

Subscribe to RSS
DOI: 10.1055/s-0045-1813673
Vascular and Nonvascular Interventions in Gynecology
Authors


Abstract
Advancements in radiology have revolutionized medicine, making image-guided procedures the standard of care due to their precision and minimally invasive nature. In gynecology, these interventions are classified into nonvascular and vascular procedures. Nonvascular interventions include diagnostic biopsies and therapeutic procedures such as high-intensity focused ultrasound, radiofrequency ablation (RFA), microwave ablation (MWA), cryoablation (CA), and sclerotherapy. Vascular interventions are primarily therapeutic, including uterine artery embolization (UAE), gonadal vein embolization (GVE), and iliac/renal vein stenting.
Nonvascular interventions can be performed via transabdominal, transvaginal, or transrectal routes under ultrasound guidance, or transabdominal or transgluteal routes under computed tomography guidance. Biopsies are used to evaluate complex adnexal masses, while aspiration and drainage procedures manage ovarian cysts and pelvic collections. Sclerotherapy is an alternative to laparoscopic cystectomy for ovarian endometriomas, and RFA, MWA, and CA are used for uterine fibroids and hepatic metastasis in ovarian malignancies.
Vascular interventions, such as UAE, are effective for treating uterine fibroids and adenomyosis, offering a minimally invasive alternative to surgery. UAE reduces fibroid size and alleviates symptoms, with a high success rate. UAE is moderately effective in providing symptomatic relief in adenomyosis for patients who desire to preserve the uterus. Embolization is also used for managing bleeding in gynecological malignancies and treating pelvic venous disease (PeVD). GVE and pelvic varicosities sclerotherapy are effective for PeVD, while venous stenting addresses vein compression.
Image-guided interventions provide safe and effective diagnostic and therapeutic options for various gynecological conditions, improving patient outcomes and preserving fertility.
Introduction
Advancements in the field of radiology have revolutionized the practice of medicine. In this era of technology, image-guided procedures are the standard of care wherever it is feasible. It has the irrefutable advantage of being precise and minimally invasive while avoiding the morbidity and cost associated with surgery, which is most often the alternative.
In gynecology, like elsewhere, image-guided interventions may be broadly classified into nonvascular and vascular procedures. Nonvascular interventions can be further divided into diagnostic and therapeutic procedures. The former primarily comprises biopsies, while therapeutic interventions include procedures such as high-intensity focused ultrasound (HIFU), radiofrequency ablation (RFA), microwave ablation (MWA), cryoablation (CA), and sclerotherapy. Aspiration/drainage procedures can serve both diagnostic and therapeutic purposes. Vascular interventions are essentially therapeutic in nature and include uterine artery embolization (UAE), gonadal vein embolization (GVE), sclerotherapy of pelvic varicosities, and iliac/renal vein stenting.
Nonvascular Interventions
Gynecological interventions can be done via transabdominal, transvaginal, or transrectal route under ultrasound (US) guidance and via transabdominal or transgluteal route under computed tomography (CT) guidance. Local anesthesia is sufficient for most cases, using 2% lignocaine injection (or 2% lignocaine gel in case of transvaginal/transrectal route).
In deep-seated lesions where a safe window between bowel loops might be difficult to obtain on transabdominal US, transvaginal/transrectal approach or CT guidance is required.
Biopsies
Image-guided biopsies in gynecology are primarily used in evaluating complex adnexal masses with documented spread such as malignant ascites, peritoneal deposits, or distant metastases ([Fig. 1]). This is due to the dreaded possibility of causing dissemination in an otherwise localized malignant tumor, especially in cystic neoplasms. Though this is supported only by anecdotal evidence in literature with more recent studies deeming the risk to be theoretical,[1] [2] it is advisable to avoid performing such procedures unless left with no feasible alternative. Ovarian tumors without peritoneal spread can be biopsied if local invasiveness precludes surgery and tissue diagnosis is required to initiate chemotherapy. Image-guided biopsies are also very useful in the evaluation of omental and peritoneal deposits to confirm metastatic disease.

Biopsies can be performed using semiautomatic or automatic devices ([Fig. 2]). We prefer semiautomatic biopsy guns (18/20G × 16 cm) for transabdominal/transgluteal biopsies and automatic devices (18/20G × 25 cm) for transvaginal/transrectal biopsies. Longer needles are required for endoluminal procedures (along with a needle guide) to match the length of the endoluminal probe.

Percutaneous biopsies can be done in the in-plane or out-of-plane technique ([Fig. 3]), though the former is preferred wherever possible as the entire length of the needle can be visualized in a single frame.

Aspiration
Radiological imaging plays a major role in the evaluation and monitoring of ovarian cystic lesions, with guidelines in place providing a detailed roadmap.[3] Beyond diagnosis, the management of these lesions has also come under the purview of radiology. Image-guided ovarian cyst aspiration is an established treatment of choice in pre- and perimenopausal women with persistent, symptomatic cysts that have no US features of malignancy. In postmenopausal women, however, cyst aspiration is not recommended, with the disease best treated surgically, where possible, irrespective of US appearance.[4] Benign features on US include simple cysts, cysts with few thin (<3 mm) smooth septations, diffuse low-level internal echoes, and absent internal vascularity.[3] Aspiration should be avoided in complex/multilocular cysts and cysts with typical features of mature cystic teratoma. Endometriotic cyst aspiration is controversial and percutaneous puncture should be avoided in the initial stages due to the risk of pelvic adhesions. It can be attempted, preferably via transvaginal approach, in patients with chronic pain who wish to retain their reproductive potential.
Technique is the same as in biopsies, with the choice of approach determined by the route, which gives the best visibility of the cyst. We prefer the use of a spinal needle (18/20G, 9 cm) for transabdominal approach and Chiba needle (18/20G, 20 cm) for transvaginal/transrectal aspirations ([Figs. 4] and [5]).


Drainage Procedures
Complex pelvic collections such as abscesses with dense internal echoes/debris have a high chance of recurrence/incomplete drainage after simple needle aspiration. Image-guided placement of drainage catheters is preferable in such collections[5] ([Fig. 6]). Prior to catheter placement, needle aspiration can be done to confirm the presence of pus or to obtain samples for diagnostic tests.
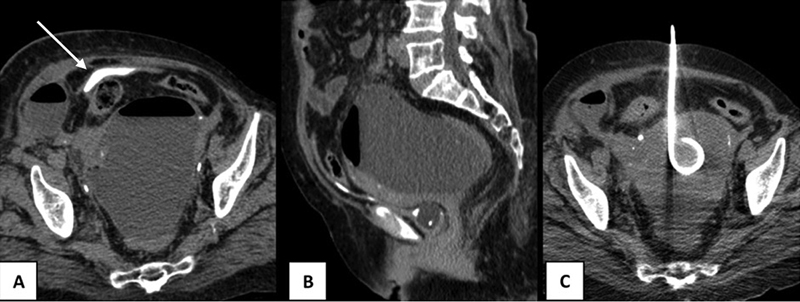
Pigtail catheters are widely used for drainage procedures. They are available in two kits, one with a guidewire and serial dilator set and another with a metal trocar ([Fig. 7]). The former is introduced using the Seldinger technique, whereas the latter is inserted via direct puncture.

Sclerotherapy
Sclerotherapy has emerged over the years as a promising alternative to laparoscopic cystectomy for the management of ovarian endometriomas due to concern over the risk of reduction in ovarian reserve associated with surgery.[6] It can also be used to treat recurrent pelvic collections such as lymphoceles/seromas. Needle aspiration of endometriomas has a high recurrence rate, and repeated aspirations increase the risk of the development of pelvic adhesions.
Catheter-directed sclerotherapy is preferred over direct needle injection due to the risk of needle displacement and peritoneal spillage of the sclerosant. Similar to drainage catheter placement, an 8Fr pigtail catheter is inserted into the endometrioma either via Seldinger technique (using Chiba needle, guidewire, and serial dilator) or direct puncture (using trocar). The cyst contents are aspirated, and a cystogram (by injecting radiopaque contrast material) is performed to confirm the absence of peritoneal leak. Ninety-five percent ethanol is then infused into the cyst at a volume of 25% of the aspirate (maximum dose of 100 mL).[7] The patient is then made to change positions intermittently, ensuring a 360-degree rotation, thereby allowing the sclerosant to mix well with any residual contents and coat the cyst wall epithelium entirely. After 20 minutes, the injected ethanol is completely reaspirated, and the catheter is removed.
Radiofrequency Ablation
RFA is a minimally invasive, uterus-preserving procedure for the treatment of symptomatic uterine leiomyomas.[8] [9] [10] It involves the placement of a specialized electrode under US or CT guidance into the lesion, through which high-frequency alternating current is passed, that causes agitation of surrounding molecules ([Fig. 8]). This results in the production of heat, which at temperatures above 60°C causes coagulative necrosis. A grounding pad is required for the completion of the circuit. The volume of ablated tissue is dependent on the electrode design, the amount of power supplied, and its duration. The uniformity of ablation can be limited by charring of tissue and proximity to vessels, the so-called heat-sink effect. RFA may be preferred over uterine fibroid embolization (UFE) in cases where the fibroids are smaller and limited in number, and when preservation of fertility is of paramount importance, as evidenced by multiple documented healthy pregnancies in post-RFA patients.[8] The requirement of an expensive cath-lab setup also limits the availability of UFE as a treatment option. RFA has also been found to be of use in the local control of hepatic metastasis in ovarian malignancies.[11]

Microwave Ablation
Similar to RFA, MWA is a minimally invasive technique of thermal ablation. It uses microwave energy to generate heat that results in a much more rapid and homogeneous ablative zone ([Fig. 8]). The indications, technique of antenna placement, and safety profile are similar to RFA.[12] [13] [14] However, unlike RFA, the thermal efficiency of MWA is less susceptible to the heat-sink effect and tissue impedance due to charring. The use of grounding pads is not required, thereby avoiding the risk of skin burns. MWA has also been found to produce larger ablation volumes and less periprocedural pain.[14] It is safe to use in patients with metallic devices such as pacemakers and surgical clips, which are absolute contraindications for RFA.
High-Intensity Focused Ultrasound
HIFU is a completely noninvasive method of thermal ablation where US energy is focused in short or continuous pulses over a target area, resulting in the production of heat and coagulative necrosis. It is used to treat symptomatic uterine fibroids as an alternative to myomectomy or hysterectomy.[15] HIFU systems can be either US-guided (USgFUS) or MRI-guided (MRgFUS). MRgFUS systems are more expensive but provide higher spatial and tissue contrast resolution for treatment planning and proton resonance frequency shift thermometry for intraprocedural monitoring ([Fig. 9]). HIFU has been found to result in shorter hospital stays, lower complication rates, and higher postprocedural pregnancy rates compared with UAE, while producing symptom reduction comparable to surgery.[16]

Cryoablation
CA is another uterine-sparing ablation technique which, contrary to RFA and MWA, utilizes the effect of rapid cooling (up to −40°C) to destroy tissue. It works on the principle of the Joule–Thomson effect, which refers to the drop in temperature attained when pressurized gas is forced through a valve, resulting in rapid expansion. Cryoprobes typically employ the use of argon and helium gases with a standard procedure requiring multiple freeze-thaw cycles that can be time consuming. It has been found to be as safe and effective as microwave and RFA with the added advantage of the ability to visualize the ablation zone in real time in the form of an ice-ball formation.[17] This is very helpful, both in planning further cycles to overcome underablation of the lesion and in stopping the procedure if the ablation zone has reached too close to a vital structure. Like in RFA, proximity to vessels can result in a “cold-sink effect.”[17] CA has been associated with less intraprocedural pain than MWA.[18] It has been found to be effective in the treatment of subserosal fibroids, which are resistant to UAE.[19] Similar to RFA and MWA, it can be used to treat limited hepatic metastasis in ovarian cancers.[20]
Vascular Interventions
Percutaneous vascular embolization is a highly effective therapeutic approach for treating various gynecological conditions. This minimally invasive technique eliminates the need for surgery and extended hospital stays, thereby reducing morbidity and overall cost while preserving the patient's potential for future fertility.
A comprehensive understanding of pelvic vascular anatomy is crucial for optimizing outcomes in transcatheter embolization procedures, especially in gynecologic interventions. Transcatheter embolization is utilized both for emergent control of pelvic and vaginal hemorrhages, as well as elective treatment of uterine fibroids and pelvic congestion syndrome. This technique is effective in managing bleeding complications resulting from various gynecological conditions, including benign conditions, advanced-stage cancer, and complications from gynecologic-obstetric surgeries.[21]
Transcatheter embolization is performed in an angiography suite with digital subtraction angiography capabilities or in an operating room equipped with similar angiographic technology. To manage pain and reduce anxiety, moderate sedation is administered intravenously using short-acting narcotics and benzodiazepines. After sterile preparation of the planned puncture site, the common femoral artery or radial artery is accessed utilizing a single-wall puncture technique. A 4- or 5-French short sheath is then introduced to maintain the access ([Fig. 10]).

Transcatheter embolization procedures are either performed via a transarterial route, such as UFE, or a transvenous route, such as gonadal vein (GV) and pelvic vein embolization in pelvic venous disorders (PeVDs).[21]
The procedure is usually preceded by cross-sectional imaging, which helps assess the vascular pathology and anatomy to plan the procedure. Typically, a 4- or 5-French selective angiographic catheter is used to access the internal iliac arteries, while a 2- or 3-French microcatheter and microwire may be employed for selective catheterization of smaller branches ([Fig. 10]). Once extravasation or another pathological condition is identified, the catheter is optimally positioned for embolization. The choice of embolic material depends on the indication. Transient but urgent pathologies such as postpartum hemorrhage will need swift, nonselective embolization using a nonpermanent agent (Gelfoam). At the same time, elective pathologies such as fibroid or adenomyosis require permanent particulate embolic agents (polyvinyl alcohol [PVA] or Embospheres). Focal pathologies such as pseudoaneurysms, require liquid (N-butyl cyanoacrylate) or mechanical agents (coils) ([Fig. 11]). These agents and sclerosants (sodium tetradecyl sulfate) are used during GVE for pelvic venous disease (PeVD).[21] [22]

Identification of the uterine artery, which is one of the initial branches of the anterior division of the internal iliac artery, is relatively easy due to its typical morphology. From lateral to medial, there are three portions: the descending, transverse, and ascending portions. The ascending segment, which courses along the body of the uterus, has a typical corkscrew appearance, which, when hypertrophied, becomes quite evident on the angiograms. The origin is profiled in the ipsilateral oblique projections ([Fig. 12]). Due to the abundant collateral supply of the uterus, uterine necrosis from UAE is uncommon.[15] Transradial access is gaining traction worldwide as a favored route in view of patient comfort, early mobilization, reduced complications, and potentially reduced costs.

Transarterial Procedures
Uterine Fibroid Embolization
Uterine fibroids are the most prevalent benign tumors of the pelvis, affecting approximately 20 to 40% of women of reproductive age.[23] These fibroids can be asymptomatic and may be discovered incidentally during routine pelvic USs.[23] However, they can also lead to a range of symptoms, with the most common being menorrhagia or dysmenorrhea. Other possible symptoms include urinary urgency, constipation, infertility, and pain, all of which necessitate treatment.
UFE is a minimally invasive treatment option, an alternative to surgical options such as myomectomy and hysterectomy, particularly for patients who prefer to preserve their uterus.[24] Uterine fibroids are commonly initially detected on transvaginal or transabdominal pelvic US. Contrast-enhanced magnetic resonance imaging (CE MRI) helps determine the exact size, location, and number of fibroids and their enhancement patterns ([Fig. 13A–C]). It also rules out other potential causes of a patient's symptoms.

A higher T2 signal intensity and greater postcontrast enhancement correlate with improved success rates following UFE.[25] Additionally, the type of fibroid can significantly impact clinical outcomes. For example, pedunculated and subserosal fibroids are linked to higher rates of complications such as expulsion of submucosal fibroids and necrosis or detachment of pedunculated subserosal fibroids. Understanding these factors is vital for optimizing patient care and improving treatment outcomes.[15]
Contraindications to UFE include viable pregnancy, active pelvic infections, gynecologic malignancy, severe renal dysfunction, and uncorrectable coagulopathy. Additionally, submucosal and pedunculated subserosal fibroids are considered relative contraindications.
UFE is typically performed via the common femoral artery utilizing a 5-French short sheath ([Fig. 10A]). Selective cannulation of the common iliac and internal iliac arteries is achieved using a dedicated Roberts uterine artery catheter. After successfully cannulating the uterine artery, a microcatheter may be advanced past the cervicovaginal branch of the uterine artery, and UFE is performed using PVA particles (500–700 µm) until stasis, indicated by stasis in 5 to 10 cardiac cycles. The ipsilateral iliac arteries are accessed by creating a Waltman's loop, and embolization is performed similarly to the contralateral side[25] ([Fig. 13]).
Postprocedure management after UFE is an important part of patient care; it focuses on controlling symptoms related to acute ischemia of the uterus and fibroids and addressing postembolization syndrome. Patients may experience abdominal cramps, nausea, and pain, which can start immediately after the procedure and persist during recovery. A multimodal regimen of acetaminophen, nonsteroidal anti-inflammatory drugs, and opioids is utilized for effective pain management following the procedure. Additionally, adjuvant techniques such as hypogastric nerve blocks and intra-arterial lidocaine administered during embolization may enhance pain control. Antiemetics are also used to address nausea and vomiting as part of postembolization syndrome management.[25] [26]
UAE has shown promising results for women with uterine fibroids. Patients experience a significant reduction in fibroid size, typically between 50 to 60%. Additionally, around 88 to 92% of women report relief from bulk symptoms, and more than 90% eliminate uterine bleeding. Overall, about 75% of patients see an improvement in their symptoms.[27]
Complications associated include prolonged vaginal discharge (2–17%), fibroid expulsion (3–15%), or, in rare cases, septicemia (1–3%). In patients desiring preservation of fertility, myomectomy is preferred over UFE due to a perceived fear of infertility after the latter procedure, although no robust data are available.[28] [29]
Recent studies and trials have provided insights into the efficacy and safety of UAE compared with other treatments such as myomectomy. The FEMME study, a randomized trial, compared UAE and myomectomy, finding that both treatments resulted in similar quality of life improvements. However, myomectomy had a slight edge in fibroid-related quality of life at 2-year follow-up, whereas UAE was associated with fewer complications, shorter hospital stays, and quicker return to work. There was no significant difference in the pregnancy rates or outcomes between UAE and myomectomy.[30]
The EMMY trial, with a 10-year follow-up, showed that UAE and hysterectomy had similar health-related quality of life outcomes. However, 35% of UAE patients eventually required a hysterectomy due to persistent symptoms.[31]
UAE is also effective for treating pedunculated fibroids despite initial concerns about complications such as fibroid torsion. Studies have shown that UAE can safely treat these fibroids, with a high symptom resolution rate and low complication rates.[21]
Overall, the UAE is a valuable option for women seeking uterine preservation, offering a minimally invasive alternative with comparable outcomes to surgical options.
Uterine Artery Embolization in Adenomyosis
Adenomyosis is the abnormal presence of endometrial tissue within the uterine myometrium with associated hypertrophy and hyperplasia of the stromal myometrium. This condition predominantly affects women aged 41 to 45 years, with an incidence rate of 1% and a prevalence of 0.8%. Adenomyosis can present as either focal or diffuse, and it is typically diagnosed using US and MRI. US findings often include a thickened endometrium, disruption of the endometrial–myometrial interface, and the presence of cysts within the myometrium. A thickened junctional zone exceeding 12 mm on MRI is a key diagnostic criterion for adenomyosis on MRI.
If the patient has menorrhagia or dysmenorrhea, which is medication resistant, invasive treatment options have to be considered. Hysterectomy remains the primary treatment option for definitive management, while UAE serves as an alternative strategy for patients wishing to preserve their uterus. However, UAE for adenomyosis has demonstrated lower efficacy than UFE. Recent studies indicate that the UAE's success and satisfaction rates for treating adenomyosis range from 60 to 70% and 72 to 94.3%, respectively.[28]
The technique of UAE is similar to UFE, except that embolization is started with smaller particles with progressively increased particle size using the 1-2-3 protocol (150–250, 250–355, and 355–500 µm PVA) ([Fig. 14]). This protocol aims to embolize the distal vessels and induce necrosis in the abnormal endometrial tissue.[32]

Embolization in Gynecological Malignancies
Embolization may be appropriate in patients with locally advanced uterine malignancies with intractable bleeding when conservative local treatments are ineffective ([Fig. 15]). Bleeding control within 24 hours occurs in 95% of patients after a pelvic vessel or UAE.[33] [34] Permanent embolic agents such as coils and liquid agents are preferred due to their durable embolic effect and ability to prevent the recurrence of bleeding.

Pelvic Venous Disease
PeVD is a spectrum of symptoms and signs arising from dysfunction in the pelvic veins and their drainage pathways. PeVD is characterized by noncyclic pelvic pain, dyspareunia, dysmenorrhea, and extrapelvic symptoms due to venous reflux, varices, or obstruction.[22]
The pelvic venous system includes the uterine, ovarian, and internal iliac veins (IIVs), which drain blood from the uterus and surrounding structures into the inferior vena cava (IVC). The left GV drains into the left renal vein, and the right GV drains into the IVC. Venous incompetence, often due to valve dysfunction or compression, leads to retrograde flow in the veins, which in turn causes venous hypertension and variceal formation in venous reservoirs. The PeVD primarily results from three pathophysiological mechanisms: ovarian vein reflux, compression of the left iliac vein (May–Thurner's syndrome), and the left renal vein (nutcracker syndrome).[35]
PeVD symptoms include noncyclic chronic pelvic pain, postcoital pain, and vulvar or lower extremity varices. The symptoms are aggravated by standing and become more severe by the end of the day. Transvaginal and transabdominal US and time-resolved magnetic resonance venography are key for diagnosing PeVDs and ruling out other pelvic pathologies. Key findings on US are dilated GVs (size > 6 mm) with retrograde flow on Valsalva, pelvic varices, and venous stenosis.[35] [36]
Catheter-directed venography is a definitive diagnostic tool for PeVDs. Characteristic findings include an ovarian vein diameter >6 mm, contrast retention >20 seconds, pelvic venous plexus congestion, opacification of the ipsilateral or contralateral internal iliac vein, and/or filling of vulvovaginal or thigh varices.[35]
Transcatheter embolization is an effective treatment option for PeVD. Its success rate is 98 to 100%, and symptom improvement is 80 to 93% in patients at 5 years. The complication and recurrence rates are low.
-
Gonadal vein embolization (GVE) ([Fig. 16]):
GVE is indicated in patients with gonadal venous reflux and is performed through a transjugular or transfemoral approach using coils, sclerosants, or both, with technical success of 96.7 to 100% and clinical success of 90 to 100%.[37]
GVE is a safe procedure. Rare adverse events include pulmonary embolism or coil migration. Recurrence of symptoms (15%), however, is not uncommon.
-
Pelvic varicosities sclerotherapy ([Fig. 16D]):
GV reflux is associated with pelvic varicosities and is treated with sclerotherapy using sclerosant foam (3% sodium tetradecyl sulfate). Coils are avoided because of the risk of coil migration.[37]
-
Venous stenting ([Fig. 17]):
For patients with a suspected primary cause of PeVD due to compression of either the iliac or renal veins, stenting of the stenosed or compressed vein, preferably by a dedicated venous stent, is the treatment option with a technical success rate of 94 to 100%. Intravascular US is superior to venography for grading stenosis severity, determining the exact site of stenosis, and guiding the sizing of the stent. Complications such as bleeding, stent migration, and thrombosis can occur. Venous stenting is effective for stenosis-related symptoms; however, the long-term outcome is less studied.[38]


Conclusion
Image-guided interventions provide a minimally invasive diagnostic and therapeutic option for various gynecological conditions, as outlined earlier. Drainage catheters can be safely placed into deep-seated pelvic collections under image guidance. The solid viable portion of complex adnexal masses can be accurately targeted during biopsies, thereby significantly improving diagnostic yield. Embolization of the uterine artery and image-guided ablation procedures have been proven to be as effective as surgery for uterine fibroids and adenomyosis. GVE with or without iliac vein stenting is safe and effective for the spectrum of PeVD.
Conflict of Interest
None declared.
-
References
- 1 Griffin N, Grant LA, Freeman SJ. et al. Image-guided biopsy in patients with suspected ovarian carcinoma: a safe and effective technique?. Eur Radiol 2009; 19 (01) 230-235
- 2 Thabet A, Somarouthu B, Oliva E, Gervais DA, Hahn PF, Lee SI. Image-guided ovarian mass biopsy: efficacy and safety. J Vasc Interv Radiol 2014; 25 (12) 1922-1927.e1
- 3 Andreotti RF, Timmerman D, Strachowski LM. et al. O-RADS US risk stratification and management system: a consensus guideline from the ACR Ovarian-Adnexal Reporting and Data System Committee. Radiology 2020; 294 (01) 168-185
- 4 Royal College of Obstetricians and Gynaecologists. The management of ovarian cysts in postmenopausal women. Green-top Guideline No. 34. London, England: Royal College of Obstetricians and Gynaecologists; 2011. . Accessed February 13, 2025, at: https://www.rcog.org.uk/media/4v3ncfib/gtg_34.pdf
- 5 Singh S, Chaudhary P, Saxena N, Khandelwal S, Poddar DD, Biswal UC. Treatment of liver abscess: prospective randomized comparison of catheter drainage and needle aspiration. Ann Gastroenterol 2013; 26 (04) 332-339
- 6 Cohen A, Almog B, Tulandi T. Sclerotherapy in the management of ovarian endometrioma: systematic review and meta-analysis. Fertil Steril 2017; 108 (01) 117-124.e5
- 7 Han K, Seo SK, Kim MD. et al. Catheter-directed sclerotherapy for ovarian endometrioma: short-term outcomes. Radiology 2018; 289 (03) 854-859
- 8 Chen I, Berman JM, Balk EM. et al. Radiofrequency ablation for the treatment of uterine fibroids: a systematic review and meta-analysis by the AAGL Practice Committee. J Minim Invasive Gynecol 2025; 32 (01) 74-91
- 9 Rey VE, Labrador R, Falcon M, Garcia-Benitez JL. Transvaginal radiofrequency ablation of myomas: technique, outcomes, and complications. J Laparoendosc Adv Surg Tech A 2019; 29 (01) 24-28
- 10 Yin G, Chen M, Yang S, Li J, Zhu T, Zhao X. Treatment of uterine myomas by radiofrequency thermal ablation: a 10-year retrospective cohort study. Reprod Sci 2015; 22 (05) 609-614
- 11 Gervais DA, Arellano RS, Mueller PR. Percutaneous radiofrequency ablation of ovarian cancer metastasis to the liver: indications, outcomes, and role in patient management. AJR Am J Roentgenol 2006; 187 (03) 746-750
- 12 Ierardi AM, Savasi V, Angileri SA. et al. Percutaneous high frequency microwave ablation of uterine fibroids: systematic review. BioMed Res Int 2018; 2018: 2360107 , 1-9
- 13 Liu H, Zhang J, Han ZY. et al. Effectiveness of ultrasound-guided percutaneous microwave ablation for symptomatic uterine fibroids: a multicentre study in China. Int J Hyperthermia 2016; 32 (08) 876-880
- 14 Poulou LS, Botsa E, Thanou I, Ziakas PD, Thanos L. Percutaneous microwave ablation vs radiofrequency ablation in the treatment of hepatocellular carcinoma. World J Hepatol 2015; 7 (08) 1054-1063
- 15 Silberzweig JE, Powell DK, Matsumoto AH, Spies JB. Management of uterine fibroids: a focus on uterine-sparing interventional techniques. Radiology 2016; 280 (03) 675-692
- 16 De Maio A, Alfieri G, Mattone M, Ghanouni P, Napoli A. High-intensity focused ultrasound surgery for tumor ablation: a review of current applications. Radiol Imaging Cancer 2024; 6 (01) e230074
- 17 Bertolotti L, Bazzocchi MV, Iemma E. et al. Radiofrequency ablation, cryoablation, and microwave ablation for the treatment of small renal masses: efficacy and complications. Diagnostics (Basel) 2023; 13 (03) 388
- 18 Li HW, Long YJ, Yan GW. et al. Microwave ablation vs. cryoablation for treatment of primary and metastatic pulmonary malignant tumors. Mol Clin Oncol 2022; 16 (03) 62
- 19 Zhao Z, Guo Z, Ni H, Liu F, Li B. CT-monitored percutaneous cryoablation of uterine fibroids after uterine artery embolization. Chin J Clin Oncol 2007; 4 (04) 241-245
- 20 Gao W, Guo Z, Zhang X. et al. Percutaneous cryoablation of ovarian cancer metastasis to the liver. Int J Gynecol Cancer 2015; 25 (05) 802-808
- 21 Tanaka ME, Keefe N, Caridi T, Kohi M, Salazar G. Interventional radiology in obstetrics and gynecology: updates in women's health. Radiographics 2023; 43 (03) e220039
- 22 Rezaei-Kalantari K, Fahrni G, Rotzinger DC, Qanadli SD. Insights into pelvic venous disorders. Front Cardiovasc Med 2023; 10: 1102063
- 23 Stewart JK. Uterine artery embolization for uterine fibroids: a closer look at misperceptions and challenges. Tech Vasc Interv Radiol 2021; 24 (01) 100725
- 24 Bradley EA, Reidy JF, Forman RG, Jarosz J, Braude PR. Transcatheter uterine artery embolisation to treat large uterine fibroids. Br J Obstet Gynaecol 1998; 105 (02) 235-240
- 25 Ozen M, Patel R, Hoffman M, Raissi D. Update on endovascular therapy for fibroids and adenomyosis. Semin Intervent Radiol 2023; 40 (04) 327-334
- 26 Chan P, Garcia-Reyes K, Cronan J. et al. Managing postembolization syndrome-related pain after uterine fibroid embolization. Semin Intervent Radiol 2021; 38 (03) 382-387
- 27 Peng J, Wang J, Shu Q, Luo Y, Wang S, Liu Z. Systematic review and meta-analysis of current evidence in uterine artery embolization vs myomectomy for symptomatic uterine fibroids. Sci Rep 2024; 14 (01) 19252
- 28 Mailli L, Patel S, Das R. et al. Uterine artery embolisation: fertility, adenomyosis and size - what is the evidence?. CVIR Endovasc 2023; 6 (01) 8
- 29 Kröncke T. An update on uterine artery embolization for uterine leiomyomata and adenomyosis of the uterus. Br J Radiol 2023; 96 (1143): 20220121
- 30 Manyonda I, Belli AM, Lumsden MA. et al; FEMME Collaborative Group. Uterine-artery embolization or myomectomy for uterine fibroids. N Engl J Med 2020; 383 (05) 440-451
- 31 de Bruijn AM, Ankum WM, Reekers JA. et al. Uterine artery embolization vs hysterectomy in the treatment of symptomatic uterine fibroids: 10-year outcomes from the randomized EMMY trial. Am J Obstet Gynecol 2016; 215 (06) 745.e1-745.e12
- 32 Caridi TM. Uterine artery embolization for adenomyosis. Tech Vasc Interv Radiol 2021; 24 (01) 100726
- 33 Alméciga A, Rodriguez J, Beltrán J. et al. Emergency embolization of pelvic vessels in patients with locally advanced cervical cancer and massive vaginal bleeding: a case series in a Latin American Oncological Center. JCO Glob Oncol 2020; 6 (06) 1376-1383
- 34 Choi J, Shin JH, Chu HH. Transcatheter arterial embolization for palliation of uterine body cancer bleeding. J Korean Soc Radiol 2023; 84 (03) 606-614
- 35 Khilnani NM, Winokur RS, Scherer KL, Meissner MH. Clinical presentation and evaluation of pelvic venous disorders in women. Tech Vasc Interv Radiol 2021; 24 (01) 100730
- 36 Topper SR, Winokur RS. Imaging of pelvic venous disorders (PeVD); should every patient get an MRI?. Tech Vasc Interv Radiol 2021; 24 (01) 100731
- 37 Joh M, Grewal S, Gupta R. Ovarian vein embolization: how and when should it be done?. Tech Vasc Interv Radiol 2021; 24 (01) 100732
- 38 Kutsenko O, McColgan Y, Salazar G. Iliac vein stenosis: is the data strong enough for stenting in the young pelvic venous disorders (PeVD) population?. Tech Vasc Interv Radiol 2021; 24 (01) 100733
Address for correspondence
Publication History
Article published online:
03 December 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Griffin N, Grant LA, Freeman SJ. et al. Image-guided biopsy in patients with suspected ovarian carcinoma: a safe and effective technique?. Eur Radiol 2009; 19 (01) 230-235
- 2 Thabet A, Somarouthu B, Oliva E, Gervais DA, Hahn PF, Lee SI. Image-guided ovarian mass biopsy: efficacy and safety. J Vasc Interv Radiol 2014; 25 (12) 1922-1927.e1
- 3 Andreotti RF, Timmerman D, Strachowski LM. et al. O-RADS US risk stratification and management system: a consensus guideline from the ACR Ovarian-Adnexal Reporting and Data System Committee. Radiology 2020; 294 (01) 168-185
- 4 Royal College of Obstetricians and Gynaecologists. The management of ovarian cysts in postmenopausal women. Green-top Guideline No. 34. London, England: Royal College of Obstetricians and Gynaecologists; 2011. . Accessed February 13, 2025, at: https://www.rcog.org.uk/media/4v3ncfib/gtg_34.pdf
- 5 Singh S, Chaudhary P, Saxena N, Khandelwal S, Poddar DD, Biswal UC. Treatment of liver abscess: prospective randomized comparison of catheter drainage and needle aspiration. Ann Gastroenterol 2013; 26 (04) 332-339
- 6 Cohen A, Almog B, Tulandi T. Sclerotherapy in the management of ovarian endometrioma: systematic review and meta-analysis. Fertil Steril 2017; 108 (01) 117-124.e5
- 7 Han K, Seo SK, Kim MD. et al. Catheter-directed sclerotherapy for ovarian endometrioma: short-term outcomes. Radiology 2018; 289 (03) 854-859
- 8 Chen I, Berman JM, Balk EM. et al. Radiofrequency ablation for the treatment of uterine fibroids: a systematic review and meta-analysis by the AAGL Practice Committee. J Minim Invasive Gynecol 2025; 32 (01) 74-91
- 9 Rey VE, Labrador R, Falcon M, Garcia-Benitez JL. Transvaginal radiofrequency ablation of myomas: technique, outcomes, and complications. J Laparoendosc Adv Surg Tech A 2019; 29 (01) 24-28
- 10 Yin G, Chen M, Yang S, Li J, Zhu T, Zhao X. Treatment of uterine myomas by radiofrequency thermal ablation: a 10-year retrospective cohort study. Reprod Sci 2015; 22 (05) 609-614
- 11 Gervais DA, Arellano RS, Mueller PR. Percutaneous radiofrequency ablation of ovarian cancer metastasis to the liver: indications, outcomes, and role in patient management. AJR Am J Roentgenol 2006; 187 (03) 746-750
- 12 Ierardi AM, Savasi V, Angileri SA. et al. Percutaneous high frequency microwave ablation of uterine fibroids: systematic review. BioMed Res Int 2018; 2018: 2360107 , 1-9
- 13 Liu H, Zhang J, Han ZY. et al. Effectiveness of ultrasound-guided percutaneous microwave ablation for symptomatic uterine fibroids: a multicentre study in China. Int J Hyperthermia 2016; 32 (08) 876-880
- 14 Poulou LS, Botsa E, Thanou I, Ziakas PD, Thanos L. Percutaneous microwave ablation vs radiofrequency ablation in the treatment of hepatocellular carcinoma. World J Hepatol 2015; 7 (08) 1054-1063
- 15 Silberzweig JE, Powell DK, Matsumoto AH, Spies JB. Management of uterine fibroids: a focus on uterine-sparing interventional techniques. Radiology 2016; 280 (03) 675-692
- 16 De Maio A, Alfieri G, Mattone M, Ghanouni P, Napoli A. High-intensity focused ultrasound surgery for tumor ablation: a review of current applications. Radiol Imaging Cancer 2024; 6 (01) e230074
- 17 Bertolotti L, Bazzocchi MV, Iemma E. et al. Radiofrequency ablation, cryoablation, and microwave ablation for the treatment of small renal masses: efficacy and complications. Diagnostics (Basel) 2023; 13 (03) 388
- 18 Li HW, Long YJ, Yan GW. et al. Microwave ablation vs. cryoablation for treatment of primary and metastatic pulmonary malignant tumors. Mol Clin Oncol 2022; 16 (03) 62
- 19 Zhao Z, Guo Z, Ni H, Liu F, Li B. CT-monitored percutaneous cryoablation of uterine fibroids after uterine artery embolization. Chin J Clin Oncol 2007; 4 (04) 241-245
- 20 Gao W, Guo Z, Zhang X. et al. Percutaneous cryoablation of ovarian cancer metastasis to the liver. Int J Gynecol Cancer 2015; 25 (05) 802-808
- 21 Tanaka ME, Keefe N, Caridi T, Kohi M, Salazar G. Interventional radiology in obstetrics and gynecology: updates in women's health. Radiographics 2023; 43 (03) e220039
- 22 Rezaei-Kalantari K, Fahrni G, Rotzinger DC, Qanadli SD. Insights into pelvic venous disorders. Front Cardiovasc Med 2023; 10: 1102063
- 23 Stewart JK. Uterine artery embolization for uterine fibroids: a closer look at misperceptions and challenges. Tech Vasc Interv Radiol 2021; 24 (01) 100725
- 24 Bradley EA, Reidy JF, Forman RG, Jarosz J, Braude PR. Transcatheter uterine artery embolisation to treat large uterine fibroids. Br J Obstet Gynaecol 1998; 105 (02) 235-240
- 25 Ozen M, Patel R, Hoffman M, Raissi D. Update on endovascular therapy for fibroids and adenomyosis. Semin Intervent Radiol 2023; 40 (04) 327-334
- 26 Chan P, Garcia-Reyes K, Cronan J. et al. Managing postembolization syndrome-related pain after uterine fibroid embolization. Semin Intervent Radiol 2021; 38 (03) 382-387
- 27 Peng J, Wang J, Shu Q, Luo Y, Wang S, Liu Z. Systematic review and meta-analysis of current evidence in uterine artery embolization vs myomectomy for symptomatic uterine fibroids. Sci Rep 2024; 14 (01) 19252
- 28 Mailli L, Patel S, Das R. et al. Uterine artery embolisation: fertility, adenomyosis and size - what is the evidence?. CVIR Endovasc 2023; 6 (01) 8
- 29 Kröncke T. An update on uterine artery embolization for uterine leiomyomata and adenomyosis of the uterus. Br J Radiol 2023; 96 (1143): 20220121
- 30 Manyonda I, Belli AM, Lumsden MA. et al; FEMME Collaborative Group. Uterine-artery embolization or myomectomy for uterine fibroids. N Engl J Med 2020; 383 (05) 440-451
- 31 de Bruijn AM, Ankum WM, Reekers JA. et al. Uterine artery embolization vs hysterectomy in the treatment of symptomatic uterine fibroids: 10-year outcomes from the randomized EMMY trial. Am J Obstet Gynecol 2016; 215 (06) 745.e1-745.e12
- 32 Caridi TM. Uterine artery embolization for adenomyosis. Tech Vasc Interv Radiol 2021; 24 (01) 100726
- 33 Alméciga A, Rodriguez J, Beltrán J. et al. Emergency embolization of pelvic vessels in patients with locally advanced cervical cancer and massive vaginal bleeding: a case series in a Latin American Oncological Center. JCO Glob Oncol 2020; 6 (06) 1376-1383
- 34 Choi J, Shin JH, Chu HH. Transcatheter arterial embolization for palliation of uterine body cancer bleeding. J Korean Soc Radiol 2023; 84 (03) 606-614
- 35 Khilnani NM, Winokur RS, Scherer KL, Meissner MH. Clinical presentation and evaluation of pelvic venous disorders in women. Tech Vasc Interv Radiol 2021; 24 (01) 100730
- 36 Topper SR, Winokur RS. Imaging of pelvic venous disorders (PeVD); should every patient get an MRI?. Tech Vasc Interv Radiol 2021; 24 (01) 100731
- 37 Joh M, Grewal S, Gupta R. Ovarian vein embolization: how and when should it be done?. Tech Vasc Interv Radiol 2021; 24 (01) 100732
- 38 Kutsenko O, McColgan Y, Salazar G. Iliac vein stenosis: is the data strong enough for stenting in the young pelvic venous disorders (PeVD) population?. Tech Vasc Interv Radiol 2021; 24 (01) 100733