

RSS-Feed abonnieren
DOI: 10.1055/s-0035-1564422
The Role of the Intraoperative Auxiliary Methods in the Resection of Motor Area Lesions
O papel dos métodos auxiliares intraoperatórios na ressecção de lesões em área motoraAutor*innen
Address for correspondence
Publikationsverlauf
30. März 2015
07. August 2015
Publikationsdatum:
28. Oktober 2015 (online)


Abstract
Objective In recent years, technologies have advanced considerably in improving surgical outcome following treatment of lesions in eloquent brain areas. The aim of this study is to explore which method is best in the resection of motor area lesions.
Methods Prospective, non-randomized study Evaluate on 74 patients who underwent surgery to remove lesions around the motor area.
Results Total lesion removal was achieved in 68 patients (93.1%). Fifty-four patients (73.9%) presented normal motor function in the preoperative period; of these, 20 (37.3%) developed transitory deficits. Nevertheless, 85% of these patients later experienced a complete recovery. Nineteen patients presented with motor deficits preoperatively; of these, five presented deteriorating motor abilities. Intraoperative stimulation methods were used in 65% of the patients, primarily in cases of glioma.
Conclusions The morbidity in patients submitted to resections of motor area lesions is acceptable and justify the surgical indication with the purpose of maximal resection. Intraoperative stimulation is an important tool that guides glioma resection in many cases.
Resumo
Objetivo Nos últimos anos, consideráveis avanços tecnológicos têm surgido no sentido de melhorar os resultados cirúrgicos no tratamento de lesões em áreas eloquentes do cérebro. O objetivo deste estudo é investigar qual o melhor método para ressecção de lesões em área motora.
Método Estudo prospectivo não aleatório que avaliou os resultados pós-operatórios em 74 pacientes submetidos à ressecção de lesões em área motora ou adjacente.
Resultados A ressecção cirúrgica foi considerada total em 68 (93,1%) pacientes. 54 pacientes (73,9%) apresentavam força muscular normal no pré-operatório. Destes, 20 (37,3%) apresentaram déficit no pós-operatório imediato, sendo que 17 (85%) recuperaram completamente o déficit. 19 pacientes apresentavam déficit no pré-operatório, sendo que 05 apresentaram piora do déficit no pós-operatório imediato. A estimulação intraoperatória foi utilizada em 65% dos casos, principalmente nos gliomas.
Conclusão A morbidade em pacientes operados de lesões em área motora é bastante aceitável e justifica a indicação cirúrgica com objetivo de ressecção máxima. A estimulação intraoperatória é uma ferramenta importante para guiar a resseção dos gliomas em muitos casos.
Introduction
The resection of brain lesions situated in or adjacent to the motor cortex is still a challenge in modern neurosurgery. Technological advances have allowed for a more precise localization of eloquent brain areas, including the motor and language cortex, minimizing the risk of neurological deficits in the postoperative period.
There are a large number of reports supporting the use, isolated or not, of cortical stimulation, functional magnetic resonance (fMRI), motor evoked potentials, neuronavigation systems, and other techniques of defining the precise functional resection of lesions located in eloquent motor areas.[1] [2] [3] [4] [5] [6] [7] [8] In addition to the preservation of cerebral function during surgery, these techniques also offer optimization of resection limits, which helps in achieving removal of lesion or epileptic focus to a greater extent and with increased safety.[9] [10] [11] Despite increased use of such techniques, the anatomical knowledge and the use of precise neurosurgical techniques still play a decisive role in the attempt to preserve the full integrity of vascular structures and decrease the risk of functional deficits.[12] [13] [14] [15]
The aim of this study was to explore which of the above-mentioned methods is best in the resection of motor area lesions. We also investigated the relationship between methods used and the development of postoperative motor deficits. Furthermore, we attempted to identify cases that only required knowledge of microanatomy and neuroimaging analyses for safe resection of lesions in the motor cortex.
Material and Methods
Patient Population
We conducted a prospective, non-randomized study on 74 patients who underwent surgery to remove lesions around the motor cortex and in the insular lobe that presented a close relationship with subcortical motor structures. All surgeries occurred between January 2002 and 2009 by the same neurosurgeon, after obtaining written informed consent from each patient. We excluded from this study patients with a Karnofsky score lower than 70 and subject to reoperation. We preoperatively evaluated the topographic relationship between the lesion and the motor area in all patients by computerized tomography (CT) and magnetic resonance imaging (MRI). MRI was performed, and the anatomical relation between the brain lesion and the central lobe was identified using images of coronal, axial, and sagittal planes. Following intravenous administration of gadolin, the T1-weighted sequence permitted the identification of the relationship between the lesion location and the central sulcus and cortical vessels. We investigated demographic, clinical, CT, or MRI images, and treatment data, which included the following: operative intervention, lesion location and depth, histological diagnosis, extent of lesion excision, the presence or absence of a motor deficit either preoperatively, or early/late postoperatively. We obtained approval from the Ethics Committee and informed consent from patients or their closest relative.
Operative Techniques
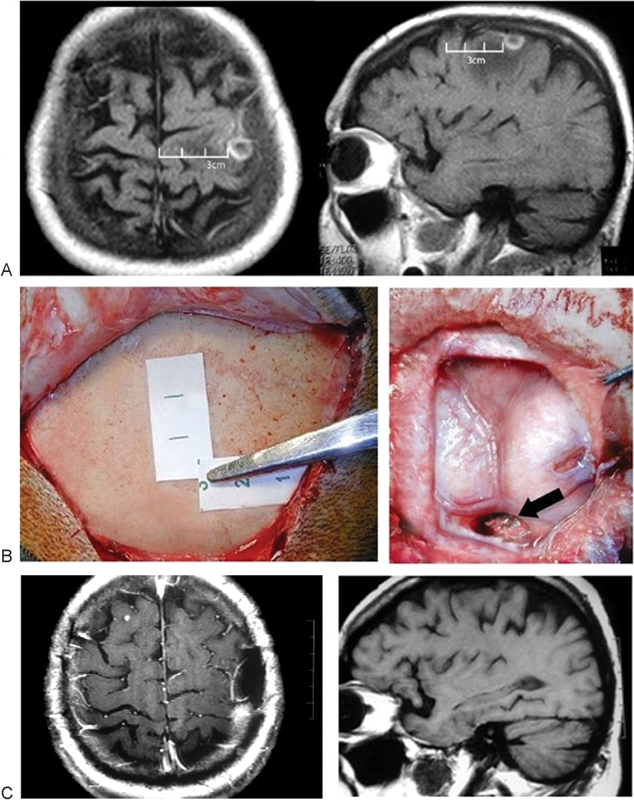
We planned craniotomy based on the topographic relationship and neuroimaging information obtained from the sutures and craniometric points. The identification of the coronal suture plays an essential role in the localization of the central sulcus and motor lobe and can be projected perfectly onto the scalp based on MRI data ([Fig. 1]). In brief, we stabilized a patient's head by a three-point fixation device (Mayfield head holder), and performed trichotomy prior to the surgical procedure only on the planned incision. For patients that required cortical stimulation, we left exposed the side of the body including the face where we expected the response. After localization of the coronal suture, we could infer the location of the central gyrus and sulcus on the skull. We used a high-speed drill to perform an initial burr hole, which we extended with a footplate to turn the craniotomy flap and expose the dura mater. We tailored the opening of the dura for each patient; however, we typically opened the dura and turned it medially to prevent damaging the sagittal sinus and/or draining the veins. Cortical stimulation was performed using a bipolar stimulator with a constant current, and a biphasic square wave (60 Hz) (Ojemann stimulator, Radionic, Burlington, MA; 5 mm between electrodes). The electrode was put in contact with the cortical surface corresponding to the anatomical location of the motor area. The current used to elicit movement ranged from 2 to 10 mA.
Postoperative Course
The same neurosurgery team conducted follow-up evaluations with all patients. They assessed and classified motor strength by using the modified Dejong Scale: no contraction (grade 1), active movement with gravity eliminated (grade 2), active movement against gravity (grade 3), active movement against resistance (grade 4), and normal strength (grade 5).
Statistical Analysis
We analyzed factors that correlated histological diagnosis and motor strength during early and late postoperative periods. We used the Friedman test and Student's t-test; p values < 0.05 were statistically significant. Due to the limited number of patients, the data available was insufficient; therefore, multivariate analysis was not possible.
Results
This is a prospective study to evaluate the postoperative surgical outcome in patients who underwent surgery to remove lesions around the motor area. The study included a total of 74 patients analyzed between January 2002 and 2009. All patients presented with lesions around the motor area or immediately adjacent to it, and were underwent a surgical procedure in accordance with a previously defined protocol. Morbidity and the presence or absence of a preoperative and early and/or later postoperative motor deficit was also evaluated. Because of the limited number of patients, the wide-range of histological variation, and the multiple variables analyzed, the overall survival rate was not a goal of this study.
[Table 1] summarizes clinical and surgical characteristics of the 74 patients. This group was composed of 31 (48.1%) male patients and 43 (56.7%) female patients with an age range of 3 to 80 years (mean 44 years). Thirty-two patients (43.2%) were diagnosed with glioma, followed by 19 patients (25.6%) with meningioma, 11 patients (14.8%) with metastasis, five patients (6.8%) with cavernoma, two patients each with primary lymphoma, cisticercus, and cortical dysplasia (2.7% in each case), and one patient with an inflammatory lesion (1.4%). Among patients with glioma, a grade IV astrocytoma was present in seven (21.8%), grade III astrocytoma was present in eight (25%), and grade II astrocytoma was present in 17 patients (53%) ([Fig. 2]).

Abbreviations: cort dysplasia, cortical dysplasia; lt, left; neuronav, neuronavigation system; oligodendro, oligodendroglioma; post op, postoperative; pre op, preoperative; rt, right; cortic stimu/cs, cortical stimulation; stereotax, stereotaxia.
Thirty-eight (51.3%) lesions were located on the left hemisphere and 35 (47.2%) on the right hemisphere. [Fig. 3] demonstrates the distribution of the lesions according to the central lobe and insula (whether the lesions were anterior, central, posterior, or paracentral in location). Thirty-eight patients harbored lesions in the anterior region of the central lobe, 17 patients in the insula, eight in the posterior part of the central lobe, seven patients in the central part of the central lobe, and in four patients in the paracentral gyrus. Compared with the lesions located in the posterior region, lesions in the anterior region presented greater impairment in motor strength (p < 0.05). Gross total lesion removal was achieved in 68 (93.1%) patients and a subtotal removal in five (6.84%).

Fifty-four patients (73.9%) presented normal motor functioning in the preoperative period. Of these, 20 (36.3%) developed transient deficits. Nevertheless, 85% of them subsequently presented a complete recovery, while three improved only partially. Nineteen patients presented preoperative motor deficits. Of these, five patients deteriorated; however, four patients subsequently improved and two recovered early in the postoperative period ([Fig. 4]). The improvement of motor strength in the late postoperative period was significant (p < 0.05).

Because of histological variation and difference in prognosis, we analyzed the data according to the category of the lesion. [Table 2] presents data describing the evaluation of motor strength according to the histological type of lesion. While comparing the evolution of motor strength in the early postoperative period between high- and low-grade gliomas, we observed a more evident deterioration in the former (p < 0.05). Muscular strength deteriorated more often in patients who had lesions in the left hemisphere than in patients with lesions in the right hemisphere (p < 0.05); however, recovery was similar between groups.
Cortical stimulation was necessary in 8 patients harboring high-grade tumors and in 13 patients who presented low-grade lesions (65% of the patients). We also used this tool in one patient with brain metastasis and in two patients with cortical dysplasia. The neuronavigation system was employed in only two patients. Finally, we performed stereotaxic surgeries in three patients with cavernomas and in one patient with neurocysticercosis ([Fig. 5]).

There were no cases of mortality among the 74 participants. Complications unrelated to motor strength occurred in four patients: one patient with a high-grade tumor had a large hematoma in the tumor bed, which we treated through surgery; two patients with cerebrospinal fistulas were treated clinically; and one patient developed a cystic formation in the tumor bed and required surgical intervention.
Discussion
The central lobe is an eloquent area of the central nervous system (CNS), surrounded anteriorly by the pre-central sulcus and posteriorly by the post-central sulcus. The central sulcus, which separates the pre- from the post-central gyrus, is one of the most important anatomical landmarks of the cerebral cortex.[16] [17]
In various situations, a neurosurgeon must take a direct approach to access cortical or subcortical lesions at the convexity or at the midline hemisphere. Although technology already offers modern intraoperative localization tools such as MRI and neuronavigation, anatomical knowledge remains an important part of surgical planning.[12] [13] [14] [15]
Craniotomy planning is an essential step in approaching motor area lesions. Paul Broca (1824–1880) was the first neurosurgeon to perform a craniotomy based on anatomical localization.[18] MRI, especially with contrast-enhanced T1 imaging, allows good visualization of the relationship between cerebral veins and lesions to be removed.[19] Radiological data and anatomical landmarks can provide a projected image of the lesion on the scalp, which influences patient position, the size and conformation of the surgical incision, and the location and extent of the craniotomy.[12] [20] [21]
Exposure of brain surface is necessary to identify the relationship between the lesion and the motor gyrus, veins, and arteries ([Fig. 6a]). The motor and sensory cortices are separated by the central sulcus, which begins at the superior border of the lateral surface and extends to the medial surface of the brain, running in an anterior-oblique direction up to around the sylvian fissure.[16] In previous anatomical studies, we verified that the distance between the coronal suture and the central sulcus ranged from 5.6 to 6.6cm in the midline, and that the coronal suture on the pterion region to the central sulcus ranged from 1.5 to 4.0cm.[13] Additionally, the coronal suture was 11.5 to 13.5cm behind the nasium. It is possible to measure these distances by using radiological images, which can then be transferred to the scalp or determined by palpation of the skull.[14] This anatomical information is useful in localizing the central lobe and craniotomy planning and dispenses non-essential use of neuronavigation. However, the use of this information during the surgical procedure can be difficult in the presence of perilesional brain edemas or in subcortical lesions. In such cases, it is important to perform functional MRI or electrophysiology.[3]

The functional localization of the motor cortex during surgery has been performed for some time and is a valuable instrument in operations performed within eloquent areas.[22] In the current study, cortical stimulation was the preferred method. This surgical approach is an easy-to-use method, which is effective and involves low cost. Cortical stimulation is available for surgical removal of tumors as well as epileptic and arteriovenous malformations, which reduces the rate of postoperative deficits and increases the degree of resection in the surgery of eloquent areas.
To obtain satisfactory cortical stimulation during surgery, a patient needs to remain awake; however, somatosensory and motor mapping can be performed while the patient is under general anesthesia.[1] [2] [23] [24] Intraoperative seizures are always a concern when using repeated stimulation of the same cortical field or using a high-stimulus setting. In our study, despite the prophylactic use of antiepileptic drugs, we had five patients that suffered partial motor seizures during cortical stimulation; however, four of these cases had a previous history of epilepsy. Therefore, we realized that the use of cortical stimulation is a safe and helpful technique for treatment of lesions involving the motor cortex because it allows the surgeon to enlarge the resection, especially in cases of gliomas.[5] [6] [25]
According to Duffau et al.,[26] Forster first used cortical stimulation in 1930, in a neurosurgery procedure. Soon after, in 1937, Penfield, who described the famous homunculus, used the technique. The operating principle of cortical stimulation is based on local neuron depolarization that induces excitation or inhibition.[26] Although cortical stimulation is technically feasible, elicitation of responses is frequently difficult in children, in patients under general anesthesia, or when stimulation is executed through the dura mater.[4] [27] In these cases, a higher current setting could possibly be required. This technique can also be used to identify descending subcortical motor fibers when resection extends below the cortical surface, such as during supplementary motor area and insular resections.[3] [28] Numerous published literature report the use of cortical stimulation alone or combined with others methods, which allows functional identification and guides surgical resection.[19] [29]
Among patients harboring high-grade gliomas, the use of cortical stimulation was necessary to identify the motor area in 65% of the patients. The criterion to use the cortical stimulator was based on the ability to correctly distinguish between normal brain tissue and tumor tissue. In other words, in 34.4% of primary malign lesions, cortical stimulation was not required because the identification and dissection of the lesion was achieved based on knowledge of anatomical parameters.
To treat subcortical lesions surrounding the motor area, both the internal capsule and corona radiata, we used the same techniques as before to avoid neurological deficits. Although the insula is not considered a part of the motor area, insular lesions close to descending motor fibers were included in this study. Recently, several authors have stressed the importance of the approach to treat lesions in the insular lobe.[17] [25] [30] Several patients in our study harbored lesions in the insular compartment and were treated surgically. In some patients, an awake craniotomy was performed, allowing us to evaluate the motor function in real time, thus, facilitating an aggressive resection of the lesion with acceptable postoperative neurologic deficits ([Fig. 6b]). When performing subcortical motor mapping, the current required to elicit movement was the same as or lower than the current needed at the cortical surface. In patients, where the resection was very close to the functional cortex, periodic repetition of the stimulation mapping procedure helped verify that the cortical and subcortical functional regions had not been damaged. In six patients, the insular lesions were resected using an awake craniotomy. In patients with subcortical or insular lesions, cortical stimulation can be used in combination with other methods such as neuronavigation; however, this was not required in the current study.
Intrinsic brain tumors may invade cortical and subcortical structures with no impairment of function, and even the grossly abnormal appearance of tissue is not an assurance that such tissue can be safely removed without risking new postoperative neurological deficits. Similar to MRI findings of some studies, we could observe motor function existing inside the tumor, generally low-grades gliomas, or on its boundaries.[31] [32] This data facilitates and guides surgical resection of the lesion. In our case, the preoperative demonstration of functional activity was not achievable, and we used cortical stimulation only to improve the quality of our surgical resection by determining the limits of the removal in eloquent areas without producing a new permanent deficit. However, it may not be possible to determine whether a new postoperative deficit is related to damage in the motor area because of surgical intervention, probable function presented in the tumor, or both.
The treatment of patients harboring a metastatic tumor was easy because, despite the aggressiveness of these tumors, they behave as an extra-axial lesion. Therefore, although several authors use an intraoperative MRI approach to these lesions, even small tumors can be thoroughly resected using careful preoperative planning.[6] [8] [33] In the current study, we used cortical stimulation in one single patient who harbored a deep metastatic tumor with an extensive brain edema. The reason why we used cortical stimulation in this patient was to choose the best place for the corticectomy.
In the patients harboring benign tumors, represented primarily by meningioma, cortical stimulation or other mapping methods were not required to guide resection of brain tumors near motor areas. Several studies in the literature describe the use of auxiliary methods to perform safe resections of these lesions[5] [25]; however, in our opinion, they are not required and increase both surgery time and surgical cost.
A neuronavigation system was used in only two patients. Its role was to verify the positioning of the craniotomy. To identify the margins of the lesion attached to adjacent structures, the use of the neuronavigation system was not of great significance, particularly because of the shift of brain structures during the procedure. According to Reithmeir et al., a more radical resection of tumors in the motor cortex area via minimal craniotomies was achieved by using neuronavigation combined with electrophysiological monitoring as compared when these methods were not available.[34] Although the literature indicates that the use of neuronavigation combined with other methods can optimize the quality of resection and decrease the risk of postoperative deficits,[35] [36] in our study, the definition of the size and craniotomy conformation was possible in all patients solely based on the knowledge of topographic anatomy of the skull.
The functional MRI is an important procedure to identify the motor area and is capable of improving surgical planning when associated to tractography. However, compared with cortical stimulation, fMRI is not a real-time mapping method.[37] [38] [39] Finally, the monitoring of motor-evoked potentials, the introaperative MRI, magnetoencephalography, and the intraoperative ultrasound imaging were not used in this study because they were not available.
Roux Fe et al. described a cortical stimulation and fMRI study involving five paretic patients with brain tumors in the motor area[6]. The authors demonstrated that patients who had motor impairment also had high activation of the supplementary motor and prefrontal areas within the ipsilateral cortex as compared with that of intact patients. In these patients, neuroplasticity may be involved in the dislocation of function; however, it is best to confirm this using other methods.[6]
In the current study, although we applied the different methods as described above in some patients, it was prudent to leave a residual lesion to avoid producing a neurological deficit that might occur due to a gross total resection.[5] [26] [40] [41] [42] Previous studies have demonstrated that the risk of new motor deficits is not greater in subsequent operations compared to the first procedure.[42] This may be a factor of a particular type of reorganization involving the motor cortex areas that render patients harboring large lesions asymptomatic.[5] [26] [43] The potential role of brain plasticity in these patients emphasizes the importance of future studies with fMRI and others methods to predict the risk of new neurological deficits after surgery and to optimize treatment planning.[43] [44] [45]
Conclusions
In this study, we demonstrated that the lack of morbidity in the surgery of lesions involving the motor area justifies the need for maximum tumor resection. The relationship between the coronal suture and the central sulcus was important in the planning of the craniotomy; however, when the central sulcus or the motor lobe was displaced due to pathological conditions, anatomical recognition was impaired. In these patients, it was important that the neurosurgeon used another tool for functional identification such as fMRI, cortical stimulation, or an awake craniotomy.
We also demonstrated that extra axial lesions such as meningioma and dural metastasis could be entirely removed with low morbidity on the basis of anatomical knowledge and appropriate microsurgical techniques, and that these cases do not require additional auxiliary methods. Thus, we can infer that cortical stimulation plays an important role in the management of infiltrative lesions and in improving quality and safety of surgical resections.
In some patients harboring subcortical lesions, an additional localization method was required to improve the cortical approach, although this may be achieved by a careful preoperative MRI analysis of the sulcus and cortical veins.
Finally, there was no difference between morbidity and resection grade when we compared our results with those using functional imaging methods, neuronavigation systems, or other methods such as intraoperative MRI during surgery around the motor area.
-
References
- 1 Berger MS, Kincaid J, Ojemann GA, Lettich E. Brain mapping techniques to maximize resection, safety, and seizure control in children with brain tumors. Neurosurgery 1989; 25 (5) 786-792
- 2 Berger MS, Ojemann GA. Intraoperative brain mapping techniques in neuro-oncology. Stereotact Funct Neurosurg 1992; 58 (1–4) 153-161
- 3 Eisner W, Burtscher J, Bale R , et al. Use of neuronavigation and electrophysiology in surgery of subcortically located lesions in the sensorimotor strip. J Neurol Neurosurg Psychiatry 2002; 72 (3) 378-381
- 4 Ebeling U, Schmid UD, Ying H, Reulen HJ. Safe surgery of lesions near the motor cortex using intra-operative mapping techniques: a report on 50 patients. Acta Neurochir (Wien) 1992; 119 (1–4) 23-28
- 5 Duffau H, Capelle L, Denvil D , et al. Usefulness of intraoperative electrical subcortical mapping during surgery for low-grade gliomas located within eloquent brain regions: functional results in a consecutive series of 103 patients. J Neurosurg 2003; 98 (4) 764-778
- 6 Roux FE, Boulanouar K, Ibarrola D, Tremoulet M, Chollet F, Berry I. Functional MRI and intraoperative brain mapping to evaluate brain plasticity in patients with brain tumours and hemiparesis. J Neurol Neurosurg Psychiatry 2000; 69 (4) 453-463
- 7 Yousry TA, Schmid UD, Jassoy AG , et al. Topography of the cortical motor hand area: prospective study with functional MR imaging and direct motor mapping at surgery. Radiology 1995; 195 (1) 23-29
- 8 Zimmermann M, Seifert V, Trantakis C, Raabe A. Open MRI-guided microsurgery of intracranial tumours in or near eloquent brain areas. Acta Neurochir (Wien) 2001; 143 (4) 327-337
- 9 Achten E, Jackson GD, Cameron JA, Abbott DF, Stella DL, Fabinyi GC. Presurgical evaluation of the motor hand area with functional MR imaging in patients with tumors and dysplastic lesions. Radiology 1999; 210 (2) 529-538
- 10 Ammirati M, Vick N, Liao YL, Ciric I, Mikhael M. Effect of the extent of surgical resection on survival and quality of life in patients with supratentorial glioblastomas and anaplastic astrocytomas. Neurosurgery 1987; 21 (2) 201-206
- 11 Brown PD, Maurer MJ, Rummans TA , et al. A prospective study of quality of life in adults with newly diagnosed high-grade gliomas: the impact of the extent of resection on quality of life and survival. Neurosurgery 2005; 57 (3) 495-504 , discussion 495–504
- 12 Sarmento SA, de Andrade EM, Tedeschi H. Strategies for resection of lesions in the motor area: preliminary results in 42 surgical patients. Arq Neuropsiquiatr 2006; 64 (4) 963-970
- 13 Sarmento SA, Jácome DC, de Andrade EM, Melo AV, de Oliveira OR, Tedeschi H. Relationship between the coronal suture and the central lobe: how important is it and how can we use it in surgical planning?. Arq Neuropsiquiatr 2008; 66 (4) 868-871
- 14 Gusmão S, Reis C, Silveira RL, Cabral G. [Relationships between the coronal suture and the sulci of the lateral convexity of the frontal lobe: neurosurgical applications]. Arq Neuropsiquiatr 2001; 59 (3-A): 570-576
- 15 Ribas GC, Yasuda A, Ribas EC, Nishikuni K, Rodrigues Jr AJ. Surgical anatomy of microneurosurgical sulcal key points. Neurosurgery 2006; 59 (4) (Suppl. 02) ONS177-ONS210 , discussion ONS210–ONS211
- 16 Rhoton Jr AL. The cerebrum. Neurosurgery 2002; 51 (4, Suppl) S1-S51
- 17 Ribas GC, Oliveira Ed. The insula and the central core concept. Arq Neuropsiquiatr 2007; 65 (1) 92-100
- 18 Stone JL. Paul Broca and the first craniotomy based on cerebral localization. J Neurosurg 1991; 75 (1) 154-159
- 19 Bizzi A, Blasi V, Falini A , et al. Presurgical functional MR imaging of language and motor functions: validation with intraoperative electrocortical mapping. Radiology 2008; 248 (2) 579-589
- 20 Araújo D, Machado HR, Oliveira RS , et al. Brain surface reformatted imaging (BSRI) in surgical planning for resections around eloquent cortex. Childs Nerv Syst 2006; 22 (9) 1122-1126
- 21 Cotton F, Rozzi FR, Vallee B , et al. Cranial sutures and craniometric points detected on MRI. Surg Radiol Anat 2005; 27 (1) 64-70
- 22 Boling W, Olivier A, Fabinyi G. Historical contributions to the modern understanding of function in the central area. Neurosurgery 2002; 50 (6) 1296-1309 , discussion 1309–1310
- 23 Gupta DK, Chandra PS, Ojha BK, Sharma BS, Mahapatra AK, Mehta VS. Awake craniotomy versus surgery under general anesthesia for resection of intrinsic lesions of eloquent cortex—a prospective randomised study. Clin Neurol Neurosurg 2007; 109 (4) 335-343
- 24 Bittar RG, Olivier A, Sadikot AF, Andermann F, Pike GB, Reutens DC. Presurgical motor and somatosensory cortex mapping with functional magnetic resonance imaging and positron emission tomography. J Neurosurg 1999; 91 (6) 915-921
- 25 Duffau H. A personal consecutive series of surgically treated 51 cases of insular WHO Grade II glioma: advances and limitations. J Neurosurg 2009; 110 (4) 696-708
- 26 Duffau H, Capelle L, Sichez J , et al. Intra-operative direct electrical stimulations of the central nervous system: the Salpêtrière experience with 60 patients. Acta Neurochir (Wien) 1999; 141 (11) 1157-1167
- 27 Silbergeld DL. Intraoperative transdural functional mapping. Technical note. J Neurosurg 1994; 80 (4) 756-758
- 28 Keles GE, Lundin DA, Lamborn KR, Chang EF, Ojemann G, Berger MS. Intraoperative subcortical stimulation mapping for hemispherical perirolandic gliomas located within or adjacent to the descending motor pathways: evaluation of morbidity and assessment of functional outcome in 294 patients. J Neurosurg 2004; 100 (3) 369-375
- 29 Berman JI, Berger MS, Chung SW, Nagarajan SS, Henry RG. Accuracy of diffusion tensor magnetic resonance imaging tractography assessed using intraoperative subcortical stimulation mapping and magnetic source imaging. J Neurosurg 2007; 107 (3) 488-494
- 30 Zentner J, Meyer B, Stangl A, Schramm J. Intrinsic tumors of the insula: a prospective surgical study of 30 patients. J Neurosurg 1996; 85 (2) 263-271
- 31 Skirboll SS, Ojemann GA, Berger MS, Lettich E, Winn HR. Functional cortex and subcortical white matter located within gliomas. Neurosurgery 1996; 38 (4) 678-684 , discussion 684–685
- 32 Schiffbauer H, Ferrari P, Rowley HA, Berger MS, Roberts TP. Functional activity within brain tumors: a magnetic source imaging study. Neurosurgery 2001; 49 (6) 1313-1320 , discussion 1320–1321
- 33 Tan TC, McL Black P. Image-guided craniotomy for cerebral metastases: techniques and outcomes. Neurosurgery 2003; 53 (1) 82-89 , discussion 89–90
- 34 Reithmeier T, Krammer M, Gumprecht H, Gerstner W, Lumenta CB. Neuronavigation combined with electrophysiological monitoring for surgery of lesions in eloquent brain areas in 42 cases: a retrospective comparison of the neurological outcome and the quality of resection with a control group with similar lesions. Minim Invasive Neurosurg 2003; 46 (2) 65-71
- 35 Ganslandt O, Fahlbusch R, Nimsky C , et al. Functional neuronavigation with magnetoencephalography: outcome in 50 patients with lesions around the motor cortex. J Neurosurg 1999; 91 (1) 73-79
- 36 Zhou H, Miller D, Schulte DM , et al. Transsulcal approach supported by navigation-guided neurophysiological monitoring for resection of paracentral cavernomas. Clin Neurol Neurosurg 2009; 111 (1) 69-78
- 37 Lehéricy S, Duffau H, Cornu P , et al. Correspondence between functional magnetic resonance imaging somatotopy and individual brain anatomy of the central region: comparison with intraoperative stimulation in patients with brain tumors. J Neurosurg 2000; 92 (4) 589-598
- 38 Baciu M, Le Bas JF, Segebarth C, Benabid AL. Presurgical fMRI evaluation of cerebral reorganization and motor deficit in patients with tumors and vascular malformations. Eur J Radiol 2003; 46 (2) 139-146
- 39 Pujol J, Conesa G, Deus J , et al. Presurgical identification of the primary sensorimotor cortex by functional magnetic resonance imaging. J Neurosurg 1996; 84 (1) 7-13
- 40 Desmurget M, Bonnetblanc F, Duffau H. Contrasting acute and slow-growing lesions: a new door to brain plasticity. Brain 2007; 130 (Pt 4): 898-914
- 41 Duffau H. Recovery from complete hemiplegia following resection of a retrocentral metastasis: the prognostic value of intraoperative cortical stimulation. J Neurosurg 2001; 95 (6) 1050-1052
- 42 Fontaine D, Capelle L, Duffau H. Somatotopy of the supplementary motor area: evidence from correlation of the extent of surgical resection with the clinical patterns of deficit. Neurosurgery 2002; 50 (2) 297-303 , discussion 303–305
- 43 Wu JS, Zhou LF, Tang WJ , et al. Clinical evaluation and follow-up outcome of diffusion tensor imaging-based functional neuronavigation: a prospective, controlled study in patients with gliomas involving pyramidal tracts. Neurosurgery 2007; 61 (5) 935-948 , discussion 948–949
- 44 Yoshiura T, Hasuo K, Mihara F, Masuda K, Morioka T, Fukui M. Increased activity of the ipsilateral motor cortex during a hand motor task in patients with brain tumor and paresis. AJNR Am J Neuroradiol 1997; 18 (5) 865-869
- 45 Thiel A, Herholz K, Koyuncu A , et al. Plasticity of language networks in patients with brain tumors: a positron emission tomography activation study. Ann Neurol 2001; 50 (5) 620-629
Address for correspondence
-
References
- 1 Berger MS, Kincaid J, Ojemann GA, Lettich E. Brain mapping techniques to maximize resection, safety, and seizure control in children with brain tumors. Neurosurgery 1989; 25 (5) 786-792
- 2 Berger MS, Ojemann GA. Intraoperative brain mapping techniques in neuro-oncology. Stereotact Funct Neurosurg 1992; 58 (1–4) 153-161
- 3 Eisner W, Burtscher J, Bale R , et al. Use of neuronavigation and electrophysiology in surgery of subcortically located lesions in the sensorimotor strip. J Neurol Neurosurg Psychiatry 2002; 72 (3) 378-381
- 4 Ebeling U, Schmid UD, Ying H, Reulen HJ. Safe surgery of lesions near the motor cortex using intra-operative mapping techniques: a report on 50 patients. Acta Neurochir (Wien) 1992; 119 (1–4) 23-28
- 5 Duffau H, Capelle L, Denvil D , et al. Usefulness of intraoperative electrical subcortical mapping during surgery for low-grade gliomas located within eloquent brain regions: functional results in a consecutive series of 103 patients. J Neurosurg 2003; 98 (4) 764-778
- 6 Roux FE, Boulanouar K, Ibarrola D, Tremoulet M, Chollet F, Berry I. Functional MRI and intraoperative brain mapping to evaluate brain plasticity in patients with brain tumours and hemiparesis. J Neurol Neurosurg Psychiatry 2000; 69 (4) 453-463
- 7 Yousry TA, Schmid UD, Jassoy AG , et al. Topography of the cortical motor hand area: prospective study with functional MR imaging and direct motor mapping at surgery. Radiology 1995; 195 (1) 23-29
- 8 Zimmermann M, Seifert V, Trantakis C, Raabe A. Open MRI-guided microsurgery of intracranial tumours in or near eloquent brain areas. Acta Neurochir (Wien) 2001; 143 (4) 327-337
- 9 Achten E, Jackson GD, Cameron JA, Abbott DF, Stella DL, Fabinyi GC. Presurgical evaluation of the motor hand area with functional MR imaging in patients with tumors and dysplastic lesions. Radiology 1999; 210 (2) 529-538
- 10 Ammirati M, Vick N, Liao YL, Ciric I, Mikhael M. Effect of the extent of surgical resection on survival and quality of life in patients with supratentorial glioblastomas and anaplastic astrocytomas. Neurosurgery 1987; 21 (2) 201-206
- 11 Brown PD, Maurer MJ, Rummans TA , et al. A prospective study of quality of life in adults with newly diagnosed high-grade gliomas: the impact of the extent of resection on quality of life and survival. Neurosurgery 2005; 57 (3) 495-504 , discussion 495–504
- 12 Sarmento SA, de Andrade EM, Tedeschi H. Strategies for resection of lesions in the motor area: preliminary results in 42 surgical patients. Arq Neuropsiquiatr 2006; 64 (4) 963-970
- 13 Sarmento SA, Jácome DC, de Andrade EM, Melo AV, de Oliveira OR, Tedeschi H. Relationship between the coronal suture and the central lobe: how important is it and how can we use it in surgical planning?. Arq Neuropsiquiatr 2008; 66 (4) 868-871
- 14 Gusmão S, Reis C, Silveira RL, Cabral G. [Relationships between the coronal suture and the sulci of the lateral convexity of the frontal lobe: neurosurgical applications]. Arq Neuropsiquiatr 2001; 59 (3-A): 570-576
- 15 Ribas GC, Yasuda A, Ribas EC, Nishikuni K, Rodrigues Jr AJ. Surgical anatomy of microneurosurgical sulcal key points. Neurosurgery 2006; 59 (4) (Suppl. 02) ONS177-ONS210 , discussion ONS210–ONS211
- 16 Rhoton Jr AL. The cerebrum. Neurosurgery 2002; 51 (4, Suppl) S1-S51
- 17 Ribas GC, Oliveira Ed. The insula and the central core concept. Arq Neuropsiquiatr 2007; 65 (1) 92-100
- 18 Stone JL. Paul Broca and the first craniotomy based on cerebral localization. J Neurosurg 1991; 75 (1) 154-159
- 19 Bizzi A, Blasi V, Falini A , et al. Presurgical functional MR imaging of language and motor functions: validation with intraoperative electrocortical mapping. Radiology 2008; 248 (2) 579-589
- 20 Araújo D, Machado HR, Oliveira RS , et al. Brain surface reformatted imaging (BSRI) in surgical planning for resections around eloquent cortex. Childs Nerv Syst 2006; 22 (9) 1122-1126
- 21 Cotton F, Rozzi FR, Vallee B , et al. Cranial sutures and craniometric points detected on MRI. Surg Radiol Anat 2005; 27 (1) 64-70
- 22 Boling W, Olivier A, Fabinyi G. Historical contributions to the modern understanding of function in the central area. Neurosurgery 2002; 50 (6) 1296-1309 , discussion 1309–1310
- 23 Gupta DK, Chandra PS, Ojha BK, Sharma BS, Mahapatra AK, Mehta VS. Awake craniotomy versus surgery under general anesthesia for resection of intrinsic lesions of eloquent cortex—a prospective randomised study. Clin Neurol Neurosurg 2007; 109 (4) 335-343
- 24 Bittar RG, Olivier A, Sadikot AF, Andermann F, Pike GB, Reutens DC. Presurgical motor and somatosensory cortex mapping with functional magnetic resonance imaging and positron emission tomography. J Neurosurg 1999; 91 (6) 915-921
- 25 Duffau H. A personal consecutive series of surgically treated 51 cases of insular WHO Grade II glioma: advances and limitations. J Neurosurg 2009; 110 (4) 696-708
- 26 Duffau H, Capelle L, Sichez J , et al. Intra-operative direct electrical stimulations of the central nervous system: the Salpêtrière experience with 60 patients. Acta Neurochir (Wien) 1999; 141 (11) 1157-1167
- 27 Silbergeld DL. Intraoperative transdural functional mapping. Technical note. J Neurosurg 1994; 80 (4) 756-758
- 28 Keles GE, Lundin DA, Lamborn KR, Chang EF, Ojemann G, Berger MS. Intraoperative subcortical stimulation mapping for hemispherical perirolandic gliomas located within or adjacent to the descending motor pathways: evaluation of morbidity and assessment of functional outcome in 294 patients. J Neurosurg 2004; 100 (3) 369-375
- 29 Berman JI, Berger MS, Chung SW, Nagarajan SS, Henry RG. Accuracy of diffusion tensor magnetic resonance imaging tractography assessed using intraoperative subcortical stimulation mapping and magnetic source imaging. J Neurosurg 2007; 107 (3) 488-494
- 30 Zentner J, Meyer B, Stangl A, Schramm J. Intrinsic tumors of the insula: a prospective surgical study of 30 patients. J Neurosurg 1996; 85 (2) 263-271
- 31 Skirboll SS, Ojemann GA, Berger MS, Lettich E, Winn HR. Functional cortex and subcortical white matter located within gliomas. Neurosurgery 1996; 38 (4) 678-684 , discussion 684–685
- 32 Schiffbauer H, Ferrari P, Rowley HA, Berger MS, Roberts TP. Functional activity within brain tumors: a magnetic source imaging study. Neurosurgery 2001; 49 (6) 1313-1320 , discussion 1320–1321
- 33 Tan TC, McL Black P. Image-guided craniotomy for cerebral metastases: techniques and outcomes. Neurosurgery 2003; 53 (1) 82-89 , discussion 89–90
- 34 Reithmeier T, Krammer M, Gumprecht H, Gerstner W, Lumenta CB. Neuronavigation combined with electrophysiological monitoring for surgery of lesions in eloquent brain areas in 42 cases: a retrospective comparison of the neurological outcome and the quality of resection with a control group with similar lesions. Minim Invasive Neurosurg 2003; 46 (2) 65-71
- 35 Ganslandt O, Fahlbusch R, Nimsky C , et al. Functional neuronavigation with magnetoencephalography: outcome in 50 patients with lesions around the motor cortex. J Neurosurg 1999; 91 (1) 73-79
- 36 Zhou H, Miller D, Schulte DM , et al. Transsulcal approach supported by navigation-guided neurophysiological monitoring for resection of paracentral cavernomas. Clin Neurol Neurosurg 2009; 111 (1) 69-78
- 37 Lehéricy S, Duffau H, Cornu P , et al. Correspondence between functional magnetic resonance imaging somatotopy and individual brain anatomy of the central region: comparison with intraoperative stimulation in patients with brain tumors. J Neurosurg 2000; 92 (4) 589-598
- 38 Baciu M, Le Bas JF, Segebarth C, Benabid AL. Presurgical fMRI evaluation of cerebral reorganization and motor deficit in patients with tumors and vascular malformations. Eur J Radiol 2003; 46 (2) 139-146
- 39 Pujol J, Conesa G, Deus J , et al. Presurgical identification of the primary sensorimotor cortex by functional magnetic resonance imaging. J Neurosurg 1996; 84 (1) 7-13
- 40 Desmurget M, Bonnetblanc F, Duffau H. Contrasting acute and slow-growing lesions: a new door to brain plasticity. Brain 2007; 130 (Pt 4): 898-914
- 41 Duffau H. Recovery from complete hemiplegia following resection of a retrocentral metastasis: the prognostic value of intraoperative cortical stimulation. J Neurosurg 2001; 95 (6) 1050-1052
- 42 Fontaine D, Capelle L, Duffau H. Somatotopy of the supplementary motor area: evidence from correlation of the extent of surgical resection with the clinical patterns of deficit. Neurosurgery 2002; 50 (2) 297-303 , discussion 303–305
- 43 Wu JS, Zhou LF, Tang WJ , et al. Clinical evaluation and follow-up outcome of diffusion tensor imaging-based functional neuronavigation: a prospective, controlled study in patients with gliomas involving pyramidal tracts. Neurosurgery 2007; 61 (5) 935-948 , discussion 948–949
- 44 Yoshiura T, Hasuo K, Mihara F, Masuda K, Morioka T, Fukui M. Increased activity of the ipsilateral motor cortex during a hand motor task in patients with brain tumor and paresis. AJNR Am J Neuroradiol 1997; 18 (5) 865-869
- 45 Thiel A, Herholz K, Koyuncu A , et al. Plasticity of language networks in patients with brain tumors: a positron emission tomography activation study. Ann Neurol 2001; 50 (5) 620-629