
Subscribe to RSS
DOI: 10.1055/s-0033-1344418
Cholecysto-duodenal fistula as the source of upper gastrointestinal bleeding
Corresponding author
Publication History
Publication Date:
05 September 2013 (online)

A 44-year-old woman was admitted with recurrent hematemesis. She had a history of intermittent upper abdominal pain, which was investigated by computed tomography (CT) scan 1 year prior to the presentation ([Fig. 1]). She was taking aspirin for ischemic heart disease.

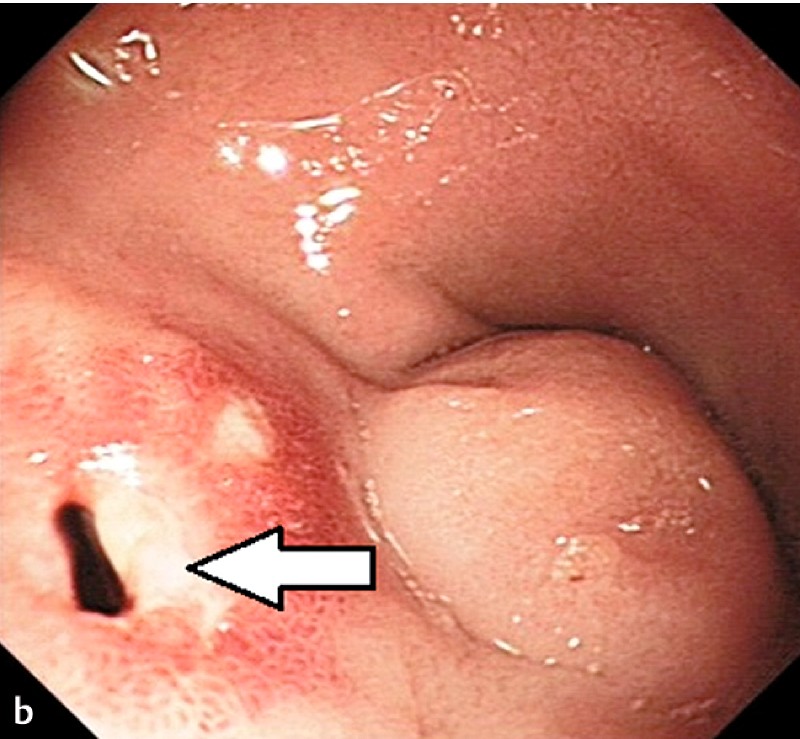
On examination, her heart rate was 110 bpm and she had postural hypotension. She was febrile (38.7 °C) and had epigastric tenderness. Blood results were abnormal: white blood cells 17.0 × 103 cells/μL, C-reactive protein 136 mg/L, and alkaline phosphatase 515 IU/L (normal range 70 – 300 IU/L). Glasgow–Blatchford and Rockall scores were elevated at 11 and 8, respectively. Findings at gastrointestinal endoscopy and CT scan are shown in [Fig. 2] and [Fig. 3].


Biliary-enteric fistula (BEF) is a rare cause of upper gastrointestinal bleeding. Cholecysto-duodenal fistula (CDF) is the commonest type of BEF [1]. The common causes of CDF include gallstones, peptic ulcer disease, malignancy, and trauma/surgery. Definitive management is cholecystectomy, resection of the fistula, and intraoperative cholangiography. Diagnosis is made by CT, endoscopic retrograde cholangiopancreatography, or laparoscopic cholecystectomy [2]. Proximal CDFs located in the posterior wall of the duodenal bulb are usually secondary to peptic ulcer disease whereas distal CDFs, which are located in the periampullary region, connect to the distal 2 cm of the bile duct and are more commonly associated with biliary stones [3].
Our patient had symptoms of biliary colic and had gallbladder calculi on initial CT scan. She had recurrent hematemesis during episodes of cholangitis. She was treated conservatively with antibiotics and underwent successful elective open cholecystectomy with repair of the CDF.
BEFs involving the duodenal bulb secondary to cholelithiasis are uncommon. CT allows visualization of the fistulas, air in the bile duct, and contraction of the gallbladder, and differentiates between cholecysto-enteric and choledocho-enteric fistulas [4]. We believe that this case highlights the importance of CT imaging in patients with upper gastrointestinal bleeding and unusual endoscopic findings.
Endoscopy_UCTN_Code_CCL_1AB_2AZ_3AZ
#
Competing interests: None
-
References
- 1 Glenn F, Reed C, Grafe WR. Biliary enteric fistula. Surg Gynecol Obstet 1981; 153: 527-531
- 2 Leung E, Kumar P. Bilo-enteric fistula (BEF) at laparoscopic cholecystectomy: review of ten year’s experience. Surgeon 2010; 8: 67-70
- 3 Stagnitti F, Mongardini M, Schillaci F et al. [Spontaneous biliodigestive fistulae. The clinical considerations, surgical treatment and complications.] [Article in Italian]. G Chir 2000; 21: 110-117
- 4 Shimono T, Nishimura K, Hayakawa K. CT imaging of biliary enteric fistula. Abdom Imaging 1998; 23: 172-176
Corresponding author
-
References
- 1 Glenn F, Reed C, Grafe WR. Biliary enteric fistula. Surg Gynecol Obstet 1981; 153: 527-531
- 2 Leung E, Kumar P. Bilo-enteric fistula (BEF) at laparoscopic cholecystectomy: review of ten year’s experience. Surgeon 2010; 8: 67-70
- 3 Stagnitti F, Mongardini M, Schillaci F et al. [Spontaneous biliodigestive fistulae. The clinical considerations, surgical treatment and complications.] [Article in Italian]. G Chir 2000; 21: 110-117
- 4 Shimono T, Nishimura K, Hayakawa K. CT imaging of biliary enteric fistula. Abdom Imaging 1998; 23: 172-176