

Subscribe to RSS
DOI: 10.1055/a-2760-9552
Side-by-side 6-mm multi-hole metal stents more effective than inside plastic stents for reintervention after stent-in-stent placement in malignant hilar biliary obstruction
Authors

Endoscopic reintervention after the stent-in-stent (SIS) placement of self-expandable metallic stents (SEMSs) for unresectable malignant hilar biliary obstruction (MHBO) is challenging [1]. Regarding revisionary stenting, SEMSs have a longer patency than plastic stents (PSs [2]), but advances in chemotherapy have increased the need for reinterventions, often using removable PSs. Additional uncovered SEMSs (UCSEMSs) can complicate future reinterventions and cannot be removed, limiting endoscopic options. We report a case of MHBO in which the side-by-side placement of the 6 mm multi-hole SEMS (MHSEMS) was effective for reintervention compared with multiple PSs after SIS.
An 84-year-old woman with MHBO, previously treated with the MHSEMS and UCSEMS in SIS placement followed by two PSs, was admitted with cholangitis ([Fig. 1]). She had experienced repeated stent occlusion over a short period, so we opted to place two removable SEMSs ([Video 1]). A guidewire (GW) was placed into the left intrahepatic bile duct (IHBD), and both PSs were removed. Another GW was placed into the right IHBD, and two 6 mm MHSEMSs with a slim delivery system were inserted. Insertion into the deep left IHBD was somewhat difficult, so the stents were inserted one by one but deployed simultaneously across the papilla ([Fig. 2]). No adverse events occurred, and the outcome was favorable.

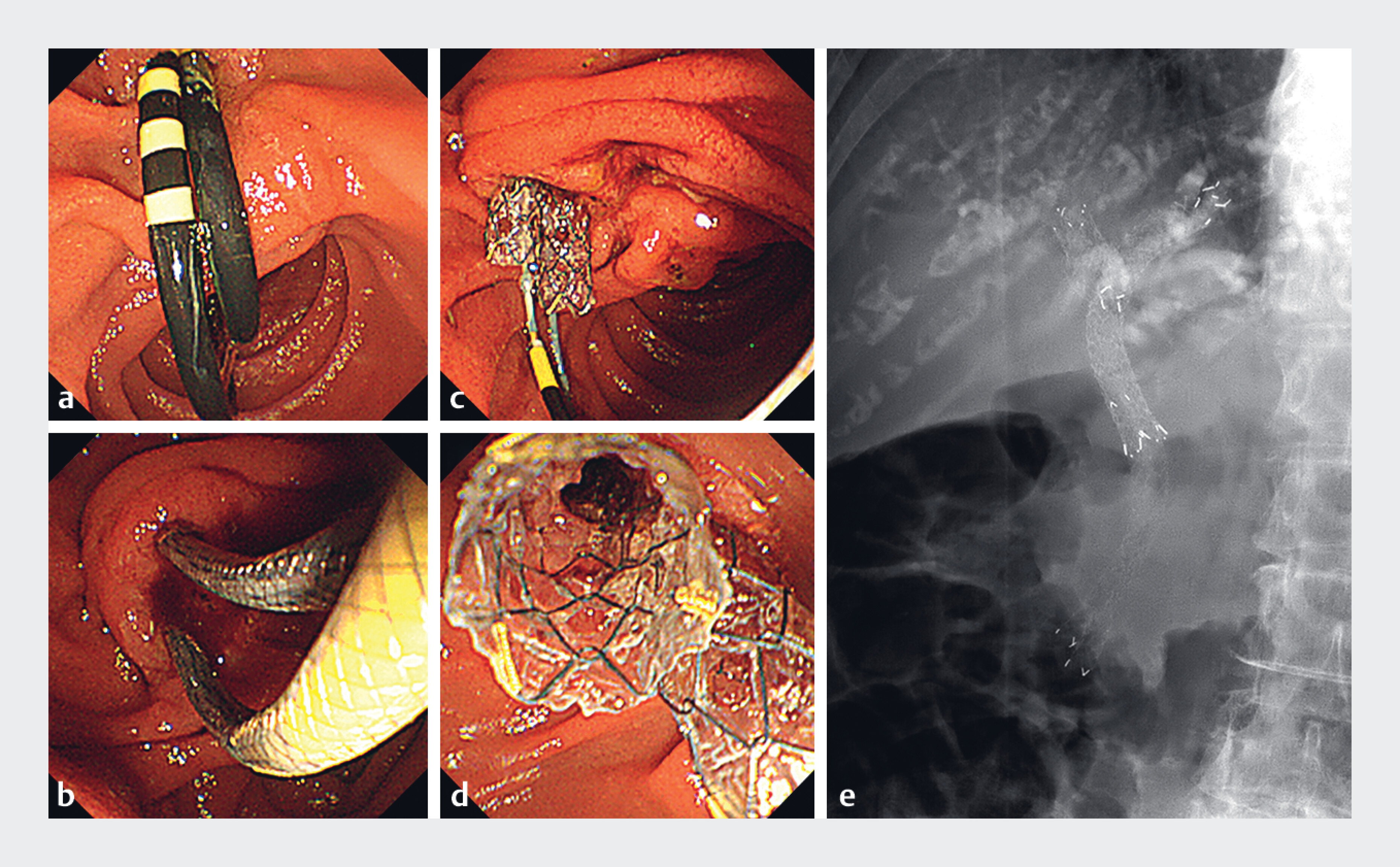
The advantages of the MHSEMS have no step between the delivery system and the stent and it has an outer diameter of 5.9 Fr. In this case, placement of a 7 Fr PS was difficult and time-consuming due to interference from the existing SEMS; however, the MHSEMS could be placed in a much shorter time. Furthermore, after deployment, the inner diameter is larger than that of a PS, and the two MHSEMSs share each other’s holes, providing a drainage effect equivalent to more than 6 mm. The MHSEMS is also removable [3], making it a favorable option for reintervention.
Endoscopy_UCTN_Code_TTT_1AR_2AZ
Contributorsʼ Statement
Hirotsugu Maruyama: Conceptualization, Writing – original draft. Kojiro Tanoue: Writing – review & editing. Yuji Kawata: Writing – review & editing. Tatsuya Kurokawa: Writing – review & editing. Yoshinori Shimamoto: Writing – review & editing. Yuki Ishikawa-Kakiya: Writing – review & editing. Yasuhiro Fujiwara: Writing – review & editing.
Conflict of Interest
The authors declare that they have no conflict of interest.
-
References
- 1 Guilmoteau T, Rouquette O, Buisson A. et al. Direct comparison of simultaneous and sequential endoscopic metallic bilateral stenting in malignant hilar biliary obstruction. World J Gastroenterol 2025; 31: 101913
- 2 Inoue T, Naitoh I, Okumura F. et al. Reintervention for stent occlusion after bilateral self-expandable metallic stent placement for malignant hilar biliary obstruction. Dig Endosc 2016; 28: 731-737
- 3 Maruyama H, Ishikawa-Kakiya Y, Kawata Y. et al. Stent-in-stent deployment across the papilla for malignant hilar biliary obstruction using novel slim multi-hole metal stents. Endosc Int Open 2025; 13: a27142453
Correspondence
Publication History
Article published online:
08 January 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Guilmoteau T, Rouquette O, Buisson A. et al. Direct comparison of simultaneous and sequential endoscopic metallic bilateral stenting in malignant hilar biliary obstruction. World J Gastroenterol 2025; 31: 101913
- 2 Inoue T, Naitoh I, Okumura F. et al. Reintervention for stent occlusion after bilateral self-expandable metallic stent placement for malignant hilar biliary obstruction. Dig Endosc 2016; 28: 731-737
- 3 Maruyama H, Ishikawa-Kakiya Y, Kawata Y. et al. Stent-in-stent deployment across the papilla for malignant hilar biliary obstruction using novel slim multi-hole metal stents. Endosc Int Open 2025; 13: a27142453