
Subscribe to RSS
DOI: 10.1055/s-0042-1758711
Surgical Management of the Armored Brain: Case Report of the Treatment of a Chronic Calcified Subdural Hematoma[*]
Manejo cirúrgico do cérebro blindado: Relato de caso do tratamento de hematoma subdural crônico calcificado

Abstract
Calcified chronic subdural hematomas (CCSDHs) are rare entities, whose yearly incidence ranges from 1.72 to 20.6 per every 100 thousand persons. Several different approaches to their management are reported in the literature, ranging from conservative treatment to craniotomy with full removal of the neomembranes. Currently, there are no guidelines or consensus that establish the best technique. We herein report a case of symptomatic CCSDH initially drained through a burr-hole craniotomy, with no resolution of the symptoms. Later, our patient underwent a craniotomy and partial membranectomy, which resulted in full symptomatic recovery.
Resumo
Hematomas subdurais crônicos calcificados (HSDCCs) são entidades raras, cuja incidência anual varia de 1,72 a 20,6 casos a cada 100 mil pessoas. Várias abordagens diferentes para seu manejo são relatadas na literatura, desde o tratamento conservador até a craniotomia com remoção total das neomembranas. Atualmente não há diretrizes ou consensos que estabeleçam a melhor técnica. Nós relatamos um caso de HSDCC inicialmente drenado por meio de uma craniotomia por trepanação, sem resolução dos sintomas. Posteriormente, nosso paciente foi submetido a uma craniotomia e membranectomia parcial, que resultou em plena recuperação dos sintomas.
Introduction
Chronic subdural hematoma (CSDH) is an abnormal collection of blood in the subdural space that develops for three or more weeks.[1] Its overall yearly incidence ranges from 1.72 to 20.6 per 100 thousand persons.[2] Between 0.5% and 2.0% of the cases of CSDH[3] undergo calcification, and they are known as calcified DSDHs (CCSDHs); their first known description was made by von Rokytansky in 1884.[4] Due to its similarity with an armor encapsulating the brain, this entity is sometimes referred to as armored brain.[5] In a review published in 2020, Turgut et al.[6] found only 114 reported cases of calcified or ossified CSDHs since 1930.
The purpose of the present report is to describe a case of a symptomatic CCSDH initially drained through a burr-hole craniotomy, with no resolution of the symptoms. Later, our patient was subjected to a craniotomy, which resulted in full symptomatic recovery.
Case Report
A 62-year-old male patient was brought to the emergency department (ED) by the emergency medical service. The accompanying family member reported that the patient felt dizzy after a meal and was unable to stand up. He also had nausea followed by vomiting with food content. His blood pressure was measured at 200/100 mmHg right after the symptoms. They denied any speech alteration or facial droop. Upon arrival at the ED, the patient had a Glasgow Coma Scale score of 14 due to confused verbal response, with an otherwise normal physical examination. His symptoms were gradually improving by the time he arrived at the ED. About five months before, the patient had a similar episode, which was treated as a hypertensive crisis with no organ damage. During the six months preceding the episode, the patient was suffering intermittent episodes of dysphasia and right hemiparesis, with spontaneous resolution. He also stated some episodes of syncope.
He was submitted to a brain magnetic resonance imaging (MRI) scan, which revealed a well-organized chronic subdural hematoma with focal compression of the underlying brain parenchyma ([Figs. 1] and [2]).


The patient was also subjected to a computed tomography (CT) scan of the brain, which showed calcifications around the hematoma.
We opted for the surgical management of the subdural hematoma through a burr hole right under the coronal suture on the left side. During the procedure, a minimum volume of hematic fluid was drained, and a suction drain was left in the subgaleal space. A postoperative contrast-enhanced MRI showed that the volume of the hematoma had not changed. This finding led us to conclude it was a CCSDH, and we indicated a reintervention.
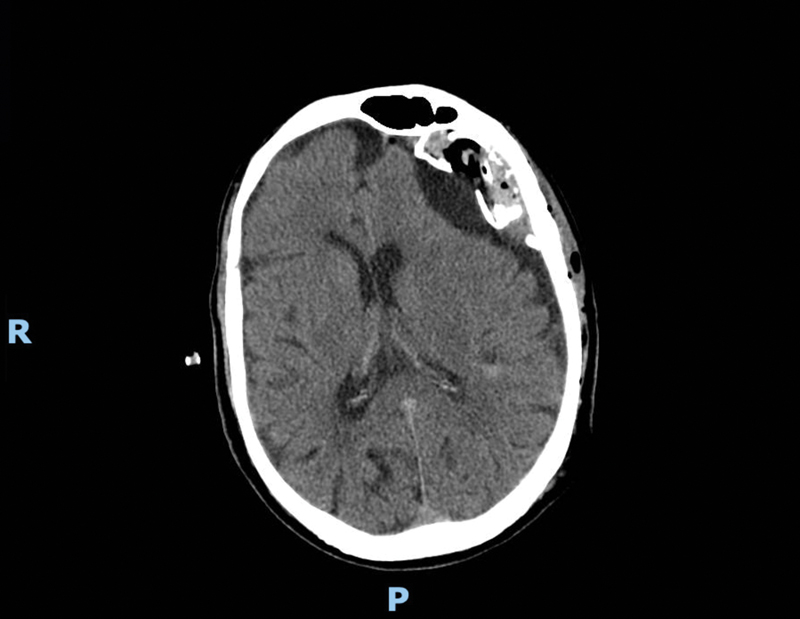
The patient was then subjected to a left frontal craniotomy, through which the hematoma was drained, and its cavity was opened to communicate with the subdural space, without complete removal of the calcified membrane. A CT scan performed after this second operation showed that the volume of the hematoma had decreased and that the calcified cavity was communicating with the subdural space beneath ([Fig. 3]).
The patient had no surgical complications or neurological deficits and his symptoms improved. He was discharged after 48 hours and remained neurologically intact at the 6-month follow-up visit.
Discussion
It is known that the pathological finding that distinguishes chronic from acute subdural hematomas is the development of neomembranes that encapsulate the bleeding in a cavity between the dura and the arachnoid.[7] With time, these neomembranes may evolve into firm collagen tissue that forms a fibrotic layer around a hygroma or liquefied hematoma.[8] It is not known why the fibrotic capsule of some of these CSDHs undergoes a process of calcification, creating a CCSDH.[9]
Although sometimes used interchangeably,[10] [11] the term ossification is best used when referring to CCSDHs that show microscopic evidence of bone formation, which may be considered a terminal phase of organization.[12]
The etiologic factor for CCSDH most commonly identified is repeated brain injuries,[6] although some cases may be related to shunt overdrainage[13] or meningitis.[14]
There are no guidelines regarding the ideal management of CCSDHs. Several authors[15] [16] [17] [18] have reported that craniotomy has no effect on long-standing symptoms, and thus recommend surgery only when acute or progressive neurological deficits are present. When indicated, the procedure of choice is a matter of controversy. Some authors advocate a craniotomy with full membranectomy,[10] [19] [20] [21] but there are also reports of satisfactory results with burr hole craniotomy.[22] When a hematoma reaccumulates after an initially satisfactory burr-hole drainage, a craniotomy may be necessary.[5] The same may be the case for infection of the subdural space after burr-hole drainage.[23] A rare but reported complication of a not sufficiently large membranectomy is the herniation of the brain into the subdural space.[24] Our patient was managed with a craniotomy and partial membranectomy, which were enough for the resolution of the symptoms.
Conclusion
Calcified chronic subdural hematoma is a rare entity whose management lacks guidelines or expert consensus. The case herein reported shows that drainage through a craniotomy and communication of the capsule with the subdural space through partial removal of the calcified membrane may be a feasible and effective option when surgical treatment is warranted.
Conflict of Interests
The authors have no conflict of interests to declare.
* Study conducted at Hospital São José, Santa Casa de Misericórdia de Porto Alegre, Porto Alegre, Rio grande do Sul, Brazil.
-
References
- 1 Sahyouni R, Goshtasbi K, Mahmoodi A, Tran DK, Chen JW. Chronic Subdural Hematoma: A Historical and Clinical Perspective. World Neurosurg 2017; 108: 948-953
- 2 Yang W, Huang J. Chronic Subdural Hematoma. 2022
- 3 Li X, Wan Y, Qian C, Yang S, Zhu X, Wang Y. Double-loculated Calcification Chronic Subdural Hematoma. Neurosurg Q 2015; 25 (02) 167-173
- 4 Rokitansky K. Handbuch der pathologischen Anatomie. Wien: Braumüller & Seidel; 1844
- 5 Dammers R, ter Laak-Poort MP, Maas AI. Neurological picture. Armoured brain: case report of a symptomatic calcified chronic subdural haematoma. J Neurol Neurosurg Psychiatry 2007; 78 (05) 542-543
- 6 Turgut M, Akhaddar A, Turgut AT. Calcified or Ossified Chronic Subdural Hematoma: A Systematic Review of 114 Cases Reported During Last Century with a Demonstrative Case Report. World Neurosurg 2020; 134: 240-263
- 7 Markwalder TM. Chronic subdural hematomas: a review. J Neurosurg 1981; 54 (05) 637-645
- 8 Friede RL. Incidence and distribution of neomembranes of dura mater. J Neurol Neurosurg Psychiatry 1971; 34 (04) 439-446
- 9 Ludwig B, Nix W, Lanksch W. Computed tomography of the “armored brain”. Neuroradiology 1983; 25 (01) 39-43
- 10 Snopko P, Kolarovszki B, Opsenak R, Hanko M, Benco M. Chronic calcified subdural hematoma - case report of a rare diagnosis. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 2020; 164 (02) 209-212
- 11 Trivedi A, Hiran S. Calcified epidural hematoma in pediatric age group: A report of two cases. J Neurosci Rural Pract 2010; 1 (02) 89-91
- 12 Chusid JG, De Gutiérrez-Mahoney CG. Ossifying subdural hematoma. J Neurosurg 1953; 10 (04) 430-434
- 13 Salunke P, Aggarwal A, Madhivanan K, Futane S. Armoured brain due to chronic subdural collections masking underlying hydrocephalus. Br J Neurosurg 2013; 27 (04) 524-525
- 14 Imaizumi S, Onuma T, Kameyama M, Naganuma H. Organized chronic subdural hematoma requiring craniotomy–five case reports. Neurol Med Chir (Tokyo) 2001; 41 (01) 19-24
- 15 Oda S, Shimoda M, Hoshikawa K, Shiramizu H, Matsumae M. Organized chronic subdural haematoma with a thick calcified inner membrane successfully treated by surgery: a case report. Tokai J Exp Clin Med 2010; 35 (03) 85-88
- 16 Watts C. The management of intracranial calcified subdural hematomas. Surg Neurol 1976; 6 (04) 247-250
- 17 Yang H, Tseng S, Chen Y, Lin S, Chen J. Calcified Chronic Subdural Hematoma—Case Report. Tzu-Chi Med J 2004; 16: 261-265
- 18 Petraglia AL, Moravan MJ, Jahromi BS. Armored brain: A case report and review of the literature. Surg Neurol Int 2011; 2 (01) 120-122
- 19 Callovini GM, Bolognini A, Callovini G, Gammone V. Primary enlarged craniotomy in organized chronic subdural hematomas. Neurol Med Chir (Tokyo) 2014; 54 (05) 349-356
- 20 Kaplan M, Akgün B, Seçer HI. Ossified chronic subdural hematoma with armored brain. Turk Neurosurg 2008; 18 (04) 420-424
- 21 Pappamikail L, Rato R, Novais G, Bernardo E. Chronic calcified subdural hematoma: Case report and review of the literature. Surg Neurol Int 2013; 4 (01) 21-23
- 22 Galldiks N, Dohmen C, Neveling M, Fink GR, Haupt WF. A giant bilateral calcified chronic subdural hematoma. Neurocrit Care 2010; 12 (02) 272-273
- 23 Li H, Mao X, Tao XG, Li JS, Liu BY, Wu Z. A Tortuous Process of Surgical Treatment for a Large Calcified Chronic Subdural Hematoma. World Neurosurg 2017; 108: 996.e1-996.e6
- 24 Marini A, Spennato P, Aliberti F. et al. Brain Herniation into the Subdural Space: Rare Iatrogenic Complication of Treatment of a Giant Calcified Subdural Hematoma. World Neurosurg 2020; 140: 65-70
Address for correspondence
Publication History
Received: 01 July 2022
Accepted: 18 August 2022
Article published online:
29 November 2022
© 2022. Sociedade Brasileira de Neurocirurgia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
References
- 1 Sahyouni R, Goshtasbi K, Mahmoodi A, Tran DK, Chen JW. Chronic Subdural Hematoma: A Historical and Clinical Perspective. World Neurosurg 2017; 108: 948-953
- 2 Yang W, Huang J. Chronic Subdural Hematoma. 2022
- 3 Li X, Wan Y, Qian C, Yang S, Zhu X, Wang Y. Double-loculated Calcification Chronic Subdural Hematoma. Neurosurg Q 2015; 25 (02) 167-173
- 4 Rokitansky K. Handbuch der pathologischen Anatomie. Wien: Braumüller & Seidel; 1844
- 5 Dammers R, ter Laak-Poort MP, Maas AI. Neurological picture. Armoured brain: case report of a symptomatic calcified chronic subdural haematoma. J Neurol Neurosurg Psychiatry 2007; 78 (05) 542-543
- 6 Turgut M, Akhaddar A, Turgut AT. Calcified or Ossified Chronic Subdural Hematoma: A Systematic Review of 114 Cases Reported During Last Century with a Demonstrative Case Report. World Neurosurg 2020; 134: 240-263
- 7 Markwalder TM. Chronic subdural hematomas: a review. J Neurosurg 1981; 54 (05) 637-645
- 8 Friede RL. Incidence and distribution of neomembranes of dura mater. J Neurol Neurosurg Psychiatry 1971; 34 (04) 439-446
- 9 Ludwig B, Nix W, Lanksch W. Computed tomography of the “armored brain”. Neuroradiology 1983; 25 (01) 39-43
- 10 Snopko P, Kolarovszki B, Opsenak R, Hanko M, Benco M. Chronic calcified subdural hematoma - case report of a rare diagnosis. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 2020; 164 (02) 209-212
- 11 Trivedi A, Hiran S. Calcified epidural hematoma in pediatric age group: A report of two cases. J Neurosci Rural Pract 2010; 1 (02) 89-91
- 12 Chusid JG, De Gutiérrez-Mahoney CG. Ossifying subdural hematoma. J Neurosurg 1953; 10 (04) 430-434
- 13 Salunke P, Aggarwal A, Madhivanan K, Futane S. Armoured brain due to chronic subdural collections masking underlying hydrocephalus. Br J Neurosurg 2013; 27 (04) 524-525
- 14 Imaizumi S, Onuma T, Kameyama M, Naganuma H. Organized chronic subdural hematoma requiring craniotomy–five case reports. Neurol Med Chir (Tokyo) 2001; 41 (01) 19-24
- 15 Oda S, Shimoda M, Hoshikawa K, Shiramizu H, Matsumae M. Organized chronic subdural haematoma with a thick calcified inner membrane successfully treated by surgery: a case report. Tokai J Exp Clin Med 2010; 35 (03) 85-88
- 16 Watts C. The management of intracranial calcified subdural hematomas. Surg Neurol 1976; 6 (04) 247-250
- 17 Yang H, Tseng S, Chen Y, Lin S, Chen J. Calcified Chronic Subdural Hematoma—Case Report. Tzu-Chi Med J 2004; 16: 261-265
- 18 Petraglia AL, Moravan MJ, Jahromi BS. Armored brain: A case report and review of the literature. Surg Neurol Int 2011; 2 (01) 120-122
- 19 Callovini GM, Bolognini A, Callovini G, Gammone V. Primary enlarged craniotomy in organized chronic subdural hematomas. Neurol Med Chir (Tokyo) 2014; 54 (05) 349-356
- 20 Kaplan M, Akgün B, Seçer HI. Ossified chronic subdural hematoma with armored brain. Turk Neurosurg 2008; 18 (04) 420-424
- 21 Pappamikail L, Rato R, Novais G, Bernardo E. Chronic calcified subdural hematoma: Case report and review of the literature. Surg Neurol Int 2013; 4 (01) 21-23
- 22 Galldiks N, Dohmen C, Neveling M, Fink GR, Haupt WF. A giant bilateral calcified chronic subdural hematoma. Neurocrit Care 2010; 12 (02) 272-273
- 23 Li H, Mao X, Tao XG, Li JS, Liu BY, Wu Z. A Tortuous Process of Surgical Treatment for a Large Calcified Chronic Subdural Hematoma. World Neurosurg 2017; 108: 996.e1-996.e6
- 24 Marini A, Spennato P, Aliberti F. et al. Brain Herniation into the Subdural Space: Rare Iatrogenic Complication of Treatment of a Giant Calcified Subdural Hematoma. World Neurosurg 2020; 140: 65-70