe cases might be more likely to undergo PTC, potentially biasing the results against this procedure. Third, we cannot account for operator experience or institutional expertise, which may significantly influence outcomes of endoscopic procedures. Finally, the reasons for choosing one procedure over another are not captured in the database, potentially introducing selection bias. However, despite these shortcomings, we used propensity scoring to a very large population-level database to provide estimates lacking in the current literature.
Conclusions
In conclusion, this nationwide cohort study demonstrates that ERCP-guided gallbladder drainage is associated with significantly better outcomes compared with PTC in patients with acute cholecystitis. Key findings include lower 30-day readmission rates, lower index admission mortality, and fewer inpatient AEs with ERCP-guided drainage. The study also reveals a lower rate of readmission for recurrent acute cholecystitis in the ERCP-guided group. These results suggest that ERCP-guided drainage may be a superior alternative for managing acute cholecystitis in patients who are not surgical candidates.
Conflict of Interest
The authors declare that they have no conflict of interest.
-
References
- 1
Yokoe M,
Takada T,
Strasberg SM.
et al.
TG13 diagnostic criteria and severity grading of acute cholecystitis (with videos).
J Hepatobiliary Pancreat Sci 2013; 20: 35-46
MissingFormLabel
- 2
Kedia P,
Sharaiha RZ,
Kumta NA.
et al.
Endoscopic gallbladder drainage compared with percutaneous drainage. Gastrointest
Endosc 2015; 82: 1031-1036
MissingFormLabel
- 3
Cirocchi R,
Cozza V,
Sapienza P.
et al.
Percutaneous cholecystostomy as bridge to surgery vs surgery in unfit patients with
acute calculous cholecystitis: A systematic review and meta-analysis. Surgeon 2023;
21: e201-e223
MissingFormLabel
- 4
Boregowda U,
Umapathy C,
Nanjappa A.
et al.
Endoscopic ultrasound guided gallbladder drainage – is it ready for prime
time?. World J Gastrointest Pharmacol Ther 2018; 9: 47-54
MissingFormLabel
- 5
Itoi T,
Coelho-Prabhu N,
Baron TH.
Endoscopic gallbladder drainage for management of acute cholecystitis. Gastrointestl
Endosc 2010; 71: 1038-1045
MissingFormLabel
- 6
Jang JW,
Lee SS,
Song TJ.
et al.
Endoscopic ultrasound-guided transmural and percutaneous transhepatic gallbladder
drainage are comparable for acute cholecystitis. Gastroenterology 2012; 142: 805-811
MissingFormLabel
- 7
Teoh A,
Serna C,
Penas I.
et al.
Endoscopic ultrasound-guided gallbladder drainage reduces adverse events compared
with percutaneous cholecystostomy in patients who are unfit for cholecystectomy. Endoscopy
2016; 49: 130-138
MissingFormLabel
- 8
Siddiqui A,
Kunda R,
Tyberg A.
et al.
Three-way comparative study of endoscopic ultrasound-guided transmural gallbladder
drainage using lumen-apposing metal stents versus endoscopic transpapillary drainage
versus percutaneous cholecystostomy for gallbladder drainage in high-risk surgical
patients with acute cholecystitis: Clinical outcomes and success in an international,
multicenter study. Surg Endosc 2019; 33: 1260-1270
MissingFormLabel
- 9
Tyberg A,
Saumoy M,
Sequeiros EV.
et al.
EUS-guided versus percutaneous gallbladder drainage: Isn’t it time to convert?. J
Clin Gastroenterol 2018; 52: 79-84
MissingFormLabel
- 10
Chaar A,
Zamora-Sifuentes J,
Nasser A.
et al.
Tu1129 EUS-guided versus percutaneous gallbladder drainage in patients who are unfit
for cholecystectomy: a community hospital setting. Gastrointest Endosc 2019; 89: AB571
MissingFormLabel
- 11
Teoh AYB,
Kitano M,
Itoi T.
et al.
Endosonography-guided gallbladder drainage versus percutaneous cholecystostomy in
very high-risk surgical patients with acute cholecystitis: an international randomised
multicentre controlled superiority trial (DRAC 1). Gut 2020; 69: 1085-1091
MissingFormLabel
- 12
Saumoy M,
Tyberg A,
Brown E.
et al.
Successful Cholecystectomy after endoscopic ultrasound gallbladder drainage compared
with percutaneous cholecystostomy, Can it be done?. J Clin Gastroenterol 2019; 53:
231-235
MissingFormLabel
- 13
Chou CK,
Lee KC,
Chan CC.
et al.
Early percutaneous cholecystostomy in severe acute cholecystitis reduces the complication
rate and duration of hospital stay. Medicine 2015; 94: e1096
MissingFormLabel
- 14
Gosain S,
Bonatti H,
Smith L.
et al.
Gallbladder stent placement for prevention of cholecystitis in patients receiving
covered metal stent for malignant obstructive jaundice: A feasibility study. Dig Dis
Sci 2010; 55: 2406-2411
MissingFormLabel
- 15
Khan MA,
Atiq O,
Kubiliun N.
et al.
Efficacy and safety of endoscopic gallbladder drainage in acute cholecystitis: Is
it better than percutaneous gallbladder drainage?. Gastrointest Endosc 2017; 85: 76-87
e3
MissingFormLabel
- 16
Sanjay P,
Mittapalli D,
Marioud A.
et al.
Clinical outcomes of a percutaneous cholecystostomy for acute cholecystitis: a multicentre
analysis. HPB (Oxford) 2013; 15: 511-516
MissingFormLabel
- 17
Hsieh M,
Shih H,
Hsu W.
et al.
Percutaneous transhepatic gallbladder drainage facilitates endoscopic transpapillary
gallbladder drainage in patients with acute cholecystitis. Adv Dig Med 2022; 9: 161-167
MissingFormLabel
- 18
Lisotti A,
Linguerri R,
Bacchilega I.
et al.
EUS-guided gallbladder drainage in high-risk surgical patients with acute cholecystitis-procedure
outcomes and evaluation of mortality predictors. Surg Endosc 2022; 36: 569-578
MissingFormLabel
- 19
Binda C,
Anderloni A,
Forti E.
et al.
EUS-guided gallbladder drainage using a lumen-apposing metal stent for acute cholecystitis:
Results of a nationwide study with long-term follow-up. diagnostics 2024; 14: 413
MissingFormLabel
- 20
Kaura K,
Bazerbachi F,
Sawas T.
et al.
Surgical outcomes of ERCP-guided transpapillary gallbladder drainage versus percutaneous
cholecystostomy as bridging therapies for acute cholecystitis followed by interval
cholecystectomy. HPB (Oxford) 2020; 22: 996-1003
MissingFormLabel
- 21
Yuste RT,
García-Alonso FJ,
Sánchez-Ocana R.
et al.
Safety and clinical outcomes of endoscopic ultrasound-guided gallbladder drainage
with lumen-apposing metal stents in patients with dwell time over one year. Ann Gastroenterol
2019; 32: 514-521
MissingFormLabel
- 22
Tyberg A,
Jha K,
Shah S.
et al.
EUS-guided gallbladder drainage: a learning curve modified by technical progress.
Endosc Int Open 2020; 8: E92-E96
MissingFormLabel
Correspondence
Publication History
Received: 17 October 2024
Accepted after revision: 15 January 2025
Accepted Manuscript online:
20 January 2025
Article published online:
26 February 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
Chun-wei Pan, Daryl Ramai, Azizullah Beran, Yichen Wang, Yuting Huang, John Morris. Endoscopic transpapillary gallbladder stenting vs percutaneous cholecystostomy for managing acute cholecystitis: Nationwide propensity score study. Endosc Int Open 2025; 13: a25210084.
DOI: 10.1055/a-2521-0084
-
References
- 1
Yokoe M,
Takada T,
Strasberg SM.
et al.
TG13 diagnostic criteria and severity grading of acute cholecystitis (with videos).
J Hepatobiliary Pancreat Sci 2013; 20: 35-46
MissingFormLabel
- 2
Kedia P,
Sharaiha RZ,
Kumta NA.
et al.
Endoscopic gallbladder drainage compared with percutaneous drainage. Gastrointest
Endosc 2015; 82: 1031-1036
MissingFormLabel
- 3
Cirocchi R,
Cozza V,
Sapienza P.
et al.
Percutaneous cholecystostomy as bridge to surgery vs surgery in unfit patients with
acute calculous cholecystitis: A systematic review and meta-analysis. Surgeon 2023;
21: e201-e223
MissingFormLabel
- 4
Boregowda U,
Umapathy C,
Nanjappa A.
et al.
Endoscopic ultrasound guided gallbladder drainage – is it ready for prime
time?. World J Gastrointest Pharmacol Ther 2018; 9: 47-54
MissingFormLabel
- 5
Itoi T,
Coelho-Prabhu N,
Baron TH.
Endoscopic gallbladder drainage for management of acute cholecystitis. Gastrointestl
Endosc 2010; 71: 1038-1045
MissingFormLabel
- 6
Jang JW,
Lee SS,
Song TJ.
et al.
Endoscopic ultrasound-guided transmural and percutaneous transhepatic gallbladder
drainage are comparable for acute cholecystitis. Gastroenterology 2012; 142: 805-811
MissingFormLabel
- 7
Teoh A,
Serna C,
Penas I.
et al.
Endoscopic ultrasound-guided gallbladder drainage reduces adverse events compared
with percutaneous cholecystostomy in patients who are unfit for cholecystectomy. Endoscopy
2016; 49: 130-138
MissingFormLabel
- 8
Siddiqui A,
Kunda R,
Tyberg A.
et al.
Three-way comparative study of endoscopic ultrasound-guided transmural gallbladder
drainage using lumen-apposing metal stents versus endoscopic transpapillary drainage
versus percutaneous cholecystostomy for gallbladder drainage in high-risk surgical
patients with acute cholecystitis: Clinical outcomes and success in an international,
multicenter study. Surg Endosc 2019; 33: 1260-1270
MissingFormLabel
- 9
Tyberg A,
Saumoy M,
Sequeiros EV.
et al.
EUS-guided versus percutaneous gallbladder drainage: Isn’t it time to convert?. J
Clin Gastroenterol 2018; 52: 79-84
MissingFormLabel
- 10
Chaar A,
Zamora-Sifuentes J,
Nasser A.
et al.
Tu1129 EUS-guided versus percutaneous gallbladder drainage in patients who are unfit
for cholecystectomy: a community hospital setting. Gastrointest Endosc 2019; 89: AB571
MissingFormLabel
- 11
Teoh AYB,
Kitano M,
Itoi T.
et al.
Endosonography-guided gallbladder drainage versus percutaneous cholecystostomy in
very high-risk surgical patients with acute cholecystitis: an international randomised
multicentre controlled superiority trial (DRAC 1). Gut 2020; 69: 1085-1091
MissingFormLabel
- 12
Saumoy M,
Tyberg A,
Brown E.
et al.
Successful Cholecystectomy after endoscopic ultrasound gallbladder drainage compared
with percutaneous cholecystostomy, Can it be done?. J Clin Gastroenterol 2019; 53:
231-235
MissingFormLabel
- 13
Chou CK,
Lee KC,
Chan CC.
et al.
Early percutaneous cholecystostomy in severe acute cholecystitis reduces the complication
rate and duration of hospital stay. Medicine 2015; 94: e1096
MissingFormLabel
- 14
Gosain S,
Bonatti H,
Smith L.
et al.
Gallbladder stent placement for prevention of cholecystitis in patients receiving
covered metal stent for malignant obstructive jaundice: A feasibility study. Dig Dis
Sci 2010; 55: 2406-2411
MissingFormLabel
- 15
Khan MA,
Atiq O,
Kubiliun N.
et al.
Efficacy and safety of endoscopic gallbladder drainage in acute cholecystitis: Is
it better than percutaneous gallbladder drainage?. Gastrointest Endosc 2017; 85: 76-87
e3
MissingFormLabel
- 16
Sanjay P,
Mittapalli D,
Marioud A.
et al.
Clinical outcomes of a percutaneous cholecystostomy for acute cholecystitis: a multicentre
analysis. HPB (Oxford) 2013; 15: 511-516
MissingFormLabel
- 17
Hsieh M,
Shih H,
Hsu W.
et al.
Percutaneous transhepatic gallbladder drainage facilitates endoscopic transpapillary
gallbladder drainage in patients with acute cholecystitis. Adv Dig Med 2022; 9: 161-167
MissingFormLabel
- 18
Lisotti A,
Linguerri R,
Bacchilega I.
et al.
EUS-guided gallbladder drainage in high-risk surgical patients with acute cholecystitis-procedure
outcomes and evaluation of mortality predictors. Surg Endosc 2022; 36: 569-578
MissingFormLabel
- 19
Binda C,
Anderloni A,
Forti E.
et al.
EUS-guided gallbladder drainage using a lumen-apposing metal stent for acute cholecystitis:
Results of a nationwide study with long-term follow-up. diagnostics 2024; 14: 413
MissingFormLabel
- 20
Kaura K,
Bazerbachi F,
Sawas T.
et al.
Surgical outcomes of ERCP-guided transpapillary gallbladder drainage versus percutaneous
cholecystostomy as bridging therapies for acute cholecystitis followed by interval
cholecystectomy. HPB (Oxford) 2020; 22: 996-1003
MissingFormLabel
- 21
Yuste RT,
García-Alonso FJ,
Sánchez-Ocana R.
et al.
Safety and clinical outcomes of endoscopic ultrasound-guided gallbladder drainage
with lumen-apposing metal stents in patients with dwell time over one year. Ann Gastroenterol
2019; 32: 514-521
MissingFormLabel
- 22
Tyberg A,
Jha K,
Shah S.
et al.
EUS-guided gallbladder drainage: a learning curve modified by technical progress.
Endosc Int Open 2020; 8: E92-E96
MissingFormLabel