
RSS-Feed abonnieren
DOI: 10.1055/s-0037-1599056
Residents' Learning Curve of Lumbar Transforaminal Epidural Steroid Injections
Abstract
Background and Study Aims There is a paucity of literature on beginners' training and on its connection with patient safety for transforaminal epidural steroid injections (TFESIs). This study retrospectively assessed the learning curves and associated complications of neurosurgery residents never previously exposed to TFESI and compared them with experienced board-certified faculty neurosurgeons (BCFNs).
Material and Methods Procedure time in minutes, dose-area product (DAP) in cGy*cm2, periprocedural observations, and complications in 354 TFESIs for radicular pain secondary to lumbar disk herniation or lumbar spinal stenosis were extracted from operative notes and the electronic infiltration logbook in the per-injection format. Learning curves for 238 residents and 116 BCFN TFESIs in terms of procedure time and DAP were estimated using monotone regression.
Results Residents' TFESI procedure time and DAP reached BCFN level (4.7 minutes and 140.2 Gy*cm2) after 67 and 68 cases, respectively. Residents' TFESIs were unsuccessful in 1.7%, mostly for severe obesity and hypertrophied facet joints, but no severe complications were noted. Obesity, however, did not result in increased procedure times or radiation exposure in general. Residents were faster and required less fluoroscopy in TFESI of the upper lumbar nerve roots than for L5 or S1 in particular.
Conclusion The residents' learning curve for TFESIs in terms of procedure time and radiation exposure can be overcome safely after < 70 TFESIs. An outcome analysis correlating to the interventionalist's training level would be worth investigating in future studies.
#
Keywords
learning curve - lumbar disk herniation - lumbar spinal stenosis - resident training - transforaminal epidural steroid injectionIntroduction
In the care of patients with radiculopathy secondary to a lumbar disk herniation or lumbar spinal stenosis, treating physicians increasingly rely on a trial of transforaminal epidural steroid injections (TFESIs). A combination of a local anesthetic and glucocorticoid is usually applied epidurally to the affected nerve root via a transforaminal or interlaminar approach under imaging guidance. Despite the fact that TFESI has been used for many decades, the pathophysiologic mechanism behind it and the efficacy of this procedure remain a source of controversy. In light of reported severe complications, safety precautions have been recommended.[1] Most studies today, including those of our institution,[2] are performed by interventionalists with long-standing experience in TFESI. However, patient care in teaching hospitals is provided by physicians with varying degrees of experience. In a previous report, the involvement of musculoskeletal and neuroradiology fellows in TFESI did not prolong fluoroscopy time and/or increase the radiation dose.[3] But how do beginners do in TFESI? We describe the learning curves and associated complications of four neurosurgery residents never previously exposed to TFESI and compare them with experienced board-certified faculty neurosurgeons (BCFNs).
#
Material and Methods
Training Program
According to our institution's structured training program ([Supplementary Table 1]), neurosurgery residents are introduced to lumbar TFESIs at the end of their postgraduate year (PGY)-1, first by observing at least 10 TFESIs. After positive appraisal of the BCFN in charge, they are allowed to perform TFESI under supervision. When deemed fit to safely perform TFESI, they proceed on their own, although a backup BCFN is always available in case of unforeseen problems.
#
Injection Technique
All TFESI procedures by residents and BCFNs were performed in the same manner under fluoroscopy guidance (Siemens Arcadis Varic, Munich, Germany). The transforaminal technique, which was previously shown to be equally[2] [4] [5] or even more effective[5] [6] [7] than the interlaminar technique, was used in all patients. The patient was in the prone position and the lumbosacral region disinfected with isopropyl and propyl alcohol with 2-phenylphenol (Kodan Forte, Schülke & Mayr, Zurich, Switzerland) and draped in a sterile manner. The correct level was determined with anteroposterior (AP) fluoroscopy. For TFESI, we never use local anesthesia for the skin. Procedure time was recorded at the point the Chiba needle (ECOJEKT 23G, 15 cm length, HS Hospital Service, Aprilia, Italy) was poked through the skin. Under single-shot fluoroscopy guidance, the needle was advanced to the base of the subjacent pedicle (so-called safe triangle[8]). For the S1 root, the needle was inserted into the craniomedial aspect of the first sacral foramen. To control depth and check for the correct needle position, the image intensifier, which was handled by operating room personnel on verbal command of the interventionalist, had to be rotated from AP to lateral and back if required. After negative flashback/aspiration, 1 to 5 mL contrast agent iopamidol 300 mg/mL (Iopamiro 300, Bracco Suisse, Manno, Switzerland) were applied under continuous fluoroscopy to ensure periradicular spread and rule out intravascular needle tip placement ([Fig. 1]). A mixture of 2 to 3 mL of 40 mg/mL triamcinolone (Kenacort-A 40, Dermapharm, Hünenberg, Switzerland) and 0.5% bupivacaine (Bupivacaine hydrochloride, Sintetica, Mendrisio, Switzerland) was administered in the ratio 1:5. Ideally, patients experienced a transient triggering of leg pain or reported tingling sensations down the leg during the injection of the drugs. Operation time ended with needle withdrawal. Throughout the procedure, the DAP in cGy*cm2 was recorded.

#
Study Groups
The resident TFESI group included all consecutive patients who received TFESIs by four neurosurgery residents starting with their first case during their training. They were compared with TFESIs performed by four BCFNs with special focus on spine surgery and long experience with TFESIs during the same time interval.
#
Data Collection
The operative notes and infiltration room electronic logbook were reviewed retrospectively. Procedure time in minutes and the dose-area product (DAP) in cGy*cm2 were used to create learning curves. Patient demographic data (age, gender, weight, and height) were extracted from the patient charts. Diagnosis, procedure-related details (nerve root level, side), and procedural observations were recorded. The latter included flashback/aspiration of blood or cerebrospinal fluid (CSF), contrast-confirmed intravascular needle tip placement, whether the patient reported a transient triggering of leg pain, tingling sensations, and so on, during the injection, as well as procedural complications and TFESI failures. In order to not exclude any patients who received TFESI for multiple nerve roots in the same session, procedure time and DAP were converted into the per-injection format as done by Smuck et al.[9]
#
Statistical Considerations
Dependent variables were TFESI time in minutes, DAP in cGy*cm2, and intraoperative observations. Independent variables were resident status of the physician, nerve root level, and the patient's body mass index (BMI) in kg/m2. An additional analysis was done on the residents' PGY. Relationships were first visualized graphically and analyzed for trends. Independent variables were then dichotomized into resident versus BCFN, upper (L1–L4) and lower nerve roots (L5–S1), obese (BMI ≥ 30 kg/m2) versus nonobese (BMI < 30 kg/m2), and whether the respective resident was at the beginning (junior level, PGY 1–3) or at the end of his or her training (senior level, PGY 4–6). Analysis of continuous variables (TFESI time and DAP) was performed using rank sum tests. Analysis of categorical variables (procedural observations and complications) was done using logistic regression with the results presented as odds ratio (OR) with 95% confidence intervals (CIs). Because there were baseline differences between patients treated by residents and BCFNs ([Table 1]), an additional multivariate logistic regression model was built. The software used for the statistical analysis was Stata v.14 (StataCorp, College Station, Texas, United States). The learning curves were estimated using monotone regression available with the isoreg function in R (v.3.2.2)[10] as previously reported.[11] [12]
#
#
Results
[Tables 1] and [2] provide baseline characteristics, procedural variables, and observations in the per-injection format. Four residents performed 238 TFESIs (resident 1, 82; resident 2, 81; resident 3, 38; and resident 4, 37). In total, 182 TFESIs were performed by residents in their junior stage (76.5%; PGY 1–3) and 56 TFESIs by residents in their senior stage of training (23.5%; PGY 4–6). At the beginning, they were supervised for an average of 5.3 cases (range: 2–9). Throughout the rest of their learning curve, BCFNs were called in for help in nine instances (4.1%). During the same time interval, 116 TFESIs were performed by four BCFNs. A total of 77 patients (21.8%) were considered obese, and one third of all TFESIs was performed for nerve roots L1–L4 (120 [33.9%]), whereas two thirds targeted L5 or S1 (234 [66.1%]). Baseline characteristics were balanced for most parameters except for patient age, indication, and nerve root level.
|
Resident TFESIs |
BCFN TFESI |
p value |
|||
|---|---|---|---|---|---|
|
Age, y |
57.1 |
16.4 |
62.1 |
15.3 |
0.009 |
|
Gender |
0.084 |
||||
|
Male |
134 |
56.3% |
54 |
46.6% |
|
|
Female |
104 |
43.7% |
62 |
53.4% |
|
|
Body proportions |
|||||
|
Weight, kg |
77.7 |
12.7 |
79.7 |
15.2 |
0.221 |
|
Height, cm |
172.1 |
9.3 |
170.7 |
9.6 |
0.364 |
|
Body mass index, kg/m2 |
26.3 |
4.4 |
27.4 |
5.4 |
0.142 |
|
Indication for TFESI |
< 0.001 |
||||
|
Lumbar disk herniation |
176 |
73.9% |
36 |
31.0% |
|
|
Lumbar spinal stenosis |
62 |
26.1% |
80 |
69.0% |
|
|
Nerve root |
0.040 |
||||
|
L1 |
1 |
0.4% |
1 |
0.9% |
|
|
L2 |
6 |
2.5% |
3 |
2.6% |
|
|
L3 |
26 |
10.9% |
13 |
11.2% |
|
|
L4 |
37 |
15.6% |
33 |
28.5% |
|
|
L5 |
108 |
45.4% |
50 |
43.1% |
|
|
S1 |
60 |
25.2% |
16 |
13.8% |
|
|
Side |
0.047 |
||||
|
Right |
119 |
50.0% |
71 |
61.2% |
|
|
Left |
119 |
50.0% |
45 |
38.8% |
|
|
Total |
n = 238 |
100% |
n = 116 |
100% |
|
Abbreviations: BCFN, board-certified faculty neurosurgeon; TFESI, transforaminal epidural steroid injection.
a A total of 238 and 116 TFESIs were performed by neurosurgery residents and BCFNs, respectively.
Note: Categorical variables are presented as count and percentage, nominal variables as mean and standard deviation.
|
Resident TFESI |
BCFN TFESI |
p value |
|||
|---|---|---|---|---|---|
|
TFESI time, min |
7.8 |
3.8 |
4.7 |
1.5 |
< 0.001 |
|
DAP, Gy*cm2 |
268.1 |
321.0 |
140.2 |
133.7 |
0.087 |
|
Periprocedural observations |
0.028 |
||||
|
Nothing special |
223 |
93.7% |
115 |
99.1% |
|
|
Yes |
15 |
6.3% |
1 |
0.9% |
|
|
CSF aspiration |
3 |
1.3% |
– |
– |
|
|
Flashback/Blood aspiration |
4 |
1.7% |
1 |
0.9% |
|
|
Intravascular needle tip placement |
8 |
3.3% |
– |
– |
|
|
Provocation during injection |
< 0.001 |
||||
|
Yes |
144 |
60.5% |
97 |
83.6% |
|
|
No |
94 |
39.5% |
19 |
16.4% |
|
|
Treatment |
0.307 |
||||
|
Successful |
234 |
98.3% |
116 |
100% |
|
|
Unsuccessful |
4 |
1.7% |
– |
0% |
|
|
Total |
n = 238 |
100% |
n = 116 |
100% |
|
Abbreviations: BCFN, board-certified faculty neurosurgeon; CSF, cerebrospinal fluid; DAP, dose-area product; TFESI, transforaminal epidural steroid injection.
a Total of 238 and 116 fluoroscopy-guided lumbar TFESIs performed by neurosurgery residents and BCFNs, respectively.
Note: Categorical variables are presented as count and percentage, nominal variables as mean and standard deviation.
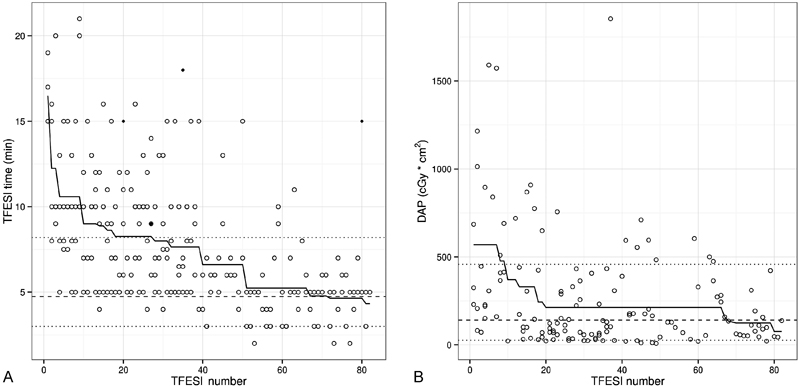
Learning Curve and TFESI Time
Procedure time was < 10 minutes by the 10th and approximated BCFN level (4.7 minutes) by the 67th TFESI ([Figs. 2A] and [3A]). TFESI time was significantly longer for those performed by junior compared with senior residents (8.50 ± 3.94 minutes versus 5.71 ± 2.39 minutes; p < 0.0001; [Fig. 3B]). Mean TFESI time for the upper lumbar nerve roots (L1–L4; 6.26 ± 3.74 minutes) was significantly shorter than for the lower nerve roots L5 or S1 (7.12 ± 3.44 minutes; p = 0.0006; [Fig. 3C]). TFESI was similarly long in nonobese (6.97 ± 3.56 minutes) and obese patients (6.31 ± 3.54 minutes; p = 0.0756).

#
Learning Curve and DAP
There was missing data for DAP in 94 of 238 (39.5%) residents and 38 of 116 (32.8%) BCFN TFESIs. In terms of DAP, the largest improvement was observed by the 20th TFESI, when DAP had reduced from 569 at baseline to 213 cGy*cm2 ([Fig. 2B]). After that, there was a long plateau until around the 68th TFESI when average DAP reduced to 135 cGy*cm2 and reached the BCFN mean DAP of 140.2 Gy*cm2.
In general, residents tended to use more radiation than BCFNs (268.1 versus 140.2 Gy*cm2; p = 0.087; [Fig. 3D]), and there was a strong tendency for more radiation exposure caused by junior residents (306.87 ± 357.33 Gy*cm2) compared with senior residents (160.09 ± 140.63 Gy*cm2; p = 0.067; [Fig. 3E]). From both figures it becomes evident that the range of used radiation was large. In general, more radiation was needed for levels L5 and S1 (281.49 ± 336.70 Gy*cm2) compared with the upper lumbar levels (153.49 ± 143.16 Gy*cm2; p = 0.0441; [Fig. 3F]). Obese patients were equally exposed to radiation (249.35 ± 216.03 Gy*cm2) as nonobese patients (243.17 ± 315.11 Gy*cm2; p = 0.2228).
#
Difficulties, Complications, and Procedural Observations
Four resident TFESIs failed (1.7%) due to the inability to pass a hypertrophied facet joint with the needle in two cases, obesity in one case and for reasons not further specified in another case. In one resident case, the injectate had to be administered 1.5 cm lateral to the neuroforamen due to obesity, but for statistical analysis this TFESI was considered successful. A change to an extra-long needle in one obese patient and four facet joint obstacles were reported in the BCFN group, but all these cases could be completed and were considered successful TFESIs.
No severe complications occurred in any of the groups. A total of 16 procedural observations were made of which 15 occurred during resident TFESIs. In univariate analysis, residents were more likely to observe flashback/aspiration of blood or CSF or contrast-confirmed intravascular needle tip placement (OR: 7.18; 95% CI, 0.93–55.34; p = 0.058). Once corrected for baseline group differences including age, gender, underlying diagnosis, segment, and side, the effect became more pronounced and statistically significant (OR: 10.25; 95% CI, 1.24–84.38; p = 0.030). Within the group of residents, junior status was no predictor of a procedural observation (OR: 1.32; 95% CI, 0.39–4.39; p = 0.648). Likewise, neither obesity (OR: 0.89; 95% CI, 0.25–3.25; p = 0.867) nor TFESI for nerve roots L5 or S1 (OR: 1.03; 95% CI, 0.34–3.07; p = 0.962) were significant predictors of procedural observations.
#
#
Discussion
In this first report on TFESI beginners, we demonstrate that the learning curve in terms of procedure time and DAP is overcome in < 70 cases when these variables approximate expert (BCFN) level. Significant improvement can already be seen after 10 to 20 cases, shortly after residents performed TFESI without supervision. Because no severe complications occurred and difficulties encountered in TFESI led to unsuccessful ESI in a few cases only, the present data suggest that patient safety is warranted while trainees build up experience with this technique. The current work lines up with a series of previous reports assessing the safety of neurosurgery resident training surgery.[11] [13] [14] [15] [16]
Considering potential long-term consequences of radiation exposure, DAP should be kept at a minimum. Because DAP was significantly higher at the beginning of the learning curve with a strong trend toward a higher DAP within the group of residents with junior status, a longer resident supervision to train a goal-directed use of fluoroscopy would be ideal. Our data suggest that an acceptable reduction in DAP can be achieved by the 20th case. However, continuous resident supervision for so-called simple procedures such as TFESI can be difficult in busy neurosurgery routines. Introductory seminars on lumbar spine procedures[17] could potentially shorten the learning curve.
Severe obesity and hypertrophied facet joints resulted in some unsuccessful resident TFESIs. These conditions therefore prove unsuitable for beginners in TFESI, although according to our data, obesity did not result in increased procedure times[9] and radiation exposure[3] [9] as previously reported. The data further support our personal experience that TFESI of the upper lumbar nerve roots is easier to perform than TFESI for L5 or S1 in particular; as for the former, residents were faster and required less fluoroscopy. More degeneration of hypertrophied facet joints of the lumbosacral segments, the iliac crest interfering with the transforaminal trajectory of L5 ESI, and problems to visualize the S1 foramen using fluoroscopy might all be explanations. It is recommended that junior residents perform their first 20 TFESIs on upper lumbar nerve roots in slim patients.
Pain provocation during injection indicates direct drug application in the proximity of the nerve root and could be regarded as proxy of a technically successful TFESI, and this was more often achieved by BCFNs than by residents. However, the residents' negative pain provocation rate of 39.5% compares with what is reported in the literature.[8]
Concerning procedural observations, the records of CSF and blood aspiration, flashback, and intravascular needle tip placement were less frequent in BCFN notes. For reporting these kinds of observations during TFESI, however, we have no hospital standard, and we cannot exclude retrospective bias. Intravascular penetration caused by residents was generally low and might be explained by the fact that inexperienced interventionalists are known to be less accurate in interpreting contrast dispersal patterns.[18] Thus the absolute rate of these observations could in fact be higher.
Limitations
In addition to the shortcomings of the retrospective design already mentioned, data for DAP were missing in 37.3% of cases. More fluoroscopy parameters such as a record on fluoroscopy time or the total number of shots could have helped to better describe the residents' learning curve. Unfortunately, these parameters could not be retrieved from our records. Although procedure time itself does not necessarily relate to proficiency,[19] it has been used before in assessments of learning curves[12] and represents a fair surrogate marker for the following reasons: Needle repositioning is done blindly most of the time, and bony obstacles such as hypertrophied facet joints and iliac crests are overcome by feeling a loss of resistance. At the beginning of the learning curve, the needle had to be completely withdrawn and the image intensifier readjusted to choose a new entry point (parameters that could also be assessed in future studies); this extra procedure time is not well reflected by fluoroscopy time. Further spinal injections of facet and sacroiliac joints performed by participating residents in a similar manner to TFESI certainly shortened the learning curve. Lastly, comparisons of patients' clinical outcomes after TFESI performed by residents and BCFNs are missing in the present report because they could not be retrieved well enough retrospectively, and some infiltrations were diagnostic, thus interfering with the analysis of longer term success.
#
#
Conclusion
After < 70 TFESIs, the learning curve in terms of procedure time and radiation exposure can be overcome by residents who had never performed this procedure before. No severe complications were encountered during 238 TFESIs performed by residents, and the rate of unsuccessful attempts was 1.7%. At the moment the question whether patients' outcomes are influenced by the interventionalist's training level as well remains unanswered.
#
#
Die Autoren geben an, dass kein Interessenkonflikt besteht.
Acknowledgments
We thank our senior neurosurgeons for the teaching of TFESI and our operating room personnel for their skilled assistance. We also thank Carolin Hock for proofreading the manuscript.
-
References
- 1 Rathmell JP, Benzon HT, Dreyfuss P. , et al. Safeguards to prevent neurologic complications after epidural steroid injections: consensus opinions from a multidisciplinary working group and national organizations. Anesthesiology 2015; 122 (05) 974-984
- 2 Brändle K, Stienen MN, Neff A, Hildebrandt G, Joswig H. Ten-day response to CT-guided spinal infiltration therapy in more than a thousand patients. J Neurol Surg A Cent Eur Neurosurg 2016; 77 (03) 181-194
- 3 Tiegs-Heiden CA, Murthy NS, Geske JR. , et al. Fluoroscopically guided transforaminal epidural steroid injections at a quaternary-care teaching institution: effect of trainee involvement and patient body mass index on fluoroscopy time and patient dose. Clin Radiol 2016; 71 (01) e16-e20
- 4 Rados I, Sakic K, Fingler M, Kapural L. Efficacy of interlaminar vs transforaminal epidural steroid injection for the treatment of chronic unilateral radicular pain: prospective, randomized study. Pain Med 2011; 12 (09) 1316-1321
- 5 Ackerman III WE, Ahmad M. The efficacy of lumbar epidural steroid injections in patients with lumbar disc herniations. Anesth Analg 2007; 104 (05) 1217-1222
- 6 Gharibo CG, Varlotta GP, Rhame EE, Liu EC, Bendo JA, Perloff MD. Interlaminar versus transforaminal epidural steroids for the treatment of subacute lumbar radicular pain: a randomized, blinded, prospective outcome study. Pain Physician 2011; 14 (06) 499-511
- 7 Schaufele MK, Hatch L, Jones W. Interlaminar versus transforaminal epidural injections for the treatment of symptomatic lumbar intervertebral disc herniations. Pain Physician 2006; 9 (04) 361-366
- 8 Manchikanti L, Cash KA, Pampati V, Damron KS, McManus CD. Evaluation of lumbar transforaminal epidural injections with needle placement and contrast flow patterns: a prospective, descriptive report. Pain Physician 2004; 7 (02) 217-223
- 9 Smuck M, Zheng P, Chong T, Kao MC, Geisser ME. Duration of fluoroscopic-guided spine interventions and radiation exposure is increased in overweight patients. PM R 2013; 5 (04) 291-296 ; quiz 296
- 10 R Development Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria. 2013. Available at: http://www.R-project.org/ . Accessed October 24, 2016
- 11 Joswig H, Hock C, Hildebrandt G, Schaller K, Stienen MN. Microscopic lumbar spinal stenosis decompression: is surgical education safe?. Acta Neurochir (Wien) 2016; 158 (02) 357-366
- 12 Joswig H, Richter H, Haile SR, Hildebrandt G, Fournier JY. Introducing Interlaminar full-endoscopic lumbar diskectomy: a critical analysis of complications, recurrence rates, and outcome in view of two spinal surgeons' learning curves. J Neurol Surg A Cent Eur Neurosurg 2016; 77 (05) 406-415
- 13 Stienen MN, Joswig H, Jucker D, Hildebrandt G, Schaller K, Gautschi OP. Anterior cervical discectomy and fusion: is surgical education safe?. Acta Neurochir (Wien) 2015; 157 (08) 1395-1404
- 14 Stienen MN, Smoll NR, Hildebrandt G, Schaller K, Gautschi OP. Early surgical education of residents is safe for microscopic lumbar disc surgery. Acta Neurochir (Wien) 2014; 156 (06) 1205-1214
- 15 Stienen MN, Smoll NR, Tessitore E, Schaller K, Hildebrandt G, Gautschi OP. Surgical resident education in noninstrumented lumbar spine surgery: a prospective observational study with a 4.5-year follow-up. World Neurosurg 2015; 84 (06) 1589-1597
- 16 Joswig H, Gautschi OP, El Rahal A. , et al. Cranioplasty: is surgical education safe?. World Neurosurg 2016; 91: 81-88
- 17 Visco CJ, Kennedy DJ, Chimes GP. , et al. Programmatic design for teaching the introductory skills and concepts of lumbar spine procedures to physiatry residents: a prospective multiyear study. Am J Phys Med Rehabil 2013; 92 (03) 248-257
- 18 Smuck M, Abbott Z, Zemper E. Interpretation of contrast dispersal patterns by experienced and inexperienced interventionalists. PM R 2009; 1 (01) 55-59
- 19 Ramsay CR, Grant AM, Wallace SA, Garthwaite PH, Monk AF, Russell IT. Assessment of the learning curve in health technologies. A systematic review. Int J Technol Assess Health Care 2000; 16 (04) 1095-1108
Address for correspondence
-
References
- 1 Rathmell JP, Benzon HT, Dreyfuss P. , et al. Safeguards to prevent neurologic complications after epidural steroid injections: consensus opinions from a multidisciplinary working group and national organizations. Anesthesiology 2015; 122 (05) 974-984
- 2 Brändle K, Stienen MN, Neff A, Hildebrandt G, Joswig H. Ten-day response to CT-guided spinal infiltration therapy in more than a thousand patients. J Neurol Surg A Cent Eur Neurosurg 2016; 77 (03) 181-194
- 3 Tiegs-Heiden CA, Murthy NS, Geske JR. , et al. Fluoroscopically guided transforaminal epidural steroid injections at a quaternary-care teaching institution: effect of trainee involvement and patient body mass index on fluoroscopy time and patient dose. Clin Radiol 2016; 71 (01) e16-e20
- 4 Rados I, Sakic K, Fingler M, Kapural L. Efficacy of interlaminar vs transforaminal epidural steroid injection for the treatment of chronic unilateral radicular pain: prospective, randomized study. Pain Med 2011; 12 (09) 1316-1321
- 5 Ackerman III WE, Ahmad M. The efficacy of lumbar epidural steroid injections in patients with lumbar disc herniations. Anesth Analg 2007; 104 (05) 1217-1222
- 6 Gharibo CG, Varlotta GP, Rhame EE, Liu EC, Bendo JA, Perloff MD. Interlaminar versus transforaminal epidural steroids for the treatment of subacute lumbar radicular pain: a randomized, blinded, prospective outcome study. Pain Physician 2011; 14 (06) 499-511
- 7 Schaufele MK, Hatch L, Jones W. Interlaminar versus transforaminal epidural injections for the treatment of symptomatic lumbar intervertebral disc herniations. Pain Physician 2006; 9 (04) 361-366
- 8 Manchikanti L, Cash KA, Pampati V, Damron KS, McManus CD. Evaluation of lumbar transforaminal epidural injections with needle placement and contrast flow patterns: a prospective, descriptive report. Pain Physician 2004; 7 (02) 217-223
- 9 Smuck M, Zheng P, Chong T, Kao MC, Geisser ME. Duration of fluoroscopic-guided spine interventions and radiation exposure is increased in overweight patients. PM R 2013; 5 (04) 291-296 ; quiz 296
- 10 R Development Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria. 2013. Available at: http://www.R-project.org/ . Accessed October 24, 2016
- 11 Joswig H, Hock C, Hildebrandt G, Schaller K, Stienen MN. Microscopic lumbar spinal stenosis decompression: is surgical education safe?. Acta Neurochir (Wien) 2016; 158 (02) 357-366
- 12 Joswig H, Richter H, Haile SR, Hildebrandt G, Fournier JY. Introducing Interlaminar full-endoscopic lumbar diskectomy: a critical analysis of complications, recurrence rates, and outcome in view of two spinal surgeons' learning curves. J Neurol Surg A Cent Eur Neurosurg 2016; 77 (05) 406-415
- 13 Stienen MN, Joswig H, Jucker D, Hildebrandt G, Schaller K, Gautschi OP. Anterior cervical discectomy and fusion: is surgical education safe?. Acta Neurochir (Wien) 2015; 157 (08) 1395-1404
- 14 Stienen MN, Smoll NR, Hildebrandt G, Schaller K, Gautschi OP. Early surgical education of residents is safe for microscopic lumbar disc surgery. Acta Neurochir (Wien) 2014; 156 (06) 1205-1214
- 15 Stienen MN, Smoll NR, Tessitore E, Schaller K, Hildebrandt G, Gautschi OP. Surgical resident education in noninstrumented lumbar spine surgery: a prospective observational study with a 4.5-year follow-up. World Neurosurg 2015; 84 (06) 1589-1597
- 16 Joswig H, Gautschi OP, El Rahal A. , et al. Cranioplasty: is surgical education safe?. World Neurosurg 2016; 91: 81-88
- 17 Visco CJ, Kennedy DJ, Chimes GP. , et al. Programmatic design for teaching the introductory skills and concepts of lumbar spine procedures to physiatry residents: a prospective multiyear study. Am J Phys Med Rehabil 2013; 92 (03) 248-257
- 18 Smuck M, Abbott Z, Zemper E. Interpretation of contrast dispersal patterns by experienced and inexperienced interventionalists. PM R 2009; 1 (01) 55-59
- 19 Ramsay CR, Grant AM, Wallace SA, Garthwaite PH, Monk AF, Russell IT. Assessment of the learning curve in health technologies. A systematic review. Int J Technol Assess Health Care 2000; 16 (04) 1095-1108