RSS-Feed abonnieren
DOI: 10.1055/s-0035-1564887
Surgical Treatment of Cavernous Angiomas in the Pineal Gland – Case Report
Artikel in mehreren Sprachen: English | portuguêsAutor*innen
Address for correspondence
Publikationsverlauf
24. Juli 2015
31. August 2015
Publikationsdatum:
02. Oktober 2015 (online)


Abstract
Pineal cavernous angioma is a vascular malformation that has a prevalence lower than 1%. The etiology is debated. It is believed that it is originated from an autosomal dominant inheritance or from radiotherapeutic treatment. Complete resection enables the cure and prevents complications of the natural evolution of the lesion, mainly hemorrhagic events. A female patient, with 67 years of age, presented mental confusion and visual acuity deficit, which evolved to periods of psychomotor agitation. A magnetic resonance imaging (MRI) scan of the head showed a lobulated mass lesion in the pineal region with hypersignal on T1 and hyposignal on the susceptibility weighted imaging (SWI) sequence. Hydrocephalus was also noticed. The patient underwent a microsurgery for complete lesion resection though a supracerebellar/supratentorial access. The anatomopathology revealed an arteriovenous malformation compatible with cavernous angioma. The pineal cavernous angioma is a rare malformation that should be considered in the differential diagnosis of expansive lesions of the pineal gland.
Introduction
Cavernous angioma is a vascular malformation that usually presents as agglomerates of blood vessels that have a histological characteristic on the vascular walls, and absence of elastic coating, with little or no intervention of the cerebral tissue. They are lesions circumscribed to the interior of the nervous parenchyma.[1] [2]
The most common sites of this lesion are the cerebral hemispheres, followed by the brainstem, the cavernous sinus, the basal ganglia and the thalamus. Considered a disease most commonly reported in females, its diagnosis is usually made after neurological manifestations related to the location of the angiomas. Thus, focal deficits, headache and seizures may occur. Accidental imaging findings are frequently observed in asymptomatic patients.[1] [3] [4]
Magnetic resonance imaging (MRI) is an imaging technique that has a greater sensitivity for the detection of angiomas,[5] and it shows a typical image of a T2-weighted peripheral hypodense ring suggestive of hemosiderin, as well as the interior of the lesion with a heterogeneous characteristic.[5] [6]
Surgical removal makes it possible to cure cavernous angioma, and is the most advised technique to avoid the complications of the natural evolution of this lesion, especially hemorrhage.[1] [3] [7] Guided stereotactic surgery is considered safer and rapid for the total resection of subcortical and deep cerebral cavernous angiomas.[1]
The cavernous angioma surrounding the pineal gland has a probability of occurrence < 1%.[7] The first reported case of angioma in the pineal gland was in 1961; the malformation was partially removed, and the patient died after an episode of cerebral hemorrhage. From that date until the year 2010, 21 cases of cavernous angioma in the pineal gland region were reported.[3] [7]
The present study reports a case of cavernous angioma in the topography of the pineal gland, with supratentorial hydrocephalus, in which a complete surgical resection was chosen.
Due to the infrequency of cavernous angioma in the pineal gland region, and because it is a curable lesion, studies that seek to deepen the knowledge of this disease are relevant.
Case Report
E.Z.F.I, a 67-year-old woman, presented an incipient blurred vision and was evaluated by an ophthalmologist, who did not observe alterations in the examination. The patient had improvement in the period of 60 days, but, 2 months after this period, she presented mental confusion, bilateral visual acuity deficit and progressive gait ataxia associated with retrograde amnesia and inversion of the sleep and wake cycle, remaining sleepy during most of the day and alert at night. There was worsening in the nocturnal insomnia, mental confusion, and gait ataxia, which consequently restricted her to the bed and the wheelchair; thus, she needed help to perform her basic routine activities.
Three weeks later, she presented a fall from her own height, and was then referred and admitted for evaluation in the emergency room. There was no report of worsening in the consciousness level, vomiting or trauma-related headache. Upon admission, the patient presented ocular opening responding to simple commands, she was confused, disoriented regarding time and space, with periods of psychomotor agitation. The pupils were isocoric and had preserved photoreactive reflex. Although it did not cooperate adequately with the neurological examination, absence of motor deficit was observed with the active mobilization of the four limbs. Extrinsic ocular motility also did not reveal apparent changes; however, the patient presented bilateral visual acuity deficit. When positioned to ambulate, she presented ataxic gait with postural instability.
A head computed tomography (CT) scan, performed at admission, revealed significant dilatation of the ventricular system. There was a hyperdense expansive lesion with hemorrhagic appearance located in the topography of the mesencephalon ceiling in the pineal gland region, which caused supratentorial obstructive hydrocephalus.
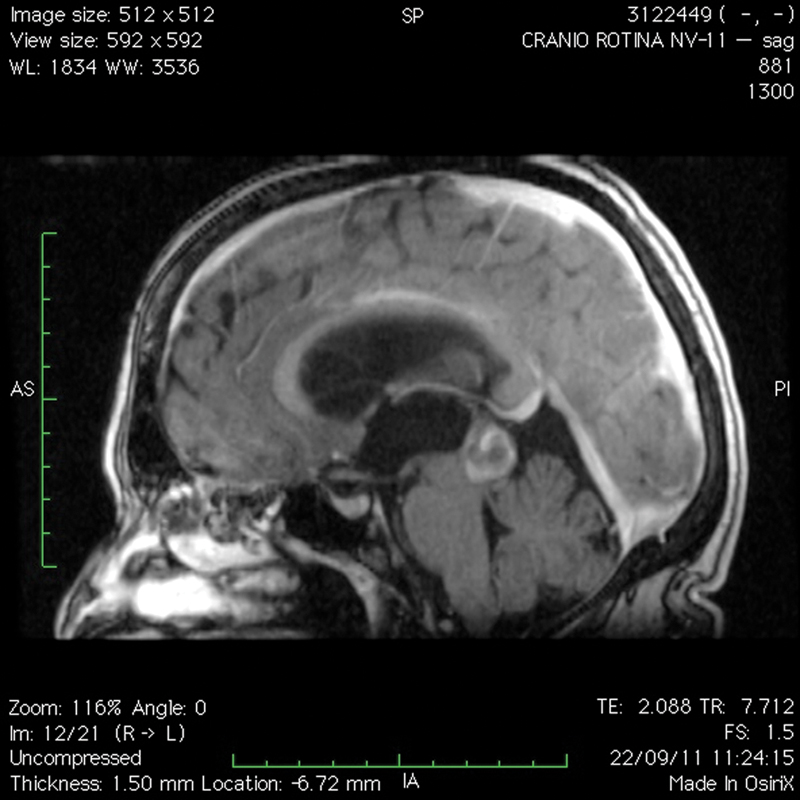
An MRI scan, performed after contrast injection, confirmed the presence of a macrolobulated expansive lesion affecting the topography of the pineal gland, and measuring 17 × 24 × 17 mm. The lesion presented a hypersignal in T1 ([Fig. 1]) with a hyposignal mark in the susceptibility weighted imaging SWI sequence, suggesting blood content as well as moderate contrast uptake.

This lesion caused obliteration of the cerebral aqueduct, with consequent obstruction of the suprathoracic ventricles ([Fig. 2]) associated with the moderate ependymal transudation revealed by the hypersignal in T2 ([Fig. 3]) and the fluid-attenuated inversion recovery (FLAIR) of the periventricular white matter. The diagnostic impression of the radiologist was of an expansive germinal lesion.


We chose to perform microsurgery with supratentorial, supracerebellar inter-hemispheric access. During the surgical procedure, the left lateral ventricle was punctured with the placement of an external ventricular derivation (EVD). The operative finding was a violaceous and capsulated lesion. The microsurgical incision of the lesion revealed its content, with organized clots and a discrete amount of nervous tissue. The report of the anatomopathological examination of the intraoperative frozen sections was compatible with cavernous angioma, and the lesion was completely removed.
In the postoperative period, the patient was gradually awakened in the intensive care unit (ICU). The EVD was kept open for cerebrospinal fluid (CSF) drainage. A CT scan of the skull for postoperative control revealed improvement in ventricular dilatation, total removal of the angioma, and pneumocephalus. The patient was extubated and presented progressive improvement in the level of consciousness and visual acuity. The EVD was closed after 48 hours, and the patient did not present alterations in the neurological picture. The EVD was removed, and the patient was discharged from the ICU. A new CT scan of the skull was performed, and it showed absence of hydrocephalus and elimination of the pneumocephalus ([Fig. 4]). On the subsequent days, the patient presented neurological improvement and was discharged from the hospital; she was alert, oriented, and ambulating with assistance. There was an improvement in visual acuity and normal extrinsic ocular motricity. The definitive anatomopathological report was compatible with an arteriovenous malformation: cavernous angioma.

Discussion
Cavernous angioma is a vascular malformation that accounts for 5 to 13% of lesions in the central nervous system.[7] Histologically, it presents thin walls of endothelial cells separated by fibrous collagen, and no elastic coating, with little or no intervention of the cerebral parenchyma.[1] [2]
The etiology of cavernous angioma is still a subject of discussion, but there is evidence that this lesion is derived from an autosomal dominant inheritance located on chromosome 7,[8] and there is still the possibility of radiotherapy-induced cavernous angioma.[5] The formation of radiotherapy-induced cavernous angioma is relatively infrequent, and usually occurs in pediatric patients.[6] The most characteristic sites of cavernous angiomas are the cerebral hemispheres, the brainstem, the cavernous sinus, the basal ganglia and the thalamus.[4] Supratentorial lesions comprise 80 to 90% of the cases; infratentorial lesions, 15%; and lesions in the spinal cord, 5%. Of the total cavernous malformations, 9 to 35% occur in the brainstem,[9] and the probability of involvement of the pineal gland region is < 1%.[5]
The risk of hemorrhage in cavernous angiomas varies according to the location: those lesions located more deeply, such as those in the brainstem, thalamus or basal ganglia, present a risk of 4.1%; in the cases of superficial craniomas, 0.4%,[5] [9] whereas the risk of hemorrhage in the region of the pineal gland is quite small.[3] Regardless of the area affected by the cavernous angioma, an initial hemorrhage significantly increases a new episode of hemorrhage.[5] Studies have shown that female patients have a higher incidence of bleeding, probably due to hormonal changes.[4]
The patient in the case reported here presented with bleeding visualized on the MRI scan ([Figs. 1] and [2]), but it is not possible to determine if this event was the first bleeding, since there are no prior examinations for comparison.
Magnetic resonance imaging is the method of choice for the detection and diagnosis of cavernous angioma because it is a more sensitive examination.[5] The characteristic image of a cavernous angioma includes a low-intensity, more sensitive T2-weighted peripheral ring due to the deposition of hemosiderin in the surrounding parenchyma, a result of small hemorrhages that most commonly exhibit a mixed intensity nucleus on both T1 and T2 images. ([Fig. 2]). These characteristics may vary depending on the imaging sequences, as they are determined by the blood products within the lesion and by the surrounding hemosiderin ring. Although it is an excellent tool for diagnosis, it is advisable to complement it with other sequences of images for a more precise definition of the lesion.[10]
The clinical diagnosis of this disease is difficult, since it can be confused with other lesions in the pineal gland,[3] as it frequently occurs in cases of pineocytomas and pineoblastomas, but especially in cases of germ-cell tumors.[3] This usually happens because the germ cells are more localized characteristic in the pineal gland or neurohypophysis, and the occurrence of germ-cell tumors is greater than that of cavernous angiomas in this region, varying from 4 to 9%.[11]
The clinical manifestations related to the disease vary; a common manifestation is the sign of Parinaud, characterized mainly by difficulty in vertical ocular movement; other manifestations may be signs of intracranial hypertension, headache, visual disturbances, gait ataxia, and altered circadian rhythm. In addition, there are still signs of hemiparesis, hemi-hypoesthesia, diabetes insipidus, and amenorrhea with elevated prolactin. Neuroendocrine disorders occur mainly due to damage to the hypothalamus region by distension of the floor of the third ventricle.
Cavernous angioma located in the pineal gland is usually accompanied by supratentorial hydrocephalus with dilation of the lateral ventricles and third ventricle, and the fourth ventricle is preserved. There may be, though more rarely, an obstruction of the aqueduct through a dilated subependymal vein, functioning as a venous channel for the angioma.[12] Patients who develop obstruction of the aqueduct, causing hydrocephalus, may present intracranial hypertension with headache, mental confusion and relegation of the level of consciousness.[3] [4]
For the treatment of supratentorial hydrocephalus, from the case reported here, an EVD was performed. Another method that could be chosen is the third ventriculostomy, considered to be less invasive and with visual control of procedures. This method is seen as a simple procedure unless there is anatomical variation in the floor of the third ventricle, especially in cases of long-standing hydrocephalus, and it also contributes as a less infectious form when compared with external ventricular drain.[13] [14] [15]
The surgery for the total removal of the cavernous angioma from the case reported here was performed by supracerebellar supratentorial interhemispheric access due to the surgeon's experience and to the anatomical particularity of the region, which enabled safe access to the pineal gland following the cerebral falx and tentorium. Other surgical techniques could be used, such as intraoperative localization (neuronavigation) or stereotactic surgery.[16]
Despite the surgeon's choice, stereotactic surgery has been the most used approach for cavernous angiomas, because the mortality of these surgeries is very low, ∼ 2%. The choice of approach is usually made by verification of the brain tissue enveloped in the structures, based on imaging exams such as the MRI. The main postoperative complications are hemorrhages and neurological deficits.[17]
The most advanced technology is neuronavigation surgery, which consists of the use of an equipment capable of associating images of the patient's MRI with real-time magnetoencephalogram images, giving the surgeon greater precision, since he/she has access to the anatomy, and the possibility of better planning for access and approach routes.[18]
Complete removal of the cavernous angioma enables the healing of this type of lesion, and is also the most advisable technique to avoid the complications that this malformation can lead to with its natural evolution, such as recurrent bleeding, convulsions and neurological deficits.
Conclusion
Based on this study, it is considered important that the occurrence of cavernous angioma, although rare, be evaluated in the diagnoses of cases of lesions in the pineal gland. In the case reported here, we verified that the surgical approach associated with the control of the hydrocephalus is a safe option for the treatment of this disease.
Die Autoren geben an, dass kein Interessenkonflikt besteht.
-
References
- 1 Meneses MS, Dallolmo VC, Kondageski C, Ramina R, Hunhevicz S, Pedrozo AA. Cirurgia Estereotáxica Guiada para Angiomas Caver- nosos. Neuropsiquiatr 2000; 58 (01) 71-75
- 2 Bartlett JE, Kishore PRS. Intracranial cavernous angioma. AJR Am J Roentgenol 1977; 128 (04) 653-656
- 3 Chamadoira C, Cerejo A, Vilarinho A, Castro L, Vaz R. Malformación cavernosa de la región pineal. Caso clínico y revisión de la literatura. Neurocir 2010; 21: 138-145
- 4 Gross BA, Lin N, Du R, Day AL. The natural history of intracranial cavernous malformations. Neurosurg Focus 2011; 30 (06) E24
- 5 Burn S, Gunny R, Phipps K, Gaze M, Hayward R. Incidence of cavernoma development in children after radiotherapy for brain tumors. J Neurosurg 2007; 106 (5, Suppl) 379-383
- 6 Martínez León MI. Detección precoz mediante resonancia magnética de un angioma cavernoso tras radioterapia craneal por ependimoma anaplásico en un niño. Radiologia 2013; 55 (06) 541-545
- 7 Muzumdar DP, Misra BK, Bhaduri AS. Pineal region cavernoma--case report. Neurol Med Chir (Tokyo) 2000; 40 (07) 372-379
- 8 Günel M, Awad IA, Anson J, Lifton RP. Mapping a gene causing cerebral cavernous malformation to 7q11.2-q21. Proc Natl Acad Sci U S A 1995; 92 (14) 6620-6624
- 9 Ramírez-Zamora A, Biller J. Brainstem cavernous malformations: a review with two case reports. Arq Neuropsiquiatr 2009; 67 (3B): 917-921
- 10 Campbell PG, Jabbour P, Yadla S, Awad IA. Emerging clinical imaging techniques for cerebral cavernous malformations: a systematic review. Neurosurg Focus 2010; 29 (03) E6
- 11 Nagaishi M, Suzuki R, Tanaka Y. , et al. Pure germinoma of the pineal gland with synchronous spinal dissemination--case report. Neurol Med Chir (Tokyo) 2010; 50 (06) 505-508
- 12 Bannur U, Korah I, Chandy MJ. Midbrain venous angioma with obstructive hydrocephalus. Neurol India 2002; 50 (02) 207-209
- 13 Martins R, Ciquini Júnior O, Matushita H, Cabral ND, Plese JPP. Infecções de derivações liquóricas em crianças. Revisão de 100 infecções em 87 crianças. Arq Neuropsiquiatr 1997; 55 (01) 75-81
- 14 Pfisterer W, Mühlbauer M, Czech T, Reinprecht A. Early diagnosis of external ventricular drainage infection: results of a prospective study. J Neurol Neurosurg Psychiatry 2003; 74 (07) 929-932
- 15 Morota N, Watabe T, Inukai T, Hongo K, Nakagawa H. Anatomical variants in the floor of the third ventricle; implications for endoscopic third ventriculostomy. J Neurol Neurosurg Psychiatry 2000; 69 (04) 531-534
- 16 Aguiar LR, Maeda AK, Francisco AN, Mattozo CA, Marques R. Angioma cavernoso: ressecção microcirúrgica guiada por imagem– Relato de caso. J Bras Neurocirurg 2003; 14 (01) 21-24
- 17 Hassler W, Hejazi N. Complications of angioma surgery--personal experience in 191 patients with cerebral angiomas. Neurol Med Chir (Tokyo) 1998; 38 (Suppl): 238-244
- 18 Ganslandt O, Behari S, Gralla J, Fahlbusch R, Nimsky C. Neuronavigation: concept, techniques and applications. Neurol India 2002; 50 (03) 244-255
Address for correspondence
-
References
- 1 Meneses MS, Dallolmo VC, Kondageski C, Ramina R, Hunhevicz S, Pedrozo AA. Cirurgia Estereotáxica Guiada para Angiomas Caver- nosos. Neuropsiquiatr 2000; 58 (01) 71-75
- 2 Bartlett JE, Kishore PRS. Intracranial cavernous angioma. AJR Am J Roentgenol 1977; 128 (04) 653-656
- 3 Chamadoira C, Cerejo A, Vilarinho A, Castro L, Vaz R. Malformación cavernosa de la región pineal. Caso clínico y revisión de la literatura. Neurocir 2010; 21: 138-145
- 4 Gross BA, Lin N, Du R, Day AL. The natural history of intracranial cavernous malformations. Neurosurg Focus 2011; 30 (06) E24
- 5 Burn S, Gunny R, Phipps K, Gaze M, Hayward R. Incidence of cavernoma development in children after radiotherapy for brain tumors. J Neurosurg 2007; 106 (5, Suppl) 379-383
- 6 Martínez León MI. Detección precoz mediante resonancia magnética de un angioma cavernoso tras radioterapia craneal por ependimoma anaplásico en un niño. Radiologia 2013; 55 (06) 541-545
- 7 Muzumdar DP, Misra BK, Bhaduri AS. Pineal region cavernoma--case report. Neurol Med Chir (Tokyo) 2000; 40 (07) 372-379
- 8 Günel M, Awad IA, Anson J, Lifton RP. Mapping a gene causing cerebral cavernous malformation to 7q11.2-q21. Proc Natl Acad Sci U S A 1995; 92 (14) 6620-6624
- 9 Ramírez-Zamora A, Biller J. Brainstem cavernous malformations: a review with two case reports. Arq Neuropsiquiatr 2009; 67 (3B): 917-921
- 10 Campbell PG, Jabbour P, Yadla S, Awad IA. Emerging clinical imaging techniques for cerebral cavernous malformations: a systematic review. Neurosurg Focus 2010; 29 (03) E6
- 11 Nagaishi M, Suzuki R, Tanaka Y. , et al. Pure germinoma of the pineal gland with synchronous spinal dissemination--case report. Neurol Med Chir (Tokyo) 2010; 50 (06) 505-508
- 12 Bannur U, Korah I, Chandy MJ. Midbrain venous angioma with obstructive hydrocephalus. Neurol India 2002; 50 (02) 207-209
- 13 Martins R, Ciquini Júnior O, Matushita H, Cabral ND, Plese JPP. Infecções de derivações liquóricas em crianças. Revisão de 100 infecções em 87 crianças. Arq Neuropsiquiatr 1997; 55 (01) 75-81
- 14 Pfisterer W, Mühlbauer M, Czech T, Reinprecht A. Early diagnosis of external ventricular drainage infection: results of a prospective study. J Neurol Neurosurg Psychiatry 2003; 74 (07) 929-932
- 15 Morota N, Watabe T, Inukai T, Hongo K, Nakagawa H. Anatomical variants in the floor of the third ventricle; implications for endoscopic third ventriculostomy. J Neurol Neurosurg Psychiatry 2000; 69 (04) 531-534
- 16 Aguiar LR, Maeda AK, Francisco AN, Mattozo CA, Marques R. Angioma cavernoso: ressecção microcirúrgica guiada por imagem– Relato de caso. J Bras Neurocirurg 2003; 14 (01) 21-24
- 17 Hassler W, Hejazi N. Complications of angioma surgery--personal experience in 191 patients with cerebral angiomas. Neurol Med Chir (Tokyo) 1998; 38 (Suppl): 238-244
- 18 Ganslandt O, Behari S, Gralla J, Fahlbusch R, Nimsky C. Neuronavigation: concept, techniques and applications. Neurol India 2002; 50 (03) 244-255