

Subscribe to RSS
DOI: 10.1055/a-2761-0266
Cholangioscopy-guided laser lithotripsy alongside a plastic stent for common bile duct stones after total gastrectomy
Authors

Peroral cholangioscopy (POCS)-guided lithotripsy in patients with surgically altered anatomy is challenging [1] [2]. Recently, a novel slim cholangioscope (9-Fr eyeMAX; Micro-Tech, Nanjing, China) has been developed that facilitates POCS-guided lithotripsy under balloon-enteroscopy assisted endoscopic retrograde cholangiopancreatography (BE-ERCP [3] [4]). However, the maneuverability of the cholangioscope is limited when the common bile duct is highly angulated. In such cases, inserting the cholangioscope alongside a plastic stent (PS) can improve maneuverability ([Fig. 1]). In addition, the PS allows excess saline to flow out of the bile duct, thereby preventing cholangitis. Herein, we report a successful case of POCS-guided laser lithotripsy performed alongside a PS in a patient with common bile duct stones after total gastrectomy ([Video 1]).

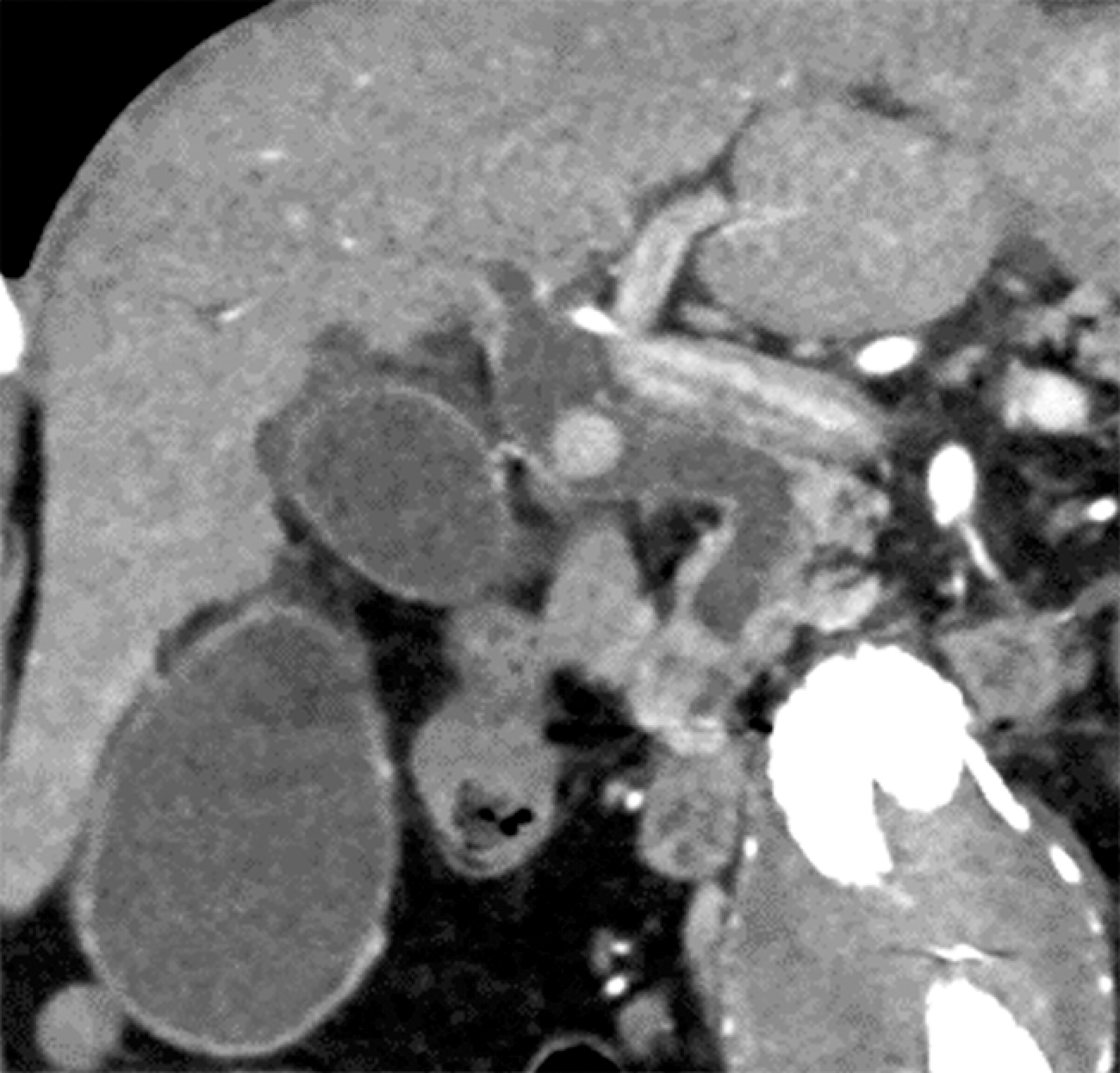
An 82-year-old man who had undergone total gastrectomy with Roux-en-Y reconstruction was referred to our hospital with cholangitis caused by large common bile duct stones ([Fig. 2]). First, BE-ERCP was performed for biliary drainage. The bile duct was highly angulated, and a double pigtail PS (7-Fr, 12 cm REGULUS double pigtail; Japan Lifeline, Co., Ltd, Tokyo, Japan) was placed with its proximal end anchored in the intrahepatic bile duct ([Fig. 3]). Six days later, POCS-guided lithotripsy was performed ([Fig. 4]). Cholangiography demonstrated that the bile duct was straightened. Subsequently, the 9-Fr eyeMAX cholangioscope was inserted alongside the PS and advanced easily to the perihilar bile duct. Laser lithotripsy was successfully performed using a holmium-YAG laser system (LithoEVO; Edap TMS, Lyon, France). After lithotripsy, the stent was removed, and stone extraction was performed using a basket catheter. Because the bile duct remained angulated, the 9-Fr eyeMAX cholangioscope was reinserted with difficulty. A residual stone was removed using a micro-basket catheter under cholangioscopy guidance. The patient was discharged without complications.


To the best of our knowledge, this is the first report of POCS-guided lithotripsy performed alongside a PS, which improves the maneuverability of the cholangioscope.
Endoscopy_UCTN_Code_TTT_1AR_2AH
Contributorsʼ Statement
Ryo Soma: Conceptualization, Formal analysis, Visualization, Writing – original draft. Haruo Miwa: Conceptualization, Supervision. Kazuki Endo: Supervision. Ritsuko Oishi: Supervision. Yuichi Suzuki: Supervision. Hiromi Tsuchiya: Supervision. Shin Maeda: Supervision.
Conflict of Interest
The authors declare that they have no conflict of interest.
Acknowledgement
The authors thank the endoscopy unit staff at Yokohama City University Medical Center for their assistance during the procedure. The authors declare that no external funding was received for this study.
-
References
- 1 Hakuta R, Kogure H, Nakai Y. et al. Successful endoscopic lithotripsy using a new digital cholangioscope through an overtube placed by an enteroscope. Endoscopy 2018; 50: E269-E271
- 2 Tonozuka R, Itoi T, Sofuni A. et al. Novel peroral direct digital cholangioscopy-assisted lithotripsy using a monorail technique through the overtube in patients with surgically altered anatomy. Dig Endosc 2019; 31: 203-208
- 3 Kao KT, Batra B. Single-balloon-assisted ERCP with electrohydraulic lithotripsy for the treatment of a bile duct stone in a patient with a hepaticojejunostomy. Gastrointest Endosc 2014; 80: 1173
- 4 Sato T, Kogure H, Nakai Y. et al. Electrohydraulic lithotripsy under double-balloon endoscope-assisted direct cholangioscopy for treatment of choledocholithiasis in a patient with Roux-en-Y gastrectomy. VideoGIE 2018; 3: 113-114
Correspondence
Publication History
Article published online:
15 January 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Hakuta R, Kogure H, Nakai Y. et al. Successful endoscopic lithotripsy using a new digital cholangioscope through an overtube placed by an enteroscope. Endoscopy 2018; 50: E269-E271
- 2 Tonozuka R, Itoi T, Sofuni A. et al. Novel peroral direct digital cholangioscopy-assisted lithotripsy using a monorail technique through the overtube in patients with surgically altered anatomy. Dig Endosc 2019; 31: 203-208
- 3 Kao KT, Batra B. Single-balloon-assisted ERCP with electrohydraulic lithotripsy for the treatment of a bile duct stone in a patient with a hepaticojejunostomy. Gastrointest Endosc 2014; 80: 1173
- 4 Sato T, Kogure H, Nakai Y. et al. Electrohydraulic lithotripsy under double-balloon endoscope-assisted direct cholangioscopy for treatment of choledocholithiasis in a patient with Roux-en-Y gastrectomy. VideoGIE 2018; 3: 113-114