

Subscribe to RSS
DOI: 10.1055/s-0042-1742507
Desiderata for a New Generation of EHRs for Inclusive Healthcare
Contribution from the IMIA Health Information Systems Working GroupAuthors

Summary
Objectives: This research addresses several factors relevant to inequity in healthcare that may be susceptible to being addressed in a new generation of electronic health records (EHRs).
Methods: Through a scoping review of the literature, inequities related to ethnicity, gender, and socioeconomic aspects in healthcare in general and, more specifically in EHRs, have been considered. Papers have been identified between 2011 and 2022 in three categories: EHR, gender inequalities, and ethnicity inequalities.
Results: Twenty-two recommendations have been identified within the scope of the three categories indicated above. These exposed requirements focus on two spheres: (1) technical sphere, mainly focused on the characteristics and tools that the EHR should develop from taking into account the studied inequalities; and (2) clinical sphere, which mainly affects patients, health professionals, and health providers.
Conclusions: Ethnic and gender inequalities are essential factors to take into account when diagnosing, monitoring, preventing, and treating a patient. These factors give us the keys to discovering recommendations for a new generation of EHRs to help mitigate these needs.
1 Introduction
1.1 Ethnic Inequalities
In recent years, interest in understanding how different forms of racism affect health has been growing. This interest has been triggered by the significant health inequalities of people of different ethnicities at the frontline of the same health system [[1]].
Racism is defined as an organized social system where a dominant racial group classifies people into different social groups called “races” and differentially allocates resources and social opportunities to each inferior group [[2], [3]]. Racism is a significant cause of racial inequalities in health because, as a structured system, it interacts with other social institutions such as political, economic, and legal institutions [[4], [5]]
Del Pino et al. [[6]] propose some strategies to eliminate ethnic health inequalities such as: (1) making integrated efforts to prevent racism from blocking the chances of success, allowing everyone to access resources with equity, and (2) health systems to shift their focus from treating diseases to preventing them, providing quality care, adapted to each patient's culture and needs.
It is also known that for sustainable development to exist, inequalities must be reduced by collecting vital information on each social group, such as gender, ethnicity, and age, among others [[7]].
Despite advances in research and reducing inequalities, African Americans, Native Americans, Native Hawaiians, and other Pacific Islanders have poorer health than the white population [[8]]. Launer et al. [[9]] conclude that, according to statistics, in the United States and the United Kingdom, people with black or brown skin have poorer health than people with white skin and receive poorer quality health care. In Germany, patterns of ethnic inequality in health care use are related to inequalities related to education, income, and work [[10]].
Ethnicity often acts as an independent variable in terms of inequality but can also intersect with other determinants such as social and educational deprivation [[9]]. Ethnicity is a determining factor in using health systems [[10]]. Migrant populations often have different health care needs, preferences, and expectations or face barriers in the use of health services, and this needs to be addressed.
1.2 Gender Inequalities
One of the structural determinants of health inequalities is gender. It determines health behavior, care practices, and health outcomes [[11], [12]].
The World Health Organization (WHO) defines the concept of health inequalities as the different opportunities and resources related to people's health, depending on their social class, gender, territory, or ethnicity, relating a worse state of health to the most disadvantaged groups. It also states that these differences are unnecessary, avoidable, and unfair [[13]]. Rohlfs et al. [[14]] consider that women and men get sick differently and have different lifestyles.
Hay et al. [[15]] propose a set of objectives to make health systems more gender-equitable. They focus on “(1) reflecting and reinforcing a gender-equitable society; (2) addressing gender norms and the root causes of inequalities across the life course; (3) providing equal opportunities for health professionals of all genders to enter, thrive, and progress within health systems; (4) ensure equal access to and use of high-quality health services by people of all genders, without financial, social and geographic barriers; and (5) commit to accountability for addressing gender inequalities at all levels.”
However, despite the efforts made, gender inequity in health persists today [[16]], and health systems remain a fundamental source of these inequalities [[17]].
Studies such as Kennedy et al. [[18]] propose analyzing gender inequalities from adolescence onwards since, from that stage, gender inequalities related mainly to contraception and reproduction are recognized.
Sen et al. [[19]] differentiate between two types of perspectives in the health and gender approach, which are related to each other: (1) biological perspective and (2) social perspective. The latter can be modified through health and social policies.
Most studies agree that health systems need to ensure equity in health care for patients of different genders. Some propose changes in health policies, in the training of health professionals, or in patient education, but there is still no consensus.
1.3 Electronic Health Records
The implementation of electronic health records (EHRs) in the US healthcare system [[20]] and worldwide [[21]] is leading to the rapid growth of data in digital format. This growth offers enormous potential for the use of clinical data beyond patient care. Secondary use of clinical data is defined as “the non-healthcare use of personal health information, including, but not limited to, analytics, research, quality/safety measurement, public health, payment, provider certification or credentialing, and marketing and other activities, including strictly commercial activities” [[22]].
The information contained in the EHR is of great value to: (1) furthering research in clinical informatics, (2) improving clinical practice, and (3) improving healthcare [[23]]. However, EHRs have essential data that cannot be reused, as they do not store the information entirely or store it in a complex format. Studies show that EHRs omit important patient data [[24]] or provide other information in a format that is not machine-processable, complicating data analysis.
This also undermines the analysis and storage of data related to gender and ethnic inequalities, which results in the loss of information on the behavior of these inequalities concerning affected patients and their diseases. Moreover, these data are necessary to combat these inequalities and eradicate them from health systems.
With this situation in mind, we undertook a scoping review of the literature to identify several factors relevant to inequity that are likely to be addressed by implementing a new generation of EHRs to respond to these needs.
2 Materials and Methods
A scoping review method defined below has been designed to identify and extract the relevant information to develop these desiderata.
2.1 Identifying the Information Sources
A search for literature related to the topic of study was conducted in the PubMed database. The search was carried out between 2011 and 2022 for English and Spanish articles to obtain the most recent information on this research. The reason for searching in two languages was to get broader and more diverse information on territorial issues.
A pattern of searching the information was established with different terms, from more general to more specific. The general terms included: (1) Electronic Health Records, (2) EHR, (3) Electronic records, (4) Medical Records, and (5) Patient Records. Subsequently, a search was conducted for more specific terms such as (1) Gender, (2) Ethnics, (3) Gender inequality, (4) Gender inequalities, (5) Ethnicity inequality, (6) Ethnicity inequalities, (7) Inequalities in HER, (8) Socioeconomic inequality, and (9) Socioeconomic inequalities.
Considering the search keywords, a total of 741 articles were detected.
To select the papers, inclusion, and exclusion criteria were defined, detailed in the following section, and the information in each article was further analyzed. Firstly, the titles were analyzed, the abstract was read, and finally, the introduction, discussion, and conclusions. Three iterations were carried out to identify the articles that met the inclusion criteria and classify them into three categories: (1) EHR, (2) Gender inequalities, and (3) Ethnicity inequalities.
2.2 Inclusion and Exclusion Criteria
In order to limit the search for information and the scope of the review to meet the objectives proposed in this research, inclusion and exclusion criteria have been established.
Inclusion criteria:
-
Papers that identify factors in EHRs related to gender or ethnic inequalities and that generate health impact;
-
The importance of good data storage in the EHR to improve clinical care and research is explored;
-
Not all studies presented in each article must have been conducted in the same country;
-
The selected article must be in English or Spanish.
Exclusion criteria:
-
The EHR information discussed in the article does not focus on improving EHR;
-
The article focuses on gender or ethnic inequalities contained in EHRs, but not on their impact on health;
-
Other types of situations that have an impact on health conditioned by EHRs are discussed.
2.3 Extracting the Information
Once the papers that met the inclusion criteria had been identified, the relevant information related to the present research was extracted and classified into the three categories defined in the section “Identifying the information.” A total of 51 references were finally identified.
First, the titles were read, and a first classification was made. Each article was assigned a number within its category within this classification, and its reference was included. As the information contained in each paper was explored in more depth, the information relevant to the present research was extracted. This information was linked to the numbered paper and its reference within the category it had been assigned. If the paper was considered to be classified in another category due to the content, the change was made if there was consensus among the authors.
Based on the results, discussions, and conclusions of the articles identified, a classification was made, and recommendations were drawn.
3 Desiderata
The recommendations proposed by this research are listed below.
3.1 Ethnicity
Several relevant needs have been identified in addressing ethnic inequalities that are addressable from the point of view of EHR design and use. These are represented schematically in [Table 1]:


-
Improving the health of a country's ethnic minorities should not only focus on the needs caused by deficits [[25]] as many are, compared to a region's population, healthier concerning non-communicable diseases such as cancer [[26]]. Moreover, the doctor-patient relationship is often paternalistic for this population, which differs from the type of relationship promoted today that is more consensual between doctor and patient;
-
A reasonable health rate in a particular age group of an ethnic group is not a predictor of good health in the future, i.e., if within a particular ethnic group there is an age range in which there is generally good health, it does not mean that when they change age range, they will continue to be in good health [[27]];
-
Even if ethnic groups established in a region speak the language of that region, healthcare professionals need to adapt information and communication with these patients. This is especially true for those of non-Western ethnic origin [[28]]. Furthermore, it is necessary to provide health education, especially to young adults of diverse ethnic backgrounds;
-
Individualized health care is also necessary for ethnic minorities, and health professionals should consider the risk factors and social needs of ethnic minorities to place greater emphasis on disease prevention [[29]]. In particular, strengthening patient-centered primary care would reduce health inequalities [[30], [31]];
-
Providing access to healthcare for different ethnic groups reduces overall healthcare costs and improves the health of this population [[29]]. In 2017 [[32]], the United States introduced the “Medicare for All Act” initiative to provide a universal right to decent healthcare. Total healthcare costs were reduced by 9.6%;
-
To improve the health of these ethnic minorities is essential for health care providers to encourage contact between these patients and social support services [[6]];
-
Research suggests that racial diversity among health professionals generates a benefit in healthcare [[33]] as health professionals from underrepresented minorities are more likely to work with underserved populations [[34]].
3.2 Gender
-
There is a need to prevent gender inequalities in early adolescence [[35]] by establishing strategies at individual, societal and structural levels [[36]];
-
Quality health care systems must be improved to reduce gender differences by strengthening national legislation and programs [[37] [38] [39]];
-
Provide continuing education courses for health professionals on the relationship between gender differences and health problems to improve healthcare quality. In addition, it would also be good to introduce a subject in medical studies on the relationship between gender and disease [[39] [40] [41]];
-
In the field of infectious diseases, knowing the infectious burden and symptoms present in each gender would be positive for optimal diagnosis, monitoring, and treatment of the disease [[41]];
-
In order to address the problem of inequalities, it is necessary to know: (1) what works, (2) for whom in particular it works, and (3) in what context it works. The more specific the knowledge, the fewer inequalities [[38], [39], [42]];
-
There is a need to know what financial, human, and infrastructural resources are needed to address gender inequality [[38], [39]];
-
Promote the use of data disaggregated by stratifies such as gender in order to address different pathologies [[38]] specifically;
-
The use of different tools EHR-based should be promoted to find out the current needs concerning gender inequalities for health professionals and patients [[38]]. In addition, these tools can provide information on monitoring the results of addressing inequalities.
3.3 EHR
In terms of the needs found to improve the EHR, they are schematically represented in [Table 3]:
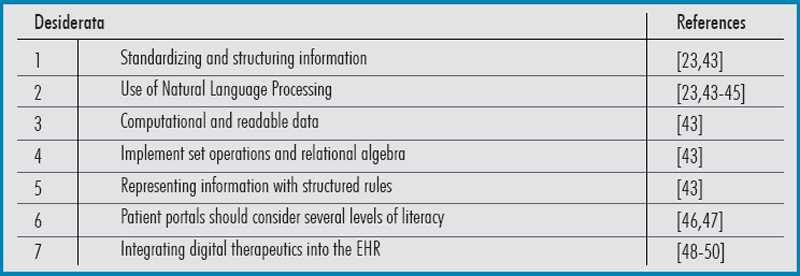
-
Standardization and structuring of the information contained in the EHR would improve the use of information for research and disease management [[23], [43]];
-
The use of NLP allows for decision support by considering variables such as gender and ethnic inequalities, which are often overlooked and highly relevant [[23], [43]]. Furthermore, the application of NLP has proven to help take into account social determinants in clinical decision-making and reduce inequity [[44], [45]];
-
The data contained in the EHR must be human-readable and computational so that they are coupled, and one can be automatically generated from the other [[43]];
-
Implementing set operations and relational algebra will provide crucial information on the influence and relationship of the different inequalities to the diseases suffered by this type of patient [[43]].
-
Representing inequality criteria with structured rules makes it possible to compare information on inequalities and diseases and to support complex workflows that take into account and relate a more significant number of variables [[43]];
-
Portals to EHRs (called patient portals) should be designed to address various levels of digital literacy and health literacy of the patients, thus minimizing the risk of excluding certain groups of the benefits of patient portals. In their Cochrane review, Ammenwerth et al. [[46]] cite the following “In contrast, as a possible adverse eDect, EHR access may increase feelings of confusion and anxiety when patients read clinical information that is unclear to them. In addition, HER access, like many other eHealth solutions, is created for “people like me.” These eHealth solutions, therefore, may only address the needs of “well-educated and well-to-do [wealthy] users rather than the needs of the most disadvantaged in society (the disempowered, disengaged, and disconnected)” [[46]]. For example, a study on the patient portal of Kaiser Permanente Georgia showed that portal users were significantly more likely to be white and to have a higher level of education [[47]].
-
To have digital therapeutics integrated into the EHR to make it more inclusive. Digital Therapeutics Alliance has declared digital therapeutics as “evidence-based therapeutic interventions driven by high-quality software programs to prevent, manage, or treat a medical disorder or disease” [[48]]. Digital therapeutics appears to be well-suited for the delivery of clinical therapies digitally that would usually be delivered in face-to-face encounters with live therapists, such as cognitive-behavioral therapy (CBT), clinical hypnotherapy, or clinical physiotherapy [[49]]. Digital therapeutics facilitates access to the therapies in a more independent environment without being limited to time and other restrictions of a meet-up with the clinician physically. The patients who are suffering from mental health disorders may experience less stigma when treated with digital therapeutics. Digital therapeutics allow more significant levels of granularity when personalizing the treatment. Since it has a history of data, it facilitates the clinicians involved in physical encounters to assess the progress and the outcomes. Digital delivery of therapy ensures consistency of quality throughout the treatment independent of the environmental factors. Digital therapeutics may provide advantages such as ease of access, the convenience of usage, fewer side effects, and cost-effectiveness [[50]]. Hence, the above factors make digital therapeutics a more inclusive method of delivering health care when integrated into EHRs.
4 Discussion
This manuscript aims to expose the unmet needs that exist today concerning gender and ethnic inequalities. It has been shown that ethnic inequalities are closely related to socio-economic inequalities.
These exposed needs focus on two spheres: (1) Technical sphere, mainly focused on the characteristics and tools that the EHR should develop from taking into account the studied inequalities when making a diagnosis, treatment, and follow-up of disease and implement preventive measures for each group, and (2) Clinical sphere, which mainly affects patients, health professionals, and health providers. Several communications and relationship needs are identified about patients, training needs for health professionals, and policy development needs for health providers and health systems.
The study has a series of limitations:
-
Restricted search: the search for information has only been carried out on PubMed when other sources of information can provide relevant data;
-
More specific review methodology: the review method could be improved and, above all, extended. This study could be expanded with a more in-depth analysis comparing countries or regions of the world;
-
Obtaining recommendations has not been developed based on a more systematic methodology (such as a Delphi panel). Instead, it identifies needs to facilitate discussion that will serve to advance the discovery of recommendations for a new generation of EHRs.
5 Conclusions
-
Gender, ethnic and socio-economic differences are determinants that significantly affect patients' health who suffer from them. Some of the problems related to these differences include:
-
Limited access to health services due to lack of financial resources. This leads to delays in diagnosis, lack of preventive measures, and lack of follow-up;
-
Mistrust of health professionals with whom they do not communicate well due to language differences;
-
Lack of health education for patients in this type of situation;
-
Lack of knowledge about the health implications of a patient's gender or ethnicity concerning the disease;
-
Patients generally do not have access to their health information and, if they do, lack of literacy can be an impediment.
The main objective of this research is to highlight the importance of taking into account the gender and ethnicity status of patients when diagnosing, treating, preventing, and monitoring disease. There is a critical need to explore this issue further and to treat these characteristics as a condition for achieving one of the main goals of medicine in recent times (personalized medicine). As is becoming increasingly clear, patients must be studied individually, considering all the factors that affect their health. Ethnic and gender inequalities are essential factors to take into account when diagnosing, monitoring, preventing, and treating a patient.
These factors give us the keys to discovering recommendations for a new generation of EHRs to help mitigate these needs.
No conflict of interest has been declared by the author(s).
-
References
- 1 Williams DR, Lawrence JA, Davis BA. Racism and Health: Evidence and Needed Research. Annu Rev Public Health 2019 Apr 1;40:105-25.
- 2 United Nations Leaving No One Behind. [cited 2022 March 28]. Available from: https://www.un.org/en/desa/leaving-no-one-behind
- 3 Weightman AL, Ellis S, Cullum A, Sander L, Turley RL, editors. Grading Evidence and Recommendations for Public Health Interventions: Developing and Piloting a Framework. London, UK: Health Development Agency; 2005. Project Report.
- 4 Hernández Sampieri R, Fernández Collado C, Baptista Lucio P. In: Metodología de la Investigación. México DF, editor. New York, NY, USA: McGraw-Hill; 2006.
- 5 Gerend MA, Pai M. Social determinants of Black-White disparities in breast cancer mortality: a review. Cancer Epidemiol Biomarkers Prev 2008 Nov;17(11):2913-23.
- 6 Del Pino S, Sánchez-Montoya SB, Guzmán JM, Mújica OJ, Gómez-Salgado J, Ruiz-Frutos C. Health Inequalities amongst People of African Descent in the Americas, 2005-2017: A Systematic Review of the Literature. Int J Environ Res Public Health 2019 Sep 8;16(18):3302.
- 7 United Nations. 2015. Transforming Our World: The 2030 Agenda for Sustainable Development. A/res/70/1. Available from : https://sustainabledevelopment.un.org/post2015/transformingourworld
- 8 Williams DR. Miles to go before we sleep: racial inequities in health. J Health Soc Behav 2012 Sep;53(3):279-95.
- 9 Launer J. Ethnic inequalities in health: should we talk about implicit white supremacism?. Postgrad Med J 2020 Feb;96(1132):117-8.
- 10 Klein J, von dem Knesebeck O. Inequalities in health care utilization among migrants and non-migrants in Germany: a systematic review. Int J Equity Health 2018 Nov 1;17(1):160.
- 11 Shannon G, Jansen M, Williams K, Cáceres C, Motta A, Odhiambo A, et al. Gender equality in science, medicine, and global health: where are we at and why does it matter? Lancet 2019 Feb 9;393(10171):560-9.
- 12 Kapilashrami A. How serious are global health leaders about gender equality? BMJ 2018 Apr 6;361:k1462.
- 13 Whitehead M. The concepts and principles of equity and health. Int J Health Serv 1992;22(3):429-45
- 14 Rohlfs I, Borrell C, Anitua C, Artazcoz L, Colomer C, Escribá V,. La importancia de la perspectiva de género en las encuestas de salud [The importance of the gender perspective in health interview surveys]. Gac Sanit 2000 Mar-Apr;14(2):146-55. Spanish.
- 15 Hay K, McDougal L, Percival V, Henry S, Klugman J, Wurie H, et al. Gender Equality, Norms, and Health Steering Committee. Disrupting gender norms in health systems: making the case for change. Lancet 2019 Jun 22;393(10190):2535-49.
- 16 Payne S. Gender mainstreaming as a global policy paradigm: Barriers to gender justice in health. J Int Comp Soc Policy 2014;30(1):28”40.
- 17 Ruiz-Cantero MT, Tomás-Aznar C, Rodríguez-Jaume MJ, Pérez-Sedeño E, Gasch-Gallén Á. Agenda de género en la formación en ciencias de la salud: experiencias internacionales para reducir tiempos en España [Gender agenda in health sciences education: international experiences to reduce time in Spain]. Gac Sanit 2019 Sep-Oct;33(5):485-90. Spanish.
- 18 Kennedy E, Binder G, Humphries-Waa K, Tidhar T, Cini K, Comrie-Thomson L, et al. Gender inequalities in health and wellbeing across the first two decades of life: an analysis of 40 low-income and middle-income countries in the Asia-Pacific region. Lancet Glob Health 2020 Dec;8(12):e1473-e1488.
- 19 Sen G, George A, Östiln P. Incorporar la perspectiva de género en la equidad en salud: un análisis de la investigación y las políticas. Organización Panamericana de la Salud 2005;(14):6. Washington DC: Harvard Center for population and Development Studies.
- 20 Mosley JD, Van Driest SL, Larkin EK, Weeke PE, Witte JS, Wells QS, et al. Mechanistic phenotypes: an aggregative phenotyping strategy to identify disease mechanisms using GWAS data. PLoS One 2013 Dec 12;8(12):e81503.
- 21 Namjou B, Keddache M, Marsolo K, Wagner M, Lingren T, Cobb B, et al. EMR-linked GWAS study: investigation of variation landscape of loci for body mass index in children. Front Genet 2013 Dec 3;4:268.
- 22 Pathak J, Kiefer RC, Bielinski SJ, Chute CG. Mining the human phenome using semantic web technologies: a case study for Type 2 Diabetes. AMIA Annu Symp Proc 2012;2012:699-708.
- 23 Kennell TI Jr, Willig JH, Cimino JJ. Clinical Informatics Researcher's Desiderata for the Data Content of the Next Generation Electronic Health Record. Appl Clin Inform 2017 Oct;8(4):1159-72.
- 24 Madden JM, Lakoma MD, Rusinak D, Lu CY, Soumerai SB. Missing clinical and behavioral health data in a large electronic health record (EHR) system. J Am Med Inform Assoc 2016 Nov;23(6):1143-9.
- 25 Razum O, Stronks K. The health of migrants and ethnic minorities in Europe: where do we go from here? Eur J Public Health 2014 Oct;24(5):701-2.
- 26 Arnold M, Razum O, Coebergh JW. Cancer risk diversity in non-western migrants to Europe: An overview of the literature. Eur J Cancer 2010 Sep;46(14):2647-59.
- 27 Allik M, Brown D, Dundas R, Leyland AH. Differences in ill health and in socioeconomic inequalities in health by ethnic groups: a cross-sectional study using 2011 Scottish census. Ethn Health 2022 Jan;27(1):190-208.
- 28 Blom IM, Cohen ES, Eshuis LV, Woudstra AJ, Snijder MB, Kunst AE, Fransen MP. Ethnic Differences in Health Literacy Among Young Adults in Amsterdam. Health Lit Res Pract 2018 Nov 5;2(4):e192-e204.
- 29 Williams DR, Cooper LA. Reducing Racial Inequities in Health: Using What We Already Know to Take Action. Int J Environ Res Public Health 2019 Feb 19;16(4):606.
- 30 Starfield B, Gérvas J, Mangin D. Clinical Care and Health Disparities. Annu Rev Public Health 2012;33:89”106.
- 31 Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank Q 2005;83:457”502.
- 32 Pollin R, Heintz J, Arno P, Wicks-Lim J, Ash M. Economic Analysis of Medicare for All. Political Economy Research Institute, University of Massachusetts; Amherst, MA, USA; 2018.
- 33 Cooper LA, Powe NR. Disparities in Patient Experiences, Health Care Processes, and Outcomes: The Role of Patient-Provider Racial, Ethnic, and Language Concordance. Commonwealth Fund (Publication #753); New York, NY, USA; 2004.
- 34 Lightfoote JB, Fielding JR, Deville C, Gunderman RB, Morgan GN, Pandharipande PV, et al. Improving diversity, inclusion, and representation in radiology and radiation oncology part 1: why these matter. J Am Coll Radiol 2014 Jul;11(7):673-80.
- 35 Kågesten A, Gibbs S, Blum RW, Moreau C, Chandra-Mouli V, Herbert A, et al. Understanding Factors that Shape Gender Attitudes in Early Adolescence Globally: A Mixed-Methods Systematic Review. PLoS One 2016 Jun 24;11(6):e0157805.
- 36 John N, Stoenbenau K, Ritter S, Edmeades J, Balvin N. Gender socialization during adolescence in low- and middle-income countries: conceptualization, influences and outcomes. Florence: UNICEF Office of Research-Innocenti; 2017.
- 37 Jonsson PM, Schmidt I, Sparring V, Tomson G. Gender equity in health care in Sweden--minor improvements since the 1990s. Health Policy 2006 Jun;77(1):24-36.
- 38 Sridharan S, Maplazi J, Shirodkar A, Richardson E, Nakaima A. Incorporating gender, equity, and human rights into the action planning process: moving from rhetoric to action. Glob Health Action 2016 Sep 6;9:30870.
- 39 Theobald S, Tolhurst R, Elsey H, Standing H. Engendering the bureaucracy? Challenges and opportunities for mainstreaming gender in Ministries of Health under sector-wide approaches. Health Policy Plan 2005 May;20(3):141-9. Erratum in: Health Policy Plan. 2005 Jul;20(4):265. Standing, Helen [corrected to Standing, Hilary].
- 40 Chavarría MLP, Gosálbez IP. Políticas sanitarias con perspectiva de género. Avances y retrocesos en Cataluña. methaodos. Revista de Ciencias Sociales 2016, 4(2): 225-39.
- 41 Sinha G, Peters DH, Bollinger RC. Strategies for gender-equitable HIV services in rural India. Health Policy Plan 2009 May;24(3):197-208.
- 42 Pawson R, Tilley N, Chelimsky E, Shadish WR. An introduction to scientific realist evaluations. Evaluation for the 21st Century: a handbook. Thousand Oaks, CA: Sage; 1997. p. 405”18.
- 43 Mo H, Thompson WK, Rasmussen LV, Pacheco JA, Jiang G, Kiefer Ret al. Desiderata for computable representations of electronic health records-driven phenotype algorithms. J Am Med Inform Assoc 2015 Nov;22(6):1220-30.
- 44 Reeves RM, Christensen L, Brown JR, Conway M, Levis M, Gobbel GT, et al. Adaptation of an NLP system to a new healthcare environment to identify social determinants of health. J Biomed Inform 2021 Aug;120:103851.
- 45 Wang M, Pantell MS, Gottlieb LM, Adler-Milstein J. Documentation and review of social determinants of health data in the EHR: measures and associated insights. J Am Med Inform Assoc 2021 Nov 25;28(12):2608-16.
- 46 Ammenwerth E, Neyer S, HÖrbst A, Mueller G, Siebert U, Schnell-Inderst P. Adult patient access to electronic health records. Cochrane Database Syst Rev 2021 Feb 26;2(2):CD012707.
- 47 Rigby M, Georgiou A, HyppÖnen H, Ammenwerth E, de Keizer N, Magrabi F, et al. Patient Portals as a Means of Information and Communication Technology Support to Patient- Centric Care Coordination - the Missing Evidence and the Challenges of Evaluation. A joint contribution of IMIA WG EVAL and EFMI WG EVAL. Yearb Med Inform 2015 Aug 13;10(1):148-59.
- 48 Patel NA, Butte AJ. Characteristics and challenges of the clinical pipeline of digital therapeutics. NPJ Digit Med 2020 Dec 11;3(1):159.
- 49 Sverdlov O, van Dam J, Hannesdottir K, Thornton-Wells T. Digital Therapeutics: An Integral Component of Digital Innovation in Drug Development. Clin Pharmacol Ther 2018 Jul;104(1):72-80.
- 50 Guthrie NL, Carpenter J, Edwards KL, Appelbaum KJ, Dey S, Eisenberg DM, et al. Emergence of digital biomarkers to predict and modify treatment efficacy: machine learning study. BMJ Open 2019 Jul 23;9(7):e030710.
Correspondence to:
Publication History
Article published online:
02 June 2022
© 2022. IMIA and Thieme. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Williams DR, Lawrence JA, Davis BA. Racism and Health: Evidence and Needed Research. Annu Rev Public Health 2019 Apr 1;40:105-25.
- 2 United Nations Leaving No One Behind. [cited 2022 March 28]. Available from: https://www.un.org/en/desa/leaving-no-one-behind
- 3 Weightman AL, Ellis S, Cullum A, Sander L, Turley RL, editors. Grading Evidence and Recommendations for Public Health Interventions: Developing and Piloting a Framework. London, UK: Health Development Agency; 2005. Project Report.
- 4 Hernández Sampieri R, Fernández Collado C, Baptista Lucio P. In: Metodología de la Investigación. México DF, editor. New York, NY, USA: McGraw-Hill; 2006.
- 5 Gerend MA, Pai M. Social determinants of Black-White disparities in breast cancer mortality: a review. Cancer Epidemiol Biomarkers Prev 2008 Nov;17(11):2913-23.
- 6 Del Pino S, Sánchez-Montoya SB, Guzmán JM, Mújica OJ, Gómez-Salgado J, Ruiz-Frutos C. Health Inequalities amongst People of African Descent in the Americas, 2005-2017: A Systematic Review of the Literature. Int J Environ Res Public Health 2019 Sep 8;16(18):3302.
- 7 United Nations. 2015. Transforming Our World: The 2030 Agenda for Sustainable Development. A/res/70/1. Available from : https://sustainabledevelopment.un.org/post2015/transformingourworld
- 8 Williams DR. Miles to go before we sleep: racial inequities in health. J Health Soc Behav 2012 Sep;53(3):279-95.
- 9 Launer J. Ethnic inequalities in health: should we talk about implicit white supremacism?. Postgrad Med J 2020 Feb;96(1132):117-8.
- 10 Klein J, von dem Knesebeck O. Inequalities in health care utilization among migrants and non-migrants in Germany: a systematic review. Int J Equity Health 2018 Nov 1;17(1):160.
- 11 Shannon G, Jansen M, Williams K, Cáceres C, Motta A, Odhiambo A, et al. Gender equality in science, medicine, and global health: where are we at and why does it matter? Lancet 2019 Feb 9;393(10171):560-9.
- 12 Kapilashrami A. How serious are global health leaders about gender equality? BMJ 2018 Apr 6;361:k1462.
- 13 Whitehead M. The concepts and principles of equity and health. Int J Health Serv 1992;22(3):429-45
- 14 Rohlfs I, Borrell C, Anitua C, Artazcoz L, Colomer C, Escribá V,. La importancia de la perspectiva de género en las encuestas de salud [The importance of the gender perspective in health interview surveys]. Gac Sanit 2000 Mar-Apr;14(2):146-55. Spanish.
- 15 Hay K, McDougal L, Percival V, Henry S, Klugman J, Wurie H, et al. Gender Equality, Norms, and Health Steering Committee. Disrupting gender norms in health systems: making the case for change. Lancet 2019 Jun 22;393(10190):2535-49.
- 16 Payne S. Gender mainstreaming as a global policy paradigm: Barriers to gender justice in health. J Int Comp Soc Policy 2014;30(1):28”40.
- 17 Ruiz-Cantero MT, Tomás-Aznar C, Rodríguez-Jaume MJ, Pérez-Sedeño E, Gasch-Gallén Á. Agenda de género en la formación en ciencias de la salud: experiencias internacionales para reducir tiempos en España [Gender agenda in health sciences education: international experiences to reduce time in Spain]. Gac Sanit 2019 Sep-Oct;33(5):485-90. Spanish.
- 18 Kennedy E, Binder G, Humphries-Waa K, Tidhar T, Cini K, Comrie-Thomson L, et al. Gender inequalities in health and wellbeing across the first two decades of life: an analysis of 40 low-income and middle-income countries in the Asia-Pacific region. Lancet Glob Health 2020 Dec;8(12):e1473-e1488.
- 19 Sen G, George A, Östiln P. Incorporar la perspectiva de género en la equidad en salud: un análisis de la investigación y las políticas. Organización Panamericana de la Salud 2005;(14):6. Washington DC: Harvard Center for population and Development Studies.
- 20 Mosley JD, Van Driest SL, Larkin EK, Weeke PE, Witte JS, Wells QS, et al. Mechanistic phenotypes: an aggregative phenotyping strategy to identify disease mechanisms using GWAS data. PLoS One 2013 Dec 12;8(12):e81503.
- 21 Namjou B, Keddache M, Marsolo K, Wagner M, Lingren T, Cobb B, et al. EMR-linked GWAS study: investigation of variation landscape of loci for body mass index in children. Front Genet 2013 Dec 3;4:268.
- 22 Pathak J, Kiefer RC, Bielinski SJ, Chute CG. Mining the human phenome using semantic web technologies: a case study for Type 2 Diabetes. AMIA Annu Symp Proc 2012;2012:699-708.
- 23 Kennell TI Jr, Willig JH, Cimino JJ. Clinical Informatics Researcher's Desiderata for the Data Content of the Next Generation Electronic Health Record. Appl Clin Inform 2017 Oct;8(4):1159-72.
- 24 Madden JM, Lakoma MD, Rusinak D, Lu CY, Soumerai SB. Missing clinical and behavioral health data in a large electronic health record (EHR) system. J Am Med Inform Assoc 2016 Nov;23(6):1143-9.
- 25 Razum O, Stronks K. The health of migrants and ethnic minorities in Europe: where do we go from here? Eur J Public Health 2014 Oct;24(5):701-2.
- 26 Arnold M, Razum O, Coebergh JW. Cancer risk diversity in non-western migrants to Europe: An overview of the literature. Eur J Cancer 2010 Sep;46(14):2647-59.
- 27 Allik M, Brown D, Dundas R, Leyland AH. Differences in ill health and in socioeconomic inequalities in health by ethnic groups: a cross-sectional study using 2011 Scottish census. Ethn Health 2022 Jan;27(1):190-208.
- 28 Blom IM, Cohen ES, Eshuis LV, Woudstra AJ, Snijder MB, Kunst AE, Fransen MP. Ethnic Differences in Health Literacy Among Young Adults in Amsterdam. Health Lit Res Pract 2018 Nov 5;2(4):e192-e204.
- 29 Williams DR, Cooper LA. Reducing Racial Inequities in Health: Using What We Already Know to Take Action. Int J Environ Res Public Health 2019 Feb 19;16(4):606.
- 30 Starfield B, Gérvas J, Mangin D. Clinical Care and Health Disparities. Annu Rev Public Health 2012;33:89”106.
- 31 Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank Q 2005;83:457”502.
- 32 Pollin R, Heintz J, Arno P, Wicks-Lim J, Ash M. Economic Analysis of Medicare for All. Political Economy Research Institute, University of Massachusetts; Amherst, MA, USA; 2018.
- 33 Cooper LA, Powe NR. Disparities in Patient Experiences, Health Care Processes, and Outcomes: The Role of Patient-Provider Racial, Ethnic, and Language Concordance. Commonwealth Fund (Publication #753); New York, NY, USA; 2004.
- 34 Lightfoote JB, Fielding JR, Deville C, Gunderman RB, Morgan GN, Pandharipande PV, et al. Improving diversity, inclusion, and representation in radiology and radiation oncology part 1: why these matter. J Am Coll Radiol 2014 Jul;11(7):673-80.
- 35 Kågesten A, Gibbs S, Blum RW, Moreau C, Chandra-Mouli V, Herbert A, et al. Understanding Factors that Shape Gender Attitudes in Early Adolescence Globally: A Mixed-Methods Systematic Review. PLoS One 2016 Jun 24;11(6):e0157805.
- 36 John N, Stoenbenau K, Ritter S, Edmeades J, Balvin N. Gender socialization during adolescence in low- and middle-income countries: conceptualization, influences and outcomes. Florence: UNICEF Office of Research-Innocenti; 2017.
- 37 Jonsson PM, Schmidt I, Sparring V, Tomson G. Gender equity in health care in Sweden--minor improvements since the 1990s. Health Policy 2006 Jun;77(1):24-36.
- 38 Sridharan S, Maplazi J, Shirodkar A, Richardson E, Nakaima A. Incorporating gender, equity, and human rights into the action planning process: moving from rhetoric to action. Glob Health Action 2016 Sep 6;9:30870.
- 39 Theobald S, Tolhurst R, Elsey H, Standing H. Engendering the bureaucracy? Challenges and opportunities for mainstreaming gender in Ministries of Health under sector-wide approaches. Health Policy Plan 2005 May;20(3):141-9. Erratum in: Health Policy Plan. 2005 Jul;20(4):265. Standing, Helen [corrected to Standing, Hilary].
- 40 Chavarría MLP, Gosálbez IP. Políticas sanitarias con perspectiva de género. Avances y retrocesos en Cataluña. methaodos. Revista de Ciencias Sociales 2016, 4(2): 225-39.
- 41 Sinha G, Peters DH, Bollinger RC. Strategies for gender-equitable HIV services in rural India. Health Policy Plan 2009 May;24(3):197-208.
- 42 Pawson R, Tilley N, Chelimsky E, Shadish WR. An introduction to scientific realist evaluations. Evaluation for the 21st Century: a handbook. Thousand Oaks, CA: Sage; 1997. p. 405”18.
- 43 Mo H, Thompson WK, Rasmussen LV, Pacheco JA, Jiang G, Kiefer Ret al. Desiderata for computable representations of electronic health records-driven phenotype algorithms. J Am Med Inform Assoc 2015 Nov;22(6):1220-30.
- 44 Reeves RM, Christensen L, Brown JR, Conway M, Levis M, Gobbel GT, et al. Adaptation of an NLP system to a new healthcare environment to identify social determinants of health. J Biomed Inform 2021 Aug;120:103851.
- 45 Wang M, Pantell MS, Gottlieb LM, Adler-Milstein J. Documentation and review of social determinants of health data in the EHR: measures and associated insights. J Am Med Inform Assoc 2021 Nov 25;28(12):2608-16.
- 46 Ammenwerth E, Neyer S, HÖrbst A, Mueller G, Siebert U, Schnell-Inderst P. Adult patient access to electronic health records. Cochrane Database Syst Rev 2021 Feb 26;2(2):CD012707.
- 47 Rigby M, Georgiou A, HyppÖnen H, Ammenwerth E, de Keizer N, Magrabi F, et al. Patient Portals as a Means of Information and Communication Technology Support to Patient- Centric Care Coordination - the Missing Evidence and the Challenges of Evaluation. A joint contribution of IMIA WG EVAL and EFMI WG EVAL. Yearb Med Inform 2015 Aug 13;10(1):148-59.
- 48 Patel NA, Butte AJ. Characteristics and challenges of the clinical pipeline of digital therapeutics. NPJ Digit Med 2020 Dec 11;3(1):159.
- 49 Sverdlov O, van Dam J, Hannesdottir K, Thornton-Wells T. Digital Therapeutics: An Integral Component of Digital Innovation in Drug Development. Clin Pharmacol Ther 2018 Jul;104(1):72-80.
- 50 Guthrie NL, Carpenter J, Edwards KL, Appelbaum KJ, Dey S, Eisenberg DM, et al. Emergence of digital biomarkers to predict and modify treatment efficacy: machine learning study. BMJ Open 2019 Jul 23;9(7):e030710.