

Subscribe to RSS
DOI: 10.1055/s-0042-1755584
Are Clinical Pilates Exercises an Effective Treatment for Scoliosis? A Randomized Clinical Trial
Authors
Funding None.

Abstract
Objectives The aim of the study was to investigate the effectiveness of clinical Pilates exercises in patients with idiopathic scoliosis.
Materials and Methods The study included patients aged 15 to 30 years with adolescent idiopathic scoliosis. Patients were randomly separated into the following two groups: the clinical Pilates exercise group (n = 16) and the control group (n = 18). The clinical Pilates exercise group received 16 sessions of exercise. Angle of trunk rotation (scoliometer), sagittal plane alignment of the spine (inclinometer), posture (PostureScreen Mobile program), quality of life (Scoliosis Research Society-23), pain (Numerical Pain scale), and cosmetic deformity perceptions (spinal appearance questionnaire) were assessed twice.
Statistical Analysis Data obtained in the study were analyzed statistically using IBM, SPSS v. 22 software. The Shapiro–Wilks test was used to assess the conformity of data to normal distribution. In the group comparisons of angle of rotation, kyphosis and lordosis angle, and anterior shift values obtained at baseline and in the 8th week, the independent sample t-test were applied to variables with normal distribution, and the Mann–Whitney U test to variables not showing normal distribution.
Results The change in the pain score from baseline to 8 weeks was determined to be significantly superior in the Pilates group (p < 0.001). A statistically significant difference was determined between the groups in respect of the amount of change in the side shift and tilt measurements in the posture evaluation, with superior improvement seen in the Pilates exercise group(p < 0.005).
Conclusions The results of this study showed that Pilates exercises did not have a significant effect on deformity, quality of life, and perception of deformity in scoliosis, but significantly reduced back and low back pain and contributed to improvements in posture.
Introduction
Currently, the indications for idiopathic scoliosis treatment largely depend on the magnitude of the curvature angle evaluated with the Cobb method on an anterior–posterior X-ray, and the treatment consists of exercise, braces, and surgical management.[1]
Exercise treatment for scoliosis management can be grouped as physiotherapeutic scoliosis-specific exercises (PSSE) and general therapeutic exercises. The word “specific” within the phrase PSSE is used to describe exercises that are designed for the treatment of patients with scoliosis.[1] [2] General exercise approaches used in the treatment of scoliosis include strengthening, stretching, mobilization, machine-assisted exercises, posture and postural correction exercises, and low-impact exercises such as Pilates, yoga, or Tai Chi to improve trunk flexibility and strength.[1] [3] [4] [5] [6]
“The Pilates Method” is an exercise system developed by Pilates in 1921. Its philosophy integrates the mind with the musculoskeletal system. In addition to the practice of Pilates by healthy individuals, “Clinical Pilates Exercises” are used by physiotherapists for rehabilitation purposes in different disease groups. Clinical Pilates Exercises, which are used in neuromuscular re-education and functional activity training in physiotherapy, are widely used for the stimulation of blood circulation, improvement of flexibility, muscle endurance and strength, postural adaptation, and body awareness.[7] [8] [9] [10] [11] [12]
Some researchers and clinicians have suggested that Pilates exercises would be a successful exercise method in scoliosis treatment.[8] [13] [14] [15] To the best of our knowledge, there is only one randomized controlled study in the English language that has investigated the effectiveness of Pilates in scoliosis rehabilitation.[13] However, in that study, the mean Cobb angles of the cases were < 10 degrees.[13] This angle of curvature is not even suitable for the definition/ diagnosis of scoliosis.[16]
The aim of this study was to investigate the effects of clinical Pilates exercises used in the clinics and recommended to patients with idiopathic scoliosis on the angle of trunk rotation, sagittal plane alignment of the spine, posture, quality of life, pain, and cosmetic deformity perceptions.
Materials and Methods
Design
A randomized controlled trial was designed to investigate the effects of clinical Pilates exercises in patients with adolescent idiopathic scoliosis. Patients were asked to select a number in a sealed envelope that included random numbers generated via the
“Research Randomizer” program[17] for the randomization process by the second author, and the patients were separated into the following two groups: the clinical Pilates exercise group and the control group. Patients in the control group were informed that after the study ended, they could be included in the same treatment program if they so wished.
Participants
The study included patients aged 15 to 30 years with adolescent idiopathic scoliosis who presented at the Orthopedics and Traumatology Clinic and the Physical Medicine and Rehabilitation Clinic, Fatih Sultan Mehmet Training and Research Hospital, between July and December 2019. Approval for the study was granted by the Ethics Committee of Marmara University Medical Faculty. Written and verbal informed consent was obtained from all participants, or the parents of those aged < 18 years.
Patients were excluded from the study if they had non-idiopathic scoliosis, neurological, muscular or rheumatic diseases, a history of lower extremity or spinal surgery, a history of cancer, if they had any congenital deformity, mental problems, or contraindications to exercise, were receiving another treatment for scoliosis during the study period, or were pregnant.
Procedures
All assessments were applied twice, first before the treatment program and then at 8 weeks when the treatment program was completed.
A Bunnell scoliometer was used to measure the angle of trunk rotation (ATR) and maximum values were recorded.[18]
Posture was evaluated with the PostureScreen Mobile program (PSM) (PostureCo, Inc., Trinity, FL, USA).[19] This is a new, easy, fast, and inexpensive application that has strong rater reliability and preliminary evidence of construct validity, and which allows posture assessment in different environments. Anterior and lateral images of the patients were taken using an iPhone camera. The shift and tilt values of the head, shoulders, ribs, and hips were evaluated on the anterior images and the shift and tilt values of the head, shoulders, hips, and knees on the lateral images. The total shift and tilt values obtained from both images were recorded.[19] [20]
In the measurement of thoracic kyphosis and lumbar lordosis, a gravity-dependent inclinometer (Baseline Bubble Inclinometer) was used, the reliability of which has been demonstrated in a previous study.[21] For thoracic kyphosis, the feet of the inclinometer were placed in the “T1–T2” and “T12–L1” vertebral processes determined by palpation, and measurements were made in the position where the patient felt most comfortable. The kyphosis angle was obtained as the total of these values. To measure lumbar spine lordosis, the inclinometer was placed in “T12–L1” and “S1–S2” vertebral processes and measurements were made in the position where the patient was comfortable. The lordosis angle was obtained as the total of these values.[21]
The Scoliosis Research Society-23 (SRS-23) questionnaire was used to evaluate the quality of life. This scale is a disease-specific quality of life scale consisting of 23 items in five subgroups of pain, self-image, function, mental health, and treatment satisfaction. Each item is scored between 0 (worst) and 5 (best).[22]
The spinal appearance questionnaire (SAQ) is a valid measure of self-image, and was used to assess the participants' perception of various aspects of spinal deformity.[23] The SAQ consists of 11 visual items and 22 questions about the patient's expectations. The 11 visual items consist of drawings showing the severity of various spinal deformity components. Each question is scored as minimum “1” and maximum “5,” with a higher score indicating a poor perception of the deformity. The SAQ can be completed by patients or their parents.[23] In this study, the patients' perception of themselves was assessed.
Back pain was assessed with an 11-point numerical pain scale (NPRS) (0 as “no pain” and 10 as “worst pain possible.” Patients were asked to mark the maximum pain level felt in the last week on the scale.[24]
Exercise Program
The patients were randomly separated into groups as the Pilates exercise and control groups. The clinical Pilates exercise program was administered to the patients in group sessions by a certified and experienced physiotherapist. An individual session was applied to all participants and the basic principles of clinical Pilates were taught, then patients received group exercises that consisted of a maximum of 10 patients under the supervision of the physiotherapist. The patients received 16 sessions in the exercise program, 2 sessions a week for 8 weeks. Each 60-minute group exercise session consisted of 10 minutes of warm-up, 10 minutes of cool-down exercises, and 40 minutes of bilateral clinical pilates exercises aimed at strengthening the global muscles ([Table 1]). A total of 15 to 20 exercises were taught during the 8-week period. Patients were asked to perform the exercises once a day at home on the days they did not attend the clinic. No exercise was recommended to patients in the control group and they were asked to continue their normal lives.
Statistical Analysis
Data obtained in the study were analyzed statistically using IBM, SPSS v. 22 software. The Shapiro–Wilk test was used to assess the conformity of data to normal distribution. Fisher's exact test was used to analyze the gender distribution in the groups and the Pearson chi-square test was used to analyze the curve type distribution. In the group comparisons of angle of rotation, kyphosis, and lordosis angle, and anterior shift values obtained at baseline and in the 8th week, the independent sample t-test were applied to variables with normal distribution, and the Mann–Whitney U test to variables not showing normal distribution. The Mann–Whitney U test was also applied to compare the differences between the groups in respect of the changes obtained after the treatment. The correlation between pain and other parameters was analyzed with Spearman's correlation analysis. A value of p < 0.05 was considered to be statistically significant for the two-tailed tests.
Results
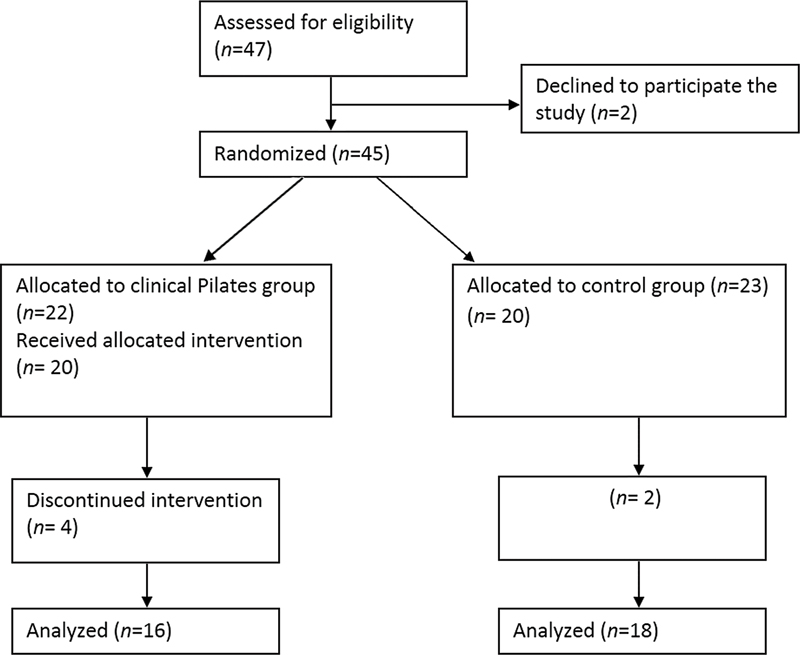
The study included 34 patients with idiopathic scoliosis ([Fig. 1]), with 16 in the clinical Pilates exercise group and 18 in the control group. No patient wore a brace or received any other treatment.
The groups had similar demographic and clinical characteristics at baseline ([Table 2]). There was a significant difference between the two groups in the comparison of mean pain scores at 8 weeks ([Table 2]). The change in the pain score from baseline to 8 weeks was determined to be statistically significantly greater in the Pilates exercise group compared with the control group (p < 0.001) ([Table 2]).
Abbreviations: SD, standard deviation; SAQ, spinal appearance questionnaire; SRS-23, Scoliosis Research Society-23.
a:Mann–Whitney U test.
b: Fisher's exact test.
c: Chi-square test.
d: Independent sample t-test.
A statistically significant difference was determined between the groups in respect of the amount of change in the side shift and side tilt measurements in the posture evaluation after the treatment program, with greater improvement seen in the Pilates exercise group (p < 0.005, [Table 3]) The Pilates exercise and control group were similar in terms of the differences obtained in the other clinical measurements.
|
Parameter |
Clinical Pilates group (n = 20) Mean ± SD |
Control group (n = 20) Mean ± SD |
p-Value[a] |
|
|---|---|---|---|---|
|
Angle of trunk rotation |
−0.7 ± 3.4 |
0.2 ± 2.9 |
0.484 |
|
|
Sagittal plane assessment |
Thoracic kyphosis angle |
2.8 ± 6.3 |
1.8 ± 5.7 |
0.506 |
|
Lumber lordosis angle |
−3.0 ± 8.6 |
−0.2 ± 6.8 |
0.220 |
|
|
Posture assessment |
Anterior shift |
−1.9 ± 11.7 |
5.0 ± 10 |
0.088 |
|
Anterior tilt |
−1.0 ± 4.5 |
0.6 ± 4.1 |
0.347 |
|
|
Side shift |
−2.5 ± 4.8 |
1.9 ± 5.9 |
0.012 |
|
|
Side tilt |
−1.8 ± 2.1- |
0 ± 1.5 |
0.005 |
|
|
Pain score |
−3.0 ± 1.8 |
−0.3 ± 1.7 |
< 0.001 |
|
|
SRS-23 total score |
0.3 ± 0.2 |
0.1 ± 0.2 |
0.117 |
|
|
SAQ |
−2.1 ± 15.1 |
−1.5 ± 15.4 |
0.621 |
|
Abbreviations: SD, standard deviation; SAQ, spinal appearance questionnaire; SRS-23, Scoliosis Research Society-23.
a Mann–Whitney U test.
A total of 93.8% of the patients in the exercise group and 94.4% of the patients in the control group reported back and low back pain, respectively. No correlation was found between the severity of pain and Cobb angle, ATR, kyphosis, and lordosis angles.
Discussion
The results of this study showed that clinical Pilates exercises applied as group exercise for 8 weeks reduced pain in patients with adolescent idiopathic scoliosis and contributed to improving posture.
The foundation principles of Pilates include breath, concentration, center, control, precision, and flow. Static and dynamic body alignments are important and should improve in Pilates. Many Pilates exercises are designed to strengthen the powerhouse, or core, can be described as the area from the bottom of the rib cage to a line across the hip joints in the front and to the buttocks in the back. The most vital muscle groups are the abdominals, spinal extensors, iliopsoas, and quadratus lumborum.[25]
In studies where more than one treatment program has been applied to patients, it is difficult to determine which treatment program resulted in the changes obtained. The advantage of the current study is that the control group received no treatment and the intervention group only received Pilates exercises. To the best of our knowledge, there is only one randomized controlled study in the literature that has investigated the effectiveness of clinical Pilates exercises, which are frequently recommended for scoliosis patients in clinical practice. However, in that research, the mean Cobb angle of the exercise group was 7.6 degrees and the mean Cobb angle of the control group was 7.1 degrees.[13] Therefore, the present study may be considered the first randomized controlled study on this topic. To the best of our knowledge, it is the first study to examine the effect of Pilates exercises on the sagittal plane. The exercises were supervised by a single experienced physiotherapist.
The limitations of the study were the lack of long-term evaluation of the effectiveness of the Pilates exercise program, and that the Cobb angle, which is still considered as the gold standard for assessing the severity of scoliosis, was not used as an outcome measurement. However, ATR is an indicator of the deformity and has been previously shown to be highly correlated with the Cobb angle.[26] [27] Therefore, if there is no improvement in ATR, no change in the Cobb angle can be expected. ATR or other assessment methods can be used to reduce radiation exposure in patients at low risk of progression, such as the current study population. In future studies, the long-term effectiveness of clinical pilates exercises in different age groups with scoliosis should be investigated.
From a scan of English literature on the effectiveness of Pilates exercises in scoliosis, only one randomized controlled trial could be identified that included a Pilates and a control group,[13] two studies comparing Schroth and Pilates exercises,[14] [15] one study that included a group of patients receiving Schroth and Pilates exercises at the same time,[28] and two case reports.[2] [29]
In the two studies comparing Schroth and Pilates exercises, the mean age of the cases was stated as 18 and 15 years for both groups.[14] [15] In both studies, a 12-week exercise program was applied and it was reported that Schroth exercises were superior to Pilates exercises in reducing the Cobb angle and improving psychological status.[14] [15] Patients between the ages of 15 and 30 years were included in the current study. Exercise therapies alone are not sufficient to manage scoliosis in younger age groups with incomplete bone maturation and high risk of progression.[1] [30] These children should also receive brace treatment, for which there is a high level of evidence.[1]
Rrecaj-Malaj et al reported that Schroth and Pilates exercises applied together to cases with mild and moderate idiopathic scoliosis were effective in reducing the Cobb angle and ATR, improving flexibility, and QOL at the end of a 24-week treatment program (2 weeks in the clinic, 10 weeks at home, 2 weeks in the clinic, 10 weeks at home, respectively).[28] However, the mean age of the cases was 13.4 years and some were wearing a brace. There was also reported to be a significant improvement in cases (mean Cobb angle presented as 14 degrees in baseline assessment) who did not use a brace. However, there was no detailed analysis according to the progression risk of the cases wearing and not wearing braces.[28]
There is no evidence to demonstrate a direct correlation between the severity of deformity and back pain.[1] A study of over 2,000 scoliosis patients with pain revealed no correlation between pain intensity and curve magnitude.[1] Muscle weakness, imbalance in strength between muscles, stiffness or a sedentary lifestyle may cause back pain.[1] A meta-analysis reported that Pilates exercises performed 2 to 3 times a week, for 5 to 12 weeks, improves abdominal muscular endurance, when compared with no exercise.[10] In the current study, Pilates exercises were applied to the patients twice a week for a total of 8 weeks. The improvement in pain and side shift and tilt posture scores in patients after clinical Pilates exercises may be related to the improvement in muscle strength, endurance, and flexibility. However, these variables were not evaluated separately in this study. Rrecaj-Malaj et al did not evaluate pain after the Schroth and Pilates exercises, but a significant improvement was reported in pain scores, which were included as subgroups in the quality of life scale.[28] Kim and Hwang Bo reported that there was no change in weight distribution in the Pilates exercise group, but there was a significant change in the Schroth exercise group.[14]
In the current study, when the sagittal plane changes were examined, it was determined that the kyphosis angle improved to within the physiological limits after the exercise program, but this change was not significant.
There was no change in quality of life and perception of spinal deformity scores after the exercise program. In a previous study, an improvement in the quality of life was achieved after the Schroth and Pilates exercise program in individuals using and not using a brace.[1]
Conclusion
The results of this study showed that Pilates exercises did not have a significant effect on deformity, quality of life, and perception of deformity in scoliosis, but significantly reduced back and low back pain and contributed to improvements in the posture.
It should not be forgotten that Pilates exercises are symmetrical and two-dimensional exercises, while scoliosis is a three-dimensional deformity. These exercises do not specifically focus on correcting the deformity. After detailed evaluation of individuals with scoliosis by physiotherapists who are experts in this field, an exercise program should be performed according to the results of this evaluation. Scoliosis-specific exercises should be preferred primarily to reduce the deformity, and if necessary, general exercise methods can be added to this program.
Conflict of Interest
None declared.
Ethics Approval
Approval for the study was granted by the Ethics Committee of Marmara University, Faculty of Medicine. All procedures were in accordance with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Informed written consent by parents and patients has been obtained. We followed the Consolidated Standards of Reporting Trials (CONSORT) checklist for the randomized clinical trials.
-
References
- 1 Moramarco M, Borsysov M, Ng SY, Weiss HR. Schroth's Textbook of scoliosis and other spinal deformities. Newcastle UK: Cambridge Scholars Publishing; 2020
- 2 Berdishevsky H, Lebel VA, Bettany-Saltikov J. et al. Physiotherapy scoliosis-specific exercises - a comprehensive review of seven major schools. Scoliosis Spinal Disord 2016; 11: 20
- 3 Burger M, Coetzee W, du Plessis LZ. et al. The effectiveness of Schroth exercises in adolescents with idiopathic scoliosis: a systematic review and meta-analysis. S Afr J Physiother 2019; 75 (01) 904
- 4 Monticone M, Ambrosini E, Cazzaniga D, Rocca B, Ferrante S. Active self-correction and task-oriented exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis. Results of a randomised controlled trial. Eur Spine J 2014; 23 (06) 1204-1214
- 5 Blum CL. Chiropractic and pilates therapy for the treatment of adult scoliosis. J Manipulative Physiol Ther 2002; 25 (04) E3
- 6 Solberg G. Postural Disorders and Musculoskelatal Dysfunction. Diagnosis, Prevention and Treatment. 2n ed. Philadelphia: Elsevier; 2008
- 7 Muscolino JE, Cipriani S. Pilates and the “powerhouse”—I. J Bodyw Mov Ther 2004; 8 (01) 15-24
- 8 Byrnes K, Wu PJ, Whillier S. Is Pilates an effective rehabilitation tool? A systematic review. J Bodyw Mov Ther 2018; 22 (01) 192-202
- 9 Hornsby E, Johnston LM. Effect of Pilates intervention on physical function of children and youth: a systematic review. Arch Phys Med Rehabil 2020; 101 (02) 317-328
- 10 Campos RR, Dias JM, Pereira LM. et al. Effect of the Pilates method on physical conditioning of healthy subjects: a systematic review and meta-analysis. J Sports Med Phys Fitness 2016; 56 (7-8): 864-873
- 11 Eliks M, Zgorzalewicz-Stachowiak M, Zeńczak-Praga K. Application of Pilates-based exercises in the treatment of chronic non-specific low back pain: state of the art. Postgrad Med J 2019; 95 (1119): 41-45
- 12 Emery K, De Serres SJ, McMillan A, Côté JN. The effects of a Pilates training program on arm-trunk posture and movement. Clin Biomech (Bristol, Avon) 2010; 25 (02) 124-130
- 13 Alves de Araújo ME, Bezerra da Silva E, Bragade Mello D, Cader SA, Shiguemi Inoue Salgado A, Dantas EH. The effectiveness of the Pilates method: reducing the degree of non-structural scoliosis, and improving flexibility and pain in female college students. J Bodyw Mov Ther 2012; 16 (02) 191-198
- 14 Kim G, HwangBo PN. Effects of Schroth and Pilates exercises on the Cobb angle and weight distribution of patients with scoliosis. J Phys Ther Sci 2016; 28 (03) 1012-1015
- 15 HwangBo PN. Psychological and physical effects of Schroth and Pilates exercise on female high school students with idiopathic scoliosis. J Kor Phys Ther 2016; 28 (06) 364-368
- 16 Scoliosis Research Society. Definitions & Causes. Accessed 20 May 2021 at: https://www.srs.org/patients-and-families/common-questions-and-glossary/frequently-asked-questions/general-spinal-deformity-faqs
- 17 Research Randomizer. Accessed September 6, 2019 at: http://www.randomizer.org/
- 18 Amendt LE, Ause-Ellias KL, Eybers JL, Wadsworth CT, Nielsen DH, Weinstein SL. Validity and reliability testing of the scoliometer. Phys Ther 1990; 70 (02) 108-117
- 19 Hopkins BB, Vehrs PR, Fellingham GW, George JD, Hager R, Ridge ST. Validity and reliability of standing posture measurements using a mobile application. J Manipulative Physiol Ther 2019; 42 (02) 132-140
- 20 Szucs KA, Brown EVD. Rater reliability and construct validity of a mobile application for posture analysis. J Phys Ther Sci 2018; 30 (01) 31-36
- 21 Salamh PA, Kolber M. The reliability, minimal detectable change and concurrent validity of a gravity-based bubble inclinometer and iphone application for measuring standing lumbar lordosis. Physiother Theory Pract 2014; 30 (01) 62-67
- 22 Scoliosis Research Society. SRS-23 scale. Accessed June 15, 2019 at: https://www.srs.org/professionals/online-education-and-resources/patient-outcome-questionnaires
- 23 Carreon LY, Sanders JO, Diab M, Polly DW, Diamond BE, Sucato DJ. Discriminative properties of the spinal appearance questionnaire compared with the Scoliosis Research Society–22 Revised. Spine Deform 2013; 1 (05) 328-338
- 24 Ferreira-Valente MA, Pais-Ribeiro JL, Jensen MP. Validity of four pain intensity rating scales. Pain 2011; 152 (10) 2399-2404
- 25 Isacowitz R, Clippinger K. Pilates Anatomy. Champaign, IL: Human Kinetics; 2020
- 26 Coelho DM, Bonagamba GH, Oliveira AS. Scoliometer measurements of patients with idiopathic scoliosis. Braz J Phys Ther 2013; 17 (02) 179-184
- 27 Samuelsson L, Norén L. Trunk rotation in scoliosis. The influence of curve type and direction in 150 children. Acta Orthop Scand 1997; 68 (03) 273-276
- 28 Rrecaj-Malaj S, Beqaj S, Krasniqi V, Qorolli M, Tufekcievski A. Outcome of 24 weeks of combined Schroth and Pilates exercises on Cobb angle, angle of trunk rotation, chest expansion, flexibility and quality of life in adolescents with idiopathic acoliosis. Med Sci Monit Basic Res 2020; 26: e920449
- 29 Moore K. The effects of mat pilates on weight-bearing symmetry, balance, and respiratory function in a young woman with scoliosis. JYP 2019; 8 (01) 10-22
- 30 Weiss HR, Negrini S, Rigo M. et al. SOSORT guideline committee. Indications for conservative management of scoliosis (guidelines). Scoliosis 2006; 1: 5
Address for correspondence
Publication History
Article published online:
04 October 2022
© 2022. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Moramarco M, Borsysov M, Ng SY, Weiss HR. Schroth's Textbook of scoliosis and other spinal deformities. Newcastle UK: Cambridge Scholars Publishing; 2020
- 2 Berdishevsky H, Lebel VA, Bettany-Saltikov J. et al. Physiotherapy scoliosis-specific exercises - a comprehensive review of seven major schools. Scoliosis Spinal Disord 2016; 11: 20
- 3 Burger M, Coetzee W, du Plessis LZ. et al. The effectiveness of Schroth exercises in adolescents with idiopathic scoliosis: a systematic review and meta-analysis. S Afr J Physiother 2019; 75 (01) 904
- 4 Monticone M, Ambrosini E, Cazzaniga D, Rocca B, Ferrante S. Active self-correction and task-oriented exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis. Results of a randomised controlled trial. Eur Spine J 2014; 23 (06) 1204-1214
- 5 Blum CL. Chiropractic and pilates therapy for the treatment of adult scoliosis. J Manipulative Physiol Ther 2002; 25 (04) E3
- 6 Solberg G. Postural Disorders and Musculoskelatal Dysfunction. Diagnosis, Prevention and Treatment. 2n ed. Philadelphia: Elsevier; 2008
- 7 Muscolino JE, Cipriani S. Pilates and the “powerhouse”—I. J Bodyw Mov Ther 2004; 8 (01) 15-24
- 8 Byrnes K, Wu PJ, Whillier S. Is Pilates an effective rehabilitation tool? A systematic review. J Bodyw Mov Ther 2018; 22 (01) 192-202
- 9 Hornsby E, Johnston LM. Effect of Pilates intervention on physical function of children and youth: a systematic review. Arch Phys Med Rehabil 2020; 101 (02) 317-328
- 10 Campos RR, Dias JM, Pereira LM. et al. Effect of the Pilates method on physical conditioning of healthy subjects: a systematic review and meta-analysis. J Sports Med Phys Fitness 2016; 56 (7-8): 864-873
- 11 Eliks M, Zgorzalewicz-Stachowiak M, Zeńczak-Praga K. Application of Pilates-based exercises in the treatment of chronic non-specific low back pain: state of the art. Postgrad Med J 2019; 95 (1119): 41-45
- 12 Emery K, De Serres SJ, McMillan A, Côté JN. The effects of a Pilates training program on arm-trunk posture and movement. Clin Biomech (Bristol, Avon) 2010; 25 (02) 124-130
- 13 Alves de Araújo ME, Bezerra da Silva E, Bragade Mello D, Cader SA, Shiguemi Inoue Salgado A, Dantas EH. The effectiveness of the Pilates method: reducing the degree of non-structural scoliosis, and improving flexibility and pain in female college students. J Bodyw Mov Ther 2012; 16 (02) 191-198
- 14 Kim G, HwangBo PN. Effects of Schroth and Pilates exercises on the Cobb angle and weight distribution of patients with scoliosis. J Phys Ther Sci 2016; 28 (03) 1012-1015
- 15 HwangBo PN. Psychological and physical effects of Schroth and Pilates exercise on female high school students with idiopathic scoliosis. J Kor Phys Ther 2016; 28 (06) 364-368
- 16 Scoliosis Research Society. Definitions & Causes. Accessed 20 May 2021 at: https://www.srs.org/patients-and-families/common-questions-and-glossary/frequently-asked-questions/general-spinal-deformity-faqs
- 17 Research Randomizer. Accessed September 6, 2019 at: http://www.randomizer.org/
- 18 Amendt LE, Ause-Ellias KL, Eybers JL, Wadsworth CT, Nielsen DH, Weinstein SL. Validity and reliability testing of the scoliometer. Phys Ther 1990; 70 (02) 108-117
- 19 Hopkins BB, Vehrs PR, Fellingham GW, George JD, Hager R, Ridge ST. Validity and reliability of standing posture measurements using a mobile application. J Manipulative Physiol Ther 2019; 42 (02) 132-140
- 20 Szucs KA, Brown EVD. Rater reliability and construct validity of a mobile application for posture analysis. J Phys Ther Sci 2018; 30 (01) 31-36
- 21 Salamh PA, Kolber M. The reliability, minimal detectable change and concurrent validity of a gravity-based bubble inclinometer and iphone application for measuring standing lumbar lordosis. Physiother Theory Pract 2014; 30 (01) 62-67
- 22 Scoliosis Research Society. SRS-23 scale. Accessed June 15, 2019 at: https://www.srs.org/professionals/online-education-and-resources/patient-outcome-questionnaires
- 23 Carreon LY, Sanders JO, Diab M, Polly DW, Diamond BE, Sucato DJ. Discriminative properties of the spinal appearance questionnaire compared with the Scoliosis Research Society–22 Revised. Spine Deform 2013; 1 (05) 328-338
- 24 Ferreira-Valente MA, Pais-Ribeiro JL, Jensen MP. Validity of four pain intensity rating scales. Pain 2011; 152 (10) 2399-2404
- 25 Isacowitz R, Clippinger K. Pilates Anatomy. Champaign, IL: Human Kinetics; 2020
- 26 Coelho DM, Bonagamba GH, Oliveira AS. Scoliometer measurements of patients with idiopathic scoliosis. Braz J Phys Ther 2013; 17 (02) 179-184
- 27 Samuelsson L, Norén L. Trunk rotation in scoliosis. The influence of curve type and direction in 150 children. Acta Orthop Scand 1997; 68 (03) 273-276
- 28 Rrecaj-Malaj S, Beqaj S, Krasniqi V, Qorolli M, Tufekcievski A. Outcome of 24 weeks of combined Schroth and Pilates exercises on Cobb angle, angle of trunk rotation, chest expansion, flexibility and quality of life in adolescents with idiopathic acoliosis. Med Sci Monit Basic Res 2020; 26: e920449
- 29 Moore K. The effects of mat pilates on weight-bearing symmetry, balance, and respiratory function in a young woman with scoliosis. JYP 2019; 8 (01) 10-22
- 30 Weiss HR, Negrini S, Rigo M. et al. SOSORT guideline committee. Indications for conservative management of scoliosis (guidelines). Scoliosis 2006; 1: 5