

Subscribe to RSS
DOI: 10.1055/s-0042-1750367
Measurement of the Consultation Duration in Otorhinolaryngology Outpatient Clinics: Comparison between a University Hospital and a City Hospital
Authors


Abstract
Materials and Methods The length of consultation per patient was measured by direct observation at the ear–nose–throat outpatient clinics of one university hospital and one city hospital. The consultation time was measured as follows. Direct consultation time: time spent on history-taking and physical examination of the patients. Indirect consultation time: time spent in charting, preparing treatment/prescription orders, medical, and writing referral letters.
Results The total consultation time length was significantly longer at the university hospital than that at the city hospital, both for the first consultation and the follow-up consultation. For first visits, the ratio of the indirect consultation time to the total consultation time was 49.2% at the university hospital and 24.2% at the city hospital. As for follow-up visits, the indirect/total consultation time ratio was 37.8% at the university hospital 24.2% at the city hospital.
Conclusion Assistance of a medical secretary would be desirable, especially for first consultations at the university hospital, in view of the long indirect consultation times.
Introduction
The long working hours of employed physicians have recently become a social concern, and medical institutions must support further streamlining and improvement of the efficiency of physicians' work. When medical service fees were revised in the fiscal year 2008, “point addition for medical office assistants” was introduced to reduce physicians' workload, and advanced treatment and long-term care hospitals employing medical office assistants (medical clerks) have become eligible to request points for medical office assistants in medical service fees since 2016. However, in terms of hospital management, objective data demonstrating the benefits of the introduction of medical clerks are required. Further, higher revenue is required from increased medical service fees to justify the additional costs associated with the introduction of medical clerks in aspects such as payroll, recruitment, and training.
This study aimed to evaluate the proportion of physicians' work that can be taken over by medical clerks in the otorhinolaryngology outpatient clinics at two hospitals with different patient characteristics and operational systems wherein a university hospital used electronic medical records and a city hospital used the ordering system and paper-based medical records. For this purpose, a medical student at our university measured the time required to perform individual tasks by directly observing the physicians' activities, including what they do as well as say, in examination rooms. The consultation duration and medical service fees for various disease groups in the individual hospitals were tallied to identify which medical services are best suited to the characteristics of each hospital.
This study does not fall under the category of clinical research that requires an ethical review. However, before participating in this study, the medical student who observed the course of medical treatment in examination rooms to take measurements took a class in research ethics and the protection of personal information as a part of the course curriculum.
Materials and Methods
This study included 157 people who visited the otorhinolaryngology outpatient clinic of Tokyo Women's Medical University Hospital (referred to as the university hospital hereafter) or a general hospital in Saitama Prefecture with approximately 200 beds (referred to as the city hospital hereafter) during 15 weekdays in the 22-day period beginning December 1, 2017 for initial/follow-up examinations and test consultation. Among the initial-visit patients in the university hospital and the city hospital, approximately 50 and 30% were referred patients, respectively. Two clinicians accompanied by a third-year medical school student from Tokyo Women's Medical University conducted medical examinations in both the university and city hospitals. The Fujitsu electronic medical record system was used in the otorhinolaryngology department of the university hospital, and the doctors entered disease names and other pertinent information into the system to prepare prescription and treatment orders as well as medical records during each consultation. However, in the otorhinolaryngology department of the city hospital, only the ordering component of the Fujitsu system, identical to the one used in the university hospital, was used for preparing prescription orders by the doctors; medical records and treatment orders were paper-based, and disease names were entered into the system by Medical Administration Division staff on behalf of the doctors.
The medical student recorded the start and end times for each task while directly observing physicians' discourse and actions in the examination rooms. On the basis of the measured time, the following analyses were performed.
Analysis of the Consultation Duration
The consultation duration was divided into two classes as follows:
Direct consultation duration: This is the time spent in the examination room by the physician on conversations with the patient, physical examinations, and other examinations/tests. The time dedicated to conversations with patients included the time required for the physician to guide patients to the testing rooms as well as the time necessary for taking history and describing the condition. Ear and nose examinations, laryngeal endoscopy, and equilibrium function tests were all part of the physical examinations. The direct consultation duration comprised physical examinations, medical record and order form preparation, and other tasks performed while conversing with the patient.
Indirect consultation duration: This is the amount of time a physician spends preparing treatment and prescription orders, medical records, and other documents, such as referral letters, as well as entering disease names into the system.
Total consultation duration: This is the sum of the direct and indirect consultation durations.
Time spent on tasks performed by medical staff other than physicians, such as hearing tests, blood sampling, and intravenous infusion, as well as time spent waiting before and after tests, was not included in the sum of direct and indirect consultation durations.
For initial- and follow-up-visit patients, the total consultation duration per patient and the percentage of indirect consultation duration out of total consultation duration were compared between the university hospital and the city hospital.
The patients were grouped according to diseases as follows: outer/middle ear diseases (e.g., earwax, outer and middle ear diseases, and tubal stenosis), hearing impairment/tinnitus (including facial nerve palsy), nasal allergies, nasal and paranasal sinus diseases other than nasal allergies (e.g., sinusitis and hemostasis for epistaxis), laryngopharyngeal diseases (e.g., inflammation, abnormal sensations in the laryngopharynx, and evaluation of swallowing), taste disorders, head and neck tumors, and vertigo/dizziness disorders.
The total consultation duration, medical service fee points, and medical service fee points per minute were calculated for the disease groups in which at least five patients were cared for in each hospital to determine whether there were specific tendencies in those hospitals and disease groups.
Excel for windows 10 and JMP Pro 16.0.0 Microsoft Windows 10 were used for the analysis. Total consultation duration and medical service fees per consultation duration were compared using analysis of variance and Tukey's Honest Significant Difference test, whereas percentage of indirect consultation duration was compared using the χ2 test and residual analysis. In all comparisons, a p-value of <0.05 was considered statistically significant.
Results
Comparisons of the Consultation Duration between the Initial and Follow-Up Visits and between the Two Hospitals
Comparisons of the Total Consultation Durations
The total consultation duration per initial-visit patient (mean ± 2 standard deviation) was 11 minutes and 48 seconds ± 8 minutes and 28 seconds (maximum: 33 minutes and 50 seconds) for the university hospital and 6 minutes and 57 seconds ± 3 minutes and 43 seconds (maximum: 7 minutes and 39 seconds) for the city hospital. Successively, the total consultation duration per follow-up patient was 10 minutes and 41 seconds ± 7 minutes and 36 seconds (maximum: 40 minutes and 40 seconds) for the university hospital and 3 minutes and 17 seconds ± 1 minute and 28 seconds (maximum: 6 minutes and 39 seconds) for the city hospital. The total consultation durations per initial-visit patient and per follow-up-visit patient for the university hospital were significantly longer than those recorded per follow-up-visit patient for the city hospital. For both the university and city hospitals, there were no significant differences between the total consultation duration per initial-visit patient and per follow-up-visit patient; however, the total consultation duration per initial-visit patient tended to be longer for the city hospital (see [Fig. 1]).

Comparisons of the Percentage of Indirect Consultation Duration
The percentage of indirect consultation duration for university hospital initial-visit patients did not differ significantly from that recorded for university hospital follow-up-visit patients; however, it was significantly higher than that observed for city hospital initial-visit patients. For the university hospital, the direct and indirect consultation durations per initial-visit patient were 5 minutes and 59 seconds ± 5 minutes and 10 seconds and 5 minutes and 48 seconds ± 4 minutes and 26 seconds, respectively; the indirect consultation duration accounted for 49.2% of the total consultation duration. The direct and indirect consultation durations per follow-up patient were 6 minutes and 39 seconds ± 9 minutes and 28 seconds and 4 minutes and 3 seconds ± 7 minutes and 38 seconds, respectively; the indirect consultation duration accounted for the remaining 37.8% of the total consultation duration.
In the city hospital, the direct and indirect consultation durations per initial-visit patient were 5 minutes and 16 seconds ± 1 minute and 2 seconds (maximum: 5 minutes and 26 seconds) and 1 minute and 41 seconds ± 26 seconds (maximum: 2 minutes and 58 seconds), respectively, and the indirect consultation duration accounted for 24.2% of the total consultation duration. The direct and indirect consultation durations per follow-up patient were 2 minutes and 16 seconds ± 1 minute and 1 second (maximum: 5 minutes and 26 seconds) and 1 minute and 1 second ± 1 minute and 1 second (maximum: 2 minutes and 58 seconds), respectively; the indirect consultation duration accounted for 31.1% of the total consultation duration. The percentages of indirect consultation duration for both initial- and follow-up-visit patients at the city hospital were significantly lower than those of the patients at the university hospital, and the percentage of indirect consultation duration for follow-up patients was significantly lower than that recorded for initial-visit patients of the city hospital (see [Fig. 2]).

Comparisons of Medical Service Fee Points and Medical Service Fee Points per Consultation Duration between the Two Hospitals and between Different Disease Groups
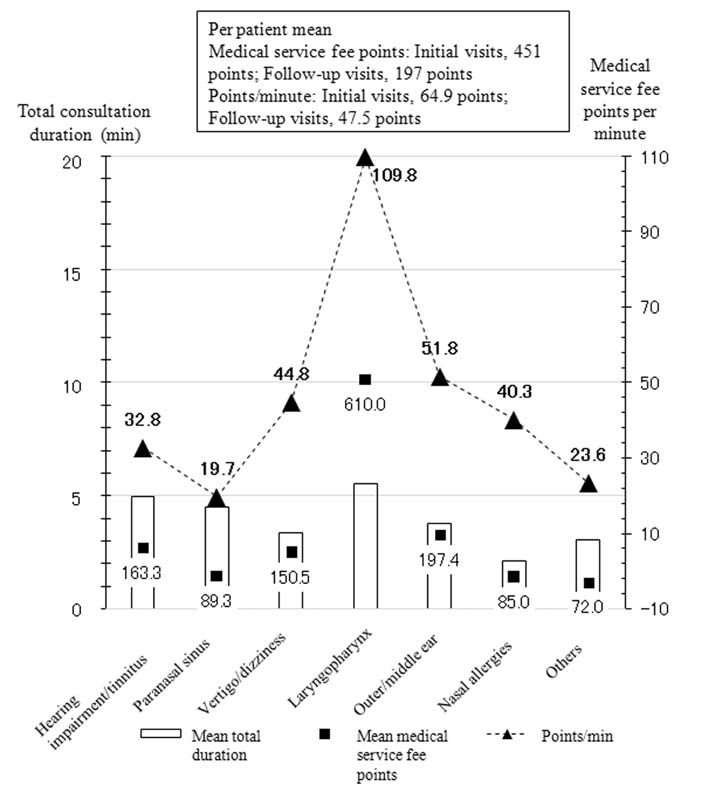
The mean medical service fee points per patient per minute of total consultation duration were 749/63.6 and 316.8/29.6 points for initial- and follow-up-visit patients of the university hospital, respectively, and 451/64.9 and 196.8/47.5 points for initial- and follow-up-visit patients of the city hospital, respectively. The number of medical service fee points per minute for follow-up patients at the university hospital was significantly lower than that for initial-visit patients at the university hospital; furthermore, no significant differences in medical service fee points per minute were found between initial-visit patients at the university hospital, initial-visit patients at the city hospital, and follow-up patients at the city hospital.
Medical service fee points and the total consultation duration for different disease groups in the university hospital are shown in [Fig. 3]. The total consultation duration was longest for head and neck tumors (16 minutes and 40 seconds), followed by vertigo/dizziness disorders (14 minutes and 13 seconds) and hearing impairment/tinnitus (13 minutes and 1 second); successively, it was shortest for the allergic rhinitis group (4 minutes and 37 seconds). The number of medical service fee points was highest for hearing impairment/tinnitus (535.8 points), followed by nasal and paranasal sinus diseases (547.7 points) and vertigo/dizziness disorders (53.8 points); however, it was lowest for nasal allergies (165.3 points). Factors contributing to the increased medical service fee points included hearing and equilibrium function tests that were performed at the request of other hospitals on patients in the hearing impairment/tinnitus and vertigo/dizziness groups as well as endoscopic examinations that were performed preoperatively and postoperatively on patients with nasal and paranasal sinus diseases on a routine basis. In contrast, the number of medical service fee points for nasal allergies was low because many patients required only prescriptions.

The number of medical service fee points per minute for the nasal and paranasal sinus disease group was significantly higher (53.1 points/min). Moreover, the medical service fee points per minute for hearing impairment/tinnitus (45.0 points/min) and laryngopharyngeal diseases (41.3 points/min) tended to be higher because hearing and endoscopic examinations were performed on patients with these diseases. Patients with head and neck tumors had the lowest number of medical service fee points per minute (14.7 points/min) because they came to the hospital throughout the research period primarily to be informed about test results and treatment options and were only charged for the consultation. Meanwhile, the number of points was lowest but the number of points per minute was second highest (35.8 points/min; only for vertigo/dizziness disorders) for patients visiting for nasal allergies because the consultation duration was short.
The data obtained for the city hospital are shown in [Fig. 4]. Both the medical service fee points and medical service fee points per minute tended to be higher for laryngopharynx diseases (610.0 points and 109.8 points/min, respectively), for which many endoscopic examinations were performed. The number of medical service fee points for paranasal sinus diseases was low, unlike that observed for the university hospital, because many patients in this group visited the hospital only to receive nebulizers. The differences among the other disease groups were not as pronounced as those observed at the university hospital.
Discussion
This study showed that the indirect consultation duration accounted for approximately half of the total consultation duration for initial-visit patients at the university hospital (mean percentage of indirect consultation duration: 49.2%), whereas the percentage of indirect consultation duration was only 24.2 and 31.1% for initial- and follow-up-visit patients of the city hospital, respectively. Moreover, the total consultation duration for both initial- and follow-up-visit patients of the university hospital was significantly longer than the total consultation duration for follow-up-visit patients of the city hospital. These results suggest that hiring medical clerks to take over indirect consultation tasks can significantly contribute to the improvement of the efficiency of medical services in the university hospital. As the current study compared the data of two physicians during their work hours in a university hospital and a city hospital, the data do not represent the tendencies of physicians of university and city hospitals in general. Nevertheless, the data obtained in the present study are useful as they were actual measurements, which are more reliable than the data from common questionnaire surveys.
According to a survey of hospital doctors' working conditions done in fiscal year 2017,[1] hospital doctors spent approximately 4 hours per week on consultation-related office work, accounting for approximately 20% of the total consultation duration. The office work is mostly related to outpatient consultations. Surgeons spent 55.6, 16.7, and 9.7% of day-shift hours (barring hours spent in operating rooms and laboratories) in outpatient clinics, nurse stations, and patient rooms, respectively, according to a study in which working hours and associated tasks of surgeons were directly observed.[2] Although the otorhinolaryngology department in which the present study was conducted is a surgical department, it deals with medical diseases, such as vertigo and dizziness. Therefore, otorhinolaryngologists' time spent on outpatient consultations and tasks that can be performed by medical clerks is probably comparable to, if not greater than, that of doctors in other surgery-related fields.
The introduction of medical clerks has been reported to be effective in reducing doctors' workload in both wards and outpatient clinics. In terms of ward tasks, a satisfaction survey of emergency room doctors about medical clerks assigned full-time roles to a university hospital's otorhinolaryngology critical care center revealed high levels of satisfaction with their assistance in clinical tasks, such as document preparation (such as medical certificate preparation and document management), consent form preparation and informed consent, and entering information into electronic medical records.[3] In terms of a specific workload-reducing effect, the survey revealed that medical clerks obtained 1,564 consent forms on behalf of doctors in a year, indicating that the doctors' work was decreased by approximately 130 hours, assuming that each consent form took 5 minutes to complete.
The effects of introducing medical clerks in outpatient services have been reported in detail by Makito et al at the Department of Otorhinolaryngology, Kitasato University.[4] The results of their questionnaire survey of doctors as well as analyses of consultation durations, hours assisted by medical secretaries (medical clerks), and medical service fee points requested in insurance claims showed decreases in overtime hours for doctors and nurses in addition to a reduction in the workload of doctors. Furthermore, regarding insurance claims, medical clerks reduced input omissions by 27% because inadvertent omissions by doctors caused by “carelessness and lack of time” were reduced. The effects of introducing medical clerks were not directly measured. However, this study showed that the percentage of indirect consultation duration was significantly lower in the city hospital, where nurses took over the doctors' clerical tasks, thereby, allowing the doctors to consult a greater number of patients, although 30% of first-visit patients were referred patients and some patients were with a complex medical course.
However, only a limited number of medical institutions currently employ medical clerks. Approximately only 30% of all medical institutions used the point addition for medical office assistants as of fiscal year 2018, with 2,828 medical institutions registered as using it. Regarding the effects of introducing medical clerks, according to the “Fact-Finding Survey on Medical Office Assistants” report[5] of the NPO Japanese Society of Medical Office Assistants, although most responses were positive (e.g., reduced physicians' clerical workloads, reduced burdens on nurses and other medical professionals, and better working environment), 208 of 1,686 institutions providing valid responses did not introduce or stopped staffing medical clerks for various reasons, such as difficulty in recruiting and the institution not meeting the approval criteria for point addition for medical office assistants. It was difficult to recruit medical clerks because of the varied levels of individual medical clerk proficiencies because the education system and career paths for medical clerks were not established and most medical clerk positions (particularly in public hospitals) had irregular and unstable working conditions. Therefore, the popularization of medical clerks requires the following conditions: the development of appropriate institution criteria; establishment of an educational system for medical clerks; and improvement of pay, benefits, and work conditions.
The comparisons of medical service fee points and medical service fee points per minute of consultation duration between the two hospitals showed that the medical service fee points per minute for initial-visit patients of the university hospital did not differ significantly from those of the city hospital. Moreover, medical service fee points per minute for follow-up visit patients of the university hospital were significantly lower than those of the city hospital. These findings suggest that if patients are immediately referred back to their family doctors after the university hospital has established a diagnosis and treatment plan, the university hospital will profit more. The results are also consistent with the national policy of differentiating outpatient care functions between large hospitals and smaller hospitals/clinics.
Both the university and city hospitals had high medical service fee points per minute of consultation duration for disease groups involving endoscopic examinations, such as paranasal sinus and laryngopharyngeal diseases. Because of the coronavirus disease 2019 (COVID-19) outbreak that started in March 2020, followed by the pediatrics department, the otorhinolaryngology department experienced the second-largest profit decrease.[6] Although the decrease is thought to be primarily due to a reduction in overall infections and the avoidance of hospital visits related to COVID-19 measures, a reduction in patients undergoing endoscopy could have been a contributing factor.
Regarding disease-specific tendencies, the medical service fee points per minute for vertigo/dizziness did not differ significantly from those for other disease groups because the total consultation duration for vertigo/dizziness was long in the university hospital; however, many hearing and equilibrium function tests were performed. Successively, as doctors spent time conversing with patients rather than performing tests or procedures, the number of medical service fee points per minute of follow-up consultation for head and neck tumors was low. To respect patients' right to make their own decisions and avoid patient–doctor conflicts, the importance of having adequate communication has recently increased. Thus, the time dedicated to patient–doctor conversation was considered to have medical relevance.
Conclusion
We measured the time taken for outpatient consultations in the otorhinolaryngology department of a university hospital and a city hospital. The indirect consultation duration accounted for approximately half (49.2% on average) of the total consultation duration for university hospital initial-visit patients, whereas it accounted for only 24.2% of the consultation duration for city hospital initial-visit patients. In the university hospital, medical clerks and other staff who can take over physicians' indirect tasks were considered effective in improving the efficiency of clinical services, particularly of outpatient services for initial-visit patients. High medical service fee points per unit consultation duration were noted for paranasal sinus and laryngeal diseases in the university and city hospitals, respectively, because many endoscopic examinations were conducted. However, low medical service fee points per unit consultation time were noted for head and neck diseases in the university hospital because adequate time was spent on conversations with patients.
Conflict of Interest
None declared.
Acknowledgments
This study was conducted as part of the 2017 Medical School Third-Year (Segment 6) Research Project of our university. We thank Dr. Yukako Seo from the Department of Otorhinolaryngology for allowing our student to observe outpatient consultations; Ms. Mao Iino, who was a third-year medical student, for performing the measurements; Dr. Hiroki Fujieda, the Chairman, and members of the Research Project Education Committee for planning and coordinating the project; and Dr. Emiri Sato for reviewing the abstract in English.
-
References
- 1 Ministry of Health. Labour and Welfare. The Eighth Review Meeting on Work Style Reform for Doctors, Information Material 4 (July 9, 2018). A survey on working conditions of hospital doctors (time steady study). Updated 2018. Accessed July 13, 2021 at: https://www.mhlw.go.jp/content/10800000/000331107.pdf
- 2 Seiki K, Tsunetoshi I, Hironobu O. et al. A study of Japanese doctors' working time. Jpn J Health Econ Policy 2009; 21: 39-54
- 3 Shino K, Asami I, Emi I. et al. The usefulness of medical clerk who support doctor's office work in our emergency medical center. Hakodate Med J 2020; 44: 37-42
- 4 Makito O, Hajime S, Hisako A. et al. Practicality of medical secretaries at university hospitals: impact on the electronic medical records system. Kitasato Med 2013; 43: 51-59
- 5 Japanese Society of Medical Office Assistants. Report on results of “fact-finding survey on medical office assistants.” Updated 2020. Accessed July 13, 2021 at: http://ishijimu.umin.jp/kenkyuukaikara/2018tyousa/houkoku.pdf
- 6 Japan Medical Association. Effects of coronavirus disease 2019 on management of clinics July–August 2020. Updated 2020. Accessed July 13, 2021 at: https://www.med.or.jp/dl-med/teireikaiken/20201105_2.pdf
Address for correspondence
Publication History
Received: 12 August 2021
Accepted: 26 November 2021
Article published online:
14 July 2022
© 2022. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Ministry of Health. Labour and Welfare. The Eighth Review Meeting on Work Style Reform for Doctors, Information Material 4 (July 9, 2018). A survey on working conditions of hospital doctors (time steady study). Updated 2018. Accessed July 13, 2021 at: https://www.mhlw.go.jp/content/10800000/000331107.pdf
- 2 Seiki K, Tsunetoshi I, Hironobu O. et al. A study of Japanese doctors' working time. Jpn J Health Econ Policy 2009; 21: 39-54
- 3 Shino K, Asami I, Emi I. et al. The usefulness of medical clerk who support doctor's office work in our emergency medical center. Hakodate Med J 2020; 44: 37-42
- 4 Makito O, Hajime S, Hisako A. et al. Practicality of medical secretaries at university hospitals: impact on the electronic medical records system. Kitasato Med 2013; 43: 51-59
- 5 Japanese Society of Medical Office Assistants. Report on results of “fact-finding survey on medical office assistants.” Updated 2020. Accessed July 13, 2021 at: http://ishijimu.umin.jp/kenkyuukaikara/2018tyousa/houkoku.pdf
- 6 Japan Medical Association. Effects of coronavirus disease 2019 on management of clinics July–August 2020. Updated 2020. Accessed July 13, 2021 at: https://www.med.or.jp/dl-med/teireikaiken/20201105_2.pdf