

RSS-Feed abonnieren
DOI: 10.1055/s-0045-1814082
Factors Affecting Facial Nerve Exposure during Extracapsular Dissection of Benign Parotid Tumors
Autor*innen


Abstract
Extracapsular dissection (ECD) is typically indicated for small, benign parotid tumors. The surgical procedure for ECD does not involve the identification of the main trunk of the facial nerve. Although the nerve branches may become exposed during surgery, it is considered safer if they are not exposed. Therefore, we investigated the relationship between tumor location and size and intraoperative exposure of nerve branches in cases of ECD. The study included 61 cases that underwent ECD, with tumors meeting all of the following criteria preoperatively: tumor diameter ≤25 mm, superficial tumor, good mobility, and benign tumor. The tumor location was determined via magnetic resonance imaging, with the anterior–posterior axis classified into anterior, middle, and posterior regions, and the superior–inferior axis classified into superior, middle, and inferior regions. We compared 29 cases in which the nerve branches were identified (identified group) with 32 cases in which the nerve branches were not identified (nonidentified group). All three cases that developed transient facial nerve paralysis after surgery were included in the identified group. Excluding anterior tumors, nerve exposure was significantly more frequent in cases with a tumor diameter of ≥16 mm. The diameter of posterior tumors was significantly larger than that of anterior tumors; however, the nerve identification rate was significantly lower. Anterior tumors were significantly smaller in diameter than posterior tumors; however, no significant difference was observed in the nerve identification rate. These findings are likely influenced by tumor location and the course of the facial nerve. When the nerve is exposed or identified during ECD, there is an associated risk of postoperative transient facial nerve paralysis. Therefore, it is important to assess the likelihood of nerve identification based on tumor size and location before surgery.
Introduction
In the early 1900s, enucleation was the primary surgical approach for benign parotid tumors, and postoperative recurrence rates were reported to be as high as 45% for pleomorphic adenomas.[1] Total parotidectomy and superficial parotidectomy (SP) were proposed in the 1940s, significantly reducing the recurrence rate of pleomorphic adenomas. However, these techniques were associated with high postoperative rates of facial nerve palsy and Frey's syndrome.[2] [3] Therefore, partial superficial parotidectomy (PSP), which preserves normal parotid tissue and minimizes the dissection of facial nerve branches, was introduced and has been shown to result in lower complications and recurrence rates than those associated with SP.[4] [5] In the 1990s, extracapsular dissection (ECD) was introduced as an even more limited surgical procedure,[6] [7] in which tumors are resected without identifying the main trunk of the facial nerve and, unlike enucleation, are removed extracapsularly. Previously, we compared ECD and PSP for benign parotid tumors and reported ECD as a useful surgical procedure for select cases.[8]
Initially, ECD was defined as a surgical procedure that removes small benign tumors in the superficial lobe without identifying the main nerve trunk of the facial nerve.[6] [7] [9] Meanwhile, intraoperative exposure and identification of nerve branches were considered acceptable. Subsequently, some reports have suggested that ECD is also appropriate for patients in whom nerve branches are deliberately identified.[10] However, from the perspective of preventing postoperative facial nerve palsy, the procedure is considered safer when nerve branches are not exposed. Therefore, performing ECD safely requires preoperative estimation of the likelihood of nerve branch exposure based on two factors, tumor size and location.
In this study, we investigated the relationships between tumor size and location and the intraoperative exposure and identification of facial nerve branches in patients in whom tumors were removed via ECD at our department.
Materials and Methods
Definition of ECD in Target Cases
Defining the resection range of ECD as “tumor resection outside the capsule” broadens its indication for benign parotid tumors. For example, in cases of deep lobe tumors, a procedure resembling ECD rather than partial deep parotidectomy is often performed. However, despite the extracapsular resection, it is generally not classified as ECD because it involves systematic identification of the main trunk and branches of the facial nerve before tumor resection.
Therefore, in the present study, we focused on cases in which the facial nerve trunk was not identified, and the tumor was removed extracapsularly. When the tumor was sufficiently distant from the nerve, it was removed along with some normal parotid tissue, whereas tumors close to the nerve were removed extracapsularly. Surgical procedures involving intentional or incidental exposure or identification of facial nerve branches were included. Nerve exposure or identification was defined as the nerve being visible in the surgical field during or after resection (exposed) and confirmed (identified) by facial nerve monitoring (FNM; NIM-Response 3.0 system [four channel], Medtronic Inc., Jacksonville, FL). Hereinafter, nerve identification refers specifically to the identification of facial nerve branches.
Target Cases
This study included 61 cases of benign parotid tumors removed by ECD over approximately 8 years, from January 2016 to March 2024. The indication criteria for ECD were a preoperative tumor size of ≤25 mm (on ultrasound), location in the superficial lobe (on ultrasound and magnetic resonance imaging [MRI]), good mobility (on palpation), and benign nature (based on imaging and fine-needle aspiration cytology). In addition, this study included cases in which patients underwent ECD for a tumor initially diagnosed as superficial but later found to be located in the deep lobe after resection. Tumor size was defined as the maximum diameter (tumor thickness), measured from the superficial to the deep lobe of the parotid gland. A total of 636 surgeries, including ECD, for benign parotid tumors were performed during the study period. The 61 patients who underwent ECD had a mean age of 55.4 years and included 25 men and 36 women. The tumors comprised 36 pleomorphic adenomas, 9 Warthin tumors, 4 basal cell adenomas, 4 cysts, and 8 cases of other types.
This study was approved by the Ethics Committee of Osaka Medical and Pharmaceutical University (#1508).
Methods
Tumor Location
Tumor location was determined via preoperative MRI. In the anterior–posterior (nasal–auricular) direction, the parotid gland was divided into three sections on axial MRI, and tumor location was classified as anterior, medial, and posterior based on the tumor center. In the superior–inferior (cranial–caudal) direction, the parotid gland was divided into three sections on coronal MRI, and tumor location was classified as superior, medial, and inferior based on the tumor center ([Fig. 1]).

Surgical Procedure and Technique
All patients underwent ECD under general anesthesia.[8] Regardless of tumor location or size, an S-shaped skin incision was made, followed by skin flap elevation to expose the surgical field. Intraoperative FNM was used as appropriate to determine the facial nerve location. For nonanterior tumors, the skin was elevated from inferior (caudal) to superior (cranial) along the anterior border of the sternocleidomastoid muscle, after which the pointer cartilage above the mastoid process was identified. The main trunk was not identified. Locating the pointer cartilage is a useful method for safer resection, as it allows estimation of the location of the main trunk and the course of the branches. Tumor resection was mainly performed using electrocautery, and dissection was performed while monitoring the degree of facial muscle contraction. In other words, dissection was performed with electrocautery when there was no facial muscle response, with electrocautery while monitoring the response using nerve integrity monitoring (NIM) when a weak response was observed, and without electrocautery while monitoring the nerve with NIM when a strong response was observed. Dissection was initiated from the posterior side of tumors. For anterior tumors, the skin was elevated to expose the surgical field, and tumor resection was performed without detaching the anterior border of the sternocleidomastoid muscle or identifying the pointer cartilage.[11] The resection margin depended on the positional relationship between the tumor and nerve and was determined based on the degree of facial muscle contraction induced by electrocautery and FNM responses. When the tumor was close to the nerve, it was resected along the extracapsular route; when the tumor was distant from the nerve, it was resected with a few millimeters to 1 cm of normal parotid tissue attached. If any nerve branches were exposed, they were identified using FNM and dissected only to the extent required for tumor resection.
Nerve-identified and Nonidentified Groups
We compared the nerve-identified (29 cases) and nonidentified groups (32 cases) in terms of age, sex, histopathological type, tumor size, operative duration, tumor location, and postoperative transient facial nerve palsy. Tumors located superficial to the facial nerve plane were classified as superficial lobe tumors, those located deeper as deep lobe tumors, and tumors with a center inferior to the marginal mandibular branch as lower pole tumors.[12]
Tumor Size and Nerve Identification
Tumor size was categorized into 5-mm intervals, and the relationship between tumor size and nerve identification versus nonidentification was examined for all cases (61 cases) and for cases excluding anterior tumors (40 cases).
Tumor Size and Nerve Identification by Tumor Location (Anterior–Posterior Direction; Axial Section)
Tumor location was divided into three regions in the anterior–posterior direction. The study included 21 anterior, 18 medial, and 22 posterior tumors.
Tumor size was compared across locations (anterior, medial, and posterior). In addition, tumor size within each location was compared between the nerve-identified and nonidentified groups. Nerve identification rates across different locations were also examined and compared.
Tumor Size and Nerve Identification by Tumor Location (Superior–Inferior Direction; Coronal Section)
Tumor location was divided into three regions in the superior–inferior direction. The study included 8 superior, 26 medial, and 27 inferior tumors.
Tumor size was compared by location (superior, medial, and inferior). In addition, tumor size in each location was compared between the nerve-identified and nonidentified groups. The nerve identification rates across different locations were examined and compared.
Statistical Analysis
The nerve-identified and nonidentified groups were compared in terms of age, tumor size, and operative duration using the Mann–Whitney U test and in terms of sex, histopathological type, tumor location, and postoperative transient facial nerve palsy using the Fisher's exact test. To investigate the relationship between nerve identification/nonidentification and tumor size, cases were divided into two groups based on tumor size: 5 to 15 mm and 16 to 25 mm. The numbers of nerve-identified and nonidentified cases were compared using Fisher's exact test. For the analysis of tumor size and nerve identification rate by tumor location, anterior, medial, and posterior tumors were compared using the Kruskal–Wallis test, with corrections for multiple comparisons using the Holm method. Superior, medial, and inferior tumors were compared using the Fisher's exact test, with corrections for multiple comparisons using the Steel–Dwass method. Tumor sizes in the nerve-identified and nonidentified groups were compared by tumor location using the Mann–Whitney U test. In addition, identification rates for tumors at different locations were compared across all cases using the binomial test. A p-value <0.05 was considered statistically significant.
Results
Comparison Between the Nerve-identified and Nonidentified Groups
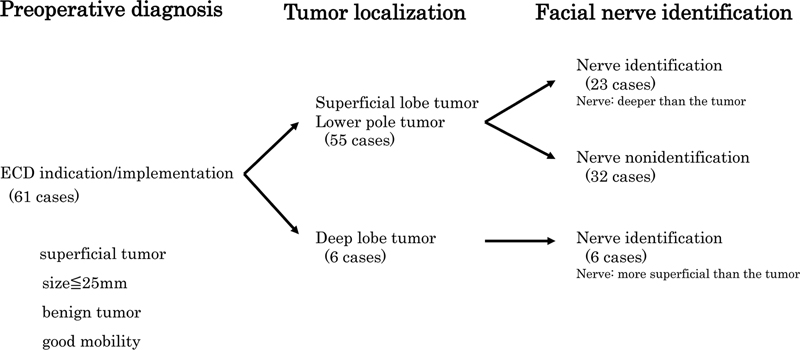
The 29 cases in which facial nerve branches were identified (identified group) and the 32 cases in which they were not identified (nonidentified group) were compared ([Table 1]). The identified and nonidentified groups had a mean age of 51.3 and 57.9 years, respectively, and a sex ratio (male:female) of 10:19 and 15:17, respectively, with no significant differences observed. The two groups also did not differ significantly in terms of age, sex, histopathological type (pleomorphic adenoma versus Warthin tumor), tumor size, and operative duration. Among 55 cases in which tumors were classified as superficial lobe or lower pole tumors after resection, nerve branches were identified in 23 cases. In contrast, nerve branches were identified in all six cases of deep lobe tumor, which were anterior tumors. These results indicate a significant association between tumor location and nerve identification (p = 0.009) ([Fig. 2]). All three cases of postoperative transient facial nerve palsy occurred in the nerve-identified group; however, the incidence of postoperative transient facial nerve palsy did not differ significantly between the identified and nonidentified groups.
Notes: Tumor size was defined as the maximum diameter (tumor thickness) from the superficial to deep lobe of the parotid gland.
Tumor location was determined after resection. Age, tumor size, and operative duration are presented as mean values and analyzed using the Mann–Whitney U test. Sex, histopathological type, tumor location, and postoperative transient facial nerve palsy were analyzed using the Fisher's exact test.
Tumor Size and Nerve Identification
The nerve identification rate was examined by tumor size ([Table 2]). Nerve branches were identified in 10 of 22 cases (45%) with tumors measuring 5 to 10 mm, 9 of 24 cases (38%) with tumors measuring 11 to 15 mm, 7 of 11 cases (64%) with tumors measuring 16 to 20 mm, and 3 of 4 cases (75%) with tumors measuring 21 to 25 mm. Nerve branches were identified in 19 of 46 cases (41%) with tumors measuring ≤15 mm and in 10 of 15 cases (67%) with tumors measuring ≥16 mm; however, the difference between the two groups was not significant (p = 0.136). Analysis of 40 nonanterior tumor cases (16 identified and 24 nonidentified) showed a significantly higher nerve identification rate in tumors measuring ≥16 mm than those measuring ≤15 mm (p = 0.018).
Notes: The number of cases with nerve identified or not identified and the corresponding identification rates are presented for tumor size categories of 5–10, 11–15, 16–20, and 21–25 mm. Among all cases, the identification rate did not differ significantly between tumors ≥16 mm and those ≤15 mm (p = 0.136). Excluding anterior tumors, identification rates were significantly higher for tumors ≥16 mm than for tumors ≤15 mm (p = 0.018). Fisher's exact test and the Mann–Whitney U test were used for statistical analyses. Furthermore, nerve identification rates by tumor locations were compared with the overall rate using the binomial test.
Tumor Size and Nerve Identification by Tumor Location (Anterior–Posterior Direction; Axial Section)
The mean tumor sizes of anterior, medial, and posterior tumors were 10.1, 12.7, and 15.0 mm, respectively, with posterior tumors being significantly larger than anterior tumors (p = 0.001). Tumor size in anterior, medial, or posterior location did not differ significantly between the identified and nonidentified groups ([Table 3A]).
|
(A) Tumor size[a] |
||||
|---|---|---|---|---|
|
Tumor location (axial section) |
Mean tumor size (all cases) |
Mean tumor size (identified cases/nonidentified cases) |
Tumor size (between locations) p-Value |
Tumor size (identified vs. nonidentified) p-Value |
|
Anterior tumor (21 cases) |
10.1 mm |
10.4 mm/9.2 mm (13 cases/8 cases) |
Anterior vs. medial 0.258 |
0.636 |
|
Medial tumor (18 cases) |
12.7 mm |
14.6 mm/10.3 mm (10 cases/8 cases) |
Medial vs. posterior 0.360 |
0.099 |
|
Posterior tumor (22 cases) |
15.0 mm |
17.3 mm/14.2 mm (6 cases/16 cases) |
Posterior vs. anterior 0.001 |
0.138 |
|
(B) Nerve identification[b] |
||||
|
Tumor location (axial section) |
Nerve identification rate (identified cases/all cases) (%) |
Nerve identification rate (between locations) p -Value |
Nerve identification rate (each location vs. all cases) p -Value |
|
|
Anterior tumor (21 cases) |
13/21(62%) |
Anterior vs. medial 0.752 |
0.074 |
|
|
Medial tumor (18 cases) |
10/18 (56%) |
Medial vs. posterior 0.213 |
0.148 |
|
|
Posterior tumor (22 cases) |
6/22 (27%) |
Posterior vs. anterior 0.099 |
0.028 |
|
|
All cases (61 cases) |
29/61(48%) |
|||
Notes: The Kruskal–Wallis test and Fisher's exact test were used for statistical analyses.
a Posterior tumors were significantly larger than anterior tumors (p = 0.001). Within each location, no significant differences in tumor size were observed between the identified and nonidentified cases.
b The nerve identification rates for anterior, medial, and posterior tumors were 62, 56, and 27%, respectively, with no significant differences among locations. Compared with all cases, those with posterior tumors had a significantly lower identification rate (p = 0.028).
The nerve identification rates for anterior, medial, and posterior tumors were 62, 56, and 27%, respectively, with no significant differences observed between the locations. Compared with all cases, those with posterior tumors had a significantly lower nerve identification rate (p = 0.028) ([Table 3B]).
The above results indicate that posterior tumors were significantly larger than anterior tumors but had a significantly lower nerve identification rate than all tumors. Anterior tumors were significantly smaller than posterior tumors; however, their nerve identification rate did not differ significantly from that of tumors in other locations.
Tumor Size and Nerve Identification by Tumor Location (Superior–Inferior Direction; Coronal Section)
The mean sizes of superior, medial, and inferior tumors were 10.6, 10.7, and 15.1 mm, respectively, with inferior tumors significantly larger than medial tumors (p = 0.002) and tending to be larger than superior tumors, although this difference was not significant (p = 0.070). Tumor size in superior, medial, or inferior locations did not differ significantly between the identified and nonidentified groups ([Table 4A]).
|
(A) Tumor size[a] |
||||
|---|---|---|---|---|
|
Tumor location (coronal section) |
Mean tumor size (all cases) |
Mean tumor size (identified cases/nonidentified cases) |
Tumor size (between locations) p-Value |
Tumor size (identified vs. nonidentified) p-Value |
|
Superior tumor (8 cases) |
10.6 mm |
11.3 mm/10.0 mm (4 cases/4 cases) |
Superior vs. medial 0.985 |
0.896 |
|
Medial tumor (26 cases) |
10.7 mm |
10.8 mm/10.6 mm (11 cases/15 cases) |
Medial vs. inferior 0.002 |
0.638 |
|
Inferior tumor (27 cases) |
15.1 mm |
15.8 mm/14.4 mm (14 cases/13 cases) |
Inferior vs. superior 0.070 |
0.330 |
|
(B) Nerve identification[b] |
||||
|
Tumor location (coronal section) |
Nerve identification rate (identified cases/all cases) (%) |
Nerve identification rate (between locations) p -Value |
Nerve identification rate (each location vs. all cases) p -Value |
|
|
Superior tumor (8 cases) |
4/8 (50%) |
Superior vs. medial 1.000 |
0.271 |
|
|
Medial tumor (26 cases) |
11/26 (42%) |
Medial vs. inferior 1.000 |
0.137 |
|
|
Inferior tumor (27 cases) |
14/27 (52%) |
Inferior vs. superior 1.000 |
0.138 |
|
|
All cases (61 cases) |
29/61 (48%) |
|||
Notes: The Kruskal–Wallis test and Fisher's exact test were used for statistical analyses.
a Inferior tumors were significantly larger than medial tumors (p = 0.002) and tended to be larger than superior tumors, although the difference was not significant (p = 0.070). Within each location, no significant differences in tumor size were observed between the nerve-identified and nonidentified cases.
b The nerve identification rates for superior, medial, and inferior tumors were 50, 42, and 52%, respectively, with no significant difference among locations. Compared with all cases, nerve identification rates did not differ significantly by location.
The nerve identification rates for superior, medial, and inferior tumors were 50, 42, and 52%, respectively, with no significant differences among the locations. Compared with all cases, tumors in each location group did not differ significantly in nerve identification rate ([Table 4B]).
Based on the above results, inferior tumors were significantly larger than medial tumors; however, their nerve identification rate did not differ significantly compared with that for tumors in other locations.
Nerve Identification Site by Tumor Location and Cases with Paralysis
The sites and number of cases with identified nerves by tumor location as well as the sites and numbers of cases with paralysis are shown in [Table 5]. Inferior tumors accounted for 10% of 21 cases with anterior tumors, 50% of 18 cases with medial tumors, and 73% of 22 cases with posterior tumors. Among 14 cases with inferior tumors in which nerves were identified, the marginal mandibular branch was identified in 12 cases. Postoperative transient nerve palsy was observed in three cases (numbers in parentheses), including one case with anterior/superior tumor (buccinator paralysis) and two cases with posterior/inferior tumors (marginal mandibular branch paralysis). Nerve exposure was confirmed in all cases. All three transient palsy cases resolved within 2 months.
Notes: Inferior tumors accounted for 10, 50, and 73% of anterior, medial, and superior tumors, respectively. Of the 14 cases with inferior tumor in which nerves were identified, the marginal mandibular branch was identified in 12 cases. The number in parentheses indicates the number of cases with postoperative transient nerve palsy.
Discussion
Currently, PSP is the standard surgical procedure for benign parotid tumors; however, in recent years, the percentage of ECD implementation has been increasing.[13] According to Albergotti et al,[14] compared with SP, ECD was associated with lower incidence rates of postoperative facial nerve palsy and Frey's syndrome; however, the two procedures did not differ significantly in recurrence rate. Xie et al[15] investigated 3,194 cases of benign parotid tumors and concluded that ECD was superior to SP. Furthermore, Kato et al[16] reported that ECD was associated with a shorter length of hospital stay and has medical and economic advantages. However, because studies on ECD have generally focused on small superficial tumors, it cannot be concluded that ECD is an absolutely superior surgical procedure compared to SP and PSP.
PSP is a surgical procedure in which the main trunk and facial nerve branches are systematically identified and protected before tumor resection. In contrast, during ECD, tumors are resected without identifying the main trunk of the facial nerve. From the perspective of preventing postoperative facial nerve palsy, exposure or identification of nerve branches during ECD is acceptable; however, it is considered safer to avoid exposing or identifying nerve branches during surgery. If the indication criteria for ECD require that nerve branches are not exposed or identified, the number of cases eligible for ECD will become more limited.
Currently, no consistent definition exists for the resection margin in ECD.[17] Some reports have recommended leaving a resection margin of a few millimeters in areas where the tumor is sufficiently distant from the nerve[18] [19]; this approach was similar to our surgical procedure. In the present study, the resection margin was determined based on the positional relationship between the tumor and nerve. When the tumor was in contact with or close to the nerve, it was resected along the extracapsular route. In contrast, when the tumor was distant from the nerve, it was removed with a few millimeters to 1 cm of normal parotid tissue attached. Considering the risk of local recurrence of pleomorphic adenoma, we anticipated no additional benefit from performing ECD for tumors distant from the nerve. In all cases with nerve exposure or identification, the nerve was identified in the area of resection along the extracapsular route.
Many studies have determined the indication for ECD based on tumor size and location. One report cited a tumor size criterion of ≤40 mm,[10] whereas several others reported a criterion of ≤25 mm.[8] [9] [13] [14] Regarding tumor location, ECD has been consistently reported to be primarily indicated for superficial tumors in the superficial lobe or lower pole. Many other reports have adopted good mobility as an indication criterion, which generally implies superficial lobe or benign tumors. Based on these reports, our department has defined the indication for ECD as meeting all of the following criteria: superficial tumor, tumor size ≤25 mm, good mobility, and benign tumor. When ECD was performed according to these indication criteria, nerve branches were exposed or identified in 29 of 61 cases (47.5%). Vanroose et al[20] performed ECD on 102 cases in which nonexposure of nerve branches was preoperatively planned but found that nerve branches were identified in 30.4% of cases.
The incidence of transient facial nerve palsy after ECD varied according to the indication criteria, with reported rates ranging from 1.5 to 7.0%.[20] [21] [22] [23] Although these incidence rates are lower than those reported for PSP, postoperative paralysis occurred in a number of cases.[24] In the present study, postoperative transient facial nerve palsy was observed in 3 of 61 cases (4.9%); although not statistically significant, the nerve was identified in all of these cases. Postoperative nerve palsy did not occur in any of the nonidentified cases, suggesting that nerve exposure or identification may contribute to the development of postoperative nerve palsy. Therefore, we focused on cases in which the nerve was identified during ECD. Nerve identification during ECD often involves incidental discovery of nerve branches during surgery and, from the perspective of nerve preservation, it is not considered a reliable surgical approach.
Therefore, we examined the relationship between nerve identification and tumor size and location. Focusing on tumor size alone, the nerve identification rate was 67% in cases with tumors measuring ≥16 mm and 41% in cases with tumors measuring ≤15 mm. The identification rate tended to be higher for cases with tumors measuring ≥16 mm, but the difference was not significant. However, the identification rate was significantly higher in cases with a tumor size of ≥16 mm when cases with anterior tumors were excluded. Furthermore, because factors other than tumor size influenced nerve identification, we focused on tumor location. We examined tumor location in the anterior–posterior direction (axial section) and found that posterior tumors were significantly larger than anterior tumors but had a significantly lower nerve identification rate. This result can be explained by the fact that the facial nerve plane lies deeper in areas posterior to the parotid gland. However, no significant difference in tumor size was observed between identified and nonidentified cases with posterior tumors. Inferior tumors accounted for 73% of posterior tumors when their location was considered in the superior–inferior direction. In general, small inferior tumors rarely contact nerve branches other than the marginal mandibular branch. Therefore, the distance between the tumor and the marginal mandibular branch is likely strongly associated with nerve identification. In other words, tumor location in the superior–inferior direction was more important than tumor size for nerve exposure or identification in posterior tumor cases.
In contrast, anterior tumors were significantly smaller than posterior tumors but did not differ significantly in nerve identification rate. This result may be explained by the nerve running more superficially in areas anterior to the parotid gland. In addition, given the insignificant difference in tumor size between identified and nonidentified cases with anterior tumors, the distance from the parotid capsule to the nerve plane is likely shorter than the tumor size in anterior regions of the parotid gland. Therefore, for anterior tumors, surgeons should exercise caution regarding nerve exposure even when the tumor size is small.[11] Furthermore, all six cases in which the nerve was located superficial to the tumor (deep lobe tumors) involved anterior tumors. These results suggest that ECD should be performed with consideration for nerve identification in anterior tumor cases, in which the nerve runs superficially.
In this study, loupes, microscopes, and exoscopes were not used. However, even if these devices had been used to magnify the surgical field, we believe that the nerve identification rate would have remained unchanged, as nerve exposure was determined based on the anatomical relationship between the tumor and nerve. In addition, in nonidentified cases, FNM was used after resection to check for nerve exposure in the surgical field; however, no new nerves were identified using FNM in any of the cases. This finding suggests that surgical field magnification is unlikely to have reduced the rate of nerve exposure during ECD. Furthermore, the use of exoscopes and microscopes results in no significant difference in the identification of nerve branches.[25]
The indications for ECD are unlikely to decrease in the future. In fact, the number of cases treated with ECD is increasing, and ECD has been reported to be preferred by more than half of patients at facilities with experienced staff.[26] In addition, ECD has been reported to be indicated for larger tumors and low-grade tumors.[27] [28] Psychogios et al[13] considered the indications for ECD and stated that cases with tumors measuring ≤2 mm are suitable candidates, whereas those with tumors measuring 2 to 4 cm are relative candidates. Compared with PSP, ECD has medical and economic advantages, such as lower invasiveness and shorter hospital stay. Moreover, ECD imposes no procedural burden because it can be performed without identifying the main nerve trunk. This suggests that total facial nerve palsy, the most serious postoperative complication of parotidectomy, can be avoided. Meanwhile, exposure and identification of facial nerve branches during ECD and the associated risk of postoperative nerve palsy occur at a manageable rate. Therefore, careful surgical technique informed by a thorough assessment of the tumor size and location along with an understanding of potential nerve involvement is recommended. Moreover, surgeons should be prepared to convert from ECD to PSP at any time point based on intraoperative findings. Multiple reports have emphasized that ECD should be performed by surgeons with substantial experience in parotidectomy.[15] [16] [29]
A limitation of this study is the relatively small sample size (61 cases). Stratification by tumor location further reduced the number of cases, limiting the ability to detect significant differences. Further studies with larger cohorts are needed to more precisely clarify the relationships between tumor size and location and facial nerve exposure or identification. In addition, recurrence at the resection margin remains a concern following ECD. In our study, no recurrences were observed over a mean postoperative follow-up of approximately 5 years; nevertheless, longer-term follow-up is warranted to fully assess this risk.
Conclusion
Although ECD does not involve the identification of the main trunk of the facial nerve, its branches may be exposed or identified during surgery. In this study, among 61 cases in which patients underwent ECD under the criteria of tumor size ≤25 mm, superficial location, good mobility, and benign pathology, facial nerve branches were exposed or identified in 29 cases. All cases that developed postoperative transient facial nerve palsy occurred in patients in whom the nerve was identified. When anterior tumors were excluded to focus on medial and posterior tumors, the nerve identification rate was significantly higher in cases with tumors measuring ≥16 mm. Compared with anterior tumors, posterior tumors were significantly larger and had a significantly lower nerve identification rate. Although anterior tumors were smaller than posterior tumors, their nerve identification rate did not differ significantly from tumors in other locations. These results could be attributed to tumor location and nerve plane. Nerve exposure or identification during ECD poses a risk of postoperative transient facial nerve palsy. Therefore, the findings of this study highlight the importance of preoperative assessment of the likelihood of nerve identification based on tumor size and location.
Conflict of Interest
None declared.
-
References
- 1 Rawson AJ, Howard JM, Royster HP, Horn Jr RC. Tumors of the salivary glands; a clinicopathological study of 160 cases. Cancer 1950; 3 (03) 445-458
- 2 Guntinas-Lichius O, Klussmann JP, Wittekindt C, Stennert E. Parotidectomy for benign parotid disease at a university teaching hospital: outcome of 963 operations. Laryngoscope 2006; 116 (04) 534-540
- 3 Zernial O, Springer IN, Warnke P, Härle F, Risick C, Wiltfang J. Long-term recurrence rate of pleomorphic adenoma and postoperative facial nerve paresis (in parotid surgery). J Craniomaxillofac Surg 2007; 35 (03) 189-192
- 4 O'Brien CJ. Current management of benign parotid tumors—the role of limited superficial parotidectomy. Head Neck 2003; 25 (11) 946-952
- 5 Liu H-T, Jiang W-P, Xia G, Liao J-M. Evaluation of the effectiveness of superficial parotidectomy and partial superficial parotidectomy for benign parotid tumours: a meta-analysis. J Otolaryngol Head Neck Surg 2023; 52 (01) 86
- 6 Dallera P, Marchetti C, Campobassi A. Local capsular dissection of parotid pleomorphic adenomas. Int J Oral Maxillofac Surg 1993; 22 (03) 154-157
- 7 McGurk M, Renehan A, Gleave EN, Hancock BD. Clinical significance of the tumour capsule in the treatment of parotid pleomorphic adenomas. Br J Surg 1996; 83 (12) 1747-1749
- 8 Kawata R, Terada T, Higashino M. et al. Extracapsular dissection for parotid tumors: comparison with partial superficial parotidectomy. Nippon Jibiinkoka Gakkai Kaiho 2021; 124: 205-210
- 9 Witt RL. Minimally invasive surgery for parotid pleomorphic adenoma. Ear Nose Throat J 2005; 84 (05) 308 , 310–311
- 10 Foresta E, Torroni A, Di Nardo F. et al. Pleomorphic adenoma and benign parotid tumors: extracapsular dissection vs superficial parotidectomy—review of literature and meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol 2014; 117 (06) 663-676
- 11 Omura S, Kawata R, Haginomori SI. et al. Effective surgical management of anterior tumors of the parotid gland: main trunk method vs. peripheral Smethod. Am J Otolaryngol 2021; 42 (04) 102964
- 12 Ichihara T, Kawata R, Higashino M, Terada T, Haginomori S. A more appropriate clinical classification of benign parotid tumors: investigation of 425 cases. Acta Otolaryngol 2014; 134 (11) 1185-1191
- 13 Psychogios G, Bohr C, Constantinidis J. et al. Review of surgical techniques and guide for decision making in the treatment of benign parotid tumors. Eur Arch Otorhinolaryngol 2021; 278 (01) 15-29
- 14 Albergotti WG, Nguyen SA, Zenk J, Gillespie MB. Extracapsular dissection for benign parotid tumors: a meta-analysis. Laryngoscope 2012; 122 (09) 1954-1960
- 15 Xie S, Wang K, Xu H. et al. PRISMA-extracapsular dissection versus superficial parotidectomy in treatment of benign parotid tumors: evidence from 3194 patients. Medicine (Baltimore) 2015; 94 (34) e1237
- 16 Kato MG, Erkul E, Nguyen SA. et al. Extracapsular dissection vs superficial parotidectomy of benign parotid lesions: surgical outcomes and cost-effectiveness analysis. JAMA Otolaryngol Head Neck Surg 2017; 143 (11) 1092-1097
- 17 Quer M, Hernandez-Prera JC, Silver CE. et al. Current trends and controversies in the management of Warthin tumor of the parotid gland. Diagnostics (Basel) 2021; 11 (08) 1467
- 18 Klintworth N, Zenk J, Koch M, Iro H. Postoperative complications after extracapsular dissection of benign parotid lesions with particular reference to facial nerve function. Laryngoscope 2010; 120 (03) 484-490
- 19 Zbären P, Vander Poorten V, Witt RL. et al. Pleomorphic adenoma of the parotid: formal parotidectomy or limited surgery?. Am J Surg 2013; 205 (01) 109-118
- 20 Vanroose R, Scheerlinck J, Coopman R, Nout E. Clinical outcomes and cost-effectiveness of superficial parotidectomy versus extracapsular dissection of the parotid gland: a single-centre retrospective study of 161 patients. Int J Oral Maxillofac Implants 2023; 52 (02) 191-198
- 21 Barca I, Cristofaro MG. Surgical approach to parotid pleomorphic adenoma: a 15-year retrospective cohort study. Br J Oral Maxillofac Surg 2020; 58 (06) 659-662
- 22 Bonavolontà P, Dell'Aversana Orabona G, Maglitto F. et al. Postoperative complications after removal of pleomorphic adenoma from the parotid gland: a long-term follow up of 297 patients from 2002 to 2016 and a review of publications. Br J Oral Maxillofac Surg 2019; 57 (10) 998-1002
- 23 Dell'Aversana Orabona G, Bonavolontà P, Iaconetta G, Forte R, Califano L. Surgical management of benign tumors of the parotid gland: extracapsular dissection versus superficial parotidectomy—our experience in 232 cases. J Oral Maxillofac Surg 2013; 71 (02) 410-413
- 24 Kawata R, Kinoshita I, Omura S. et al. Risk factors of postoperative facial palsy for benign parotid tumors: outcome of 1,018 patients. Laryngoscope 2021; 131 (12) E2857-E2864
- 25 Bartkowiak E, Łuczewski Ł, Chou JT, Wierzbicka M. Is the 3D exoscope better than the surgical microscope in parotid surgery: a prospective, randomized single-center study. Eur Arch Otorhinolaryngol 2022; 279 (02) 1029-1034
- 26 Bär B, Mantsopoulos K, Iro H. Paradigm shift in surgery for benign parotid tumors: 19 years of experience with almost 3000 cases. Laryngoscope 2020; 130 (08) 1941-1946
- 27 Auger SR, Kramer DE, Hardy B. et al. Functional outcomes after extracapsular dissection with partial facial nerve dissection for small and large parotid neoplasms. Am J Otolaryngol 2021; 42 (01) 102770
- 28 Mantsopoulos K, Koch M, Iro H. Extracapsular dissection as sole therapy for small low-grade malignant tumors of the parotid gland. Laryngoscope 2017; 127 (08) 1804-1807
- 29 Allevi F, Borzi P, Valsecchi F. et al. The extracapsular dissection technique in the management of benign tumours of the parotid gland: our experience in 194 patients. J Laryngol Rhinol Otol 2024; 138 (05) 565-569
Address for correspondence
Publikationsverlauf
Eingereicht: 15. April 2025
Angenommen: 06. August 2025
Artikel online veröffentlicht:
11. Dezember 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Rawson AJ, Howard JM, Royster HP, Horn Jr RC. Tumors of the salivary glands; a clinicopathological study of 160 cases. Cancer 1950; 3 (03) 445-458
- 2 Guntinas-Lichius O, Klussmann JP, Wittekindt C, Stennert E. Parotidectomy for benign parotid disease at a university teaching hospital: outcome of 963 operations. Laryngoscope 2006; 116 (04) 534-540
- 3 Zernial O, Springer IN, Warnke P, Härle F, Risick C, Wiltfang J. Long-term recurrence rate of pleomorphic adenoma and postoperative facial nerve paresis (in parotid surgery). J Craniomaxillofac Surg 2007; 35 (03) 189-192
- 4 O'Brien CJ. Current management of benign parotid tumors—the role of limited superficial parotidectomy. Head Neck 2003; 25 (11) 946-952
- 5 Liu H-T, Jiang W-P, Xia G, Liao J-M. Evaluation of the effectiveness of superficial parotidectomy and partial superficial parotidectomy for benign parotid tumours: a meta-analysis. J Otolaryngol Head Neck Surg 2023; 52 (01) 86
- 6 Dallera P, Marchetti C, Campobassi A. Local capsular dissection of parotid pleomorphic adenomas. Int J Oral Maxillofac Surg 1993; 22 (03) 154-157
- 7 McGurk M, Renehan A, Gleave EN, Hancock BD. Clinical significance of the tumour capsule in the treatment of parotid pleomorphic adenomas. Br J Surg 1996; 83 (12) 1747-1749
- 8 Kawata R, Terada T, Higashino M. et al. Extracapsular dissection for parotid tumors: comparison with partial superficial parotidectomy. Nippon Jibiinkoka Gakkai Kaiho 2021; 124: 205-210
- 9 Witt RL. Minimally invasive surgery for parotid pleomorphic adenoma. Ear Nose Throat J 2005; 84 (05) 308 , 310–311
- 10 Foresta E, Torroni A, Di Nardo F. et al. Pleomorphic adenoma and benign parotid tumors: extracapsular dissection vs superficial parotidectomy—review of literature and meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol 2014; 117 (06) 663-676
- 11 Omura S, Kawata R, Haginomori SI. et al. Effective surgical management of anterior tumors of the parotid gland: main trunk method vs. peripheral Smethod. Am J Otolaryngol 2021; 42 (04) 102964
- 12 Ichihara T, Kawata R, Higashino M, Terada T, Haginomori S. A more appropriate clinical classification of benign parotid tumors: investigation of 425 cases. Acta Otolaryngol 2014; 134 (11) 1185-1191
- 13 Psychogios G, Bohr C, Constantinidis J. et al. Review of surgical techniques and guide for decision making in the treatment of benign parotid tumors. Eur Arch Otorhinolaryngol 2021; 278 (01) 15-29
- 14 Albergotti WG, Nguyen SA, Zenk J, Gillespie MB. Extracapsular dissection for benign parotid tumors: a meta-analysis. Laryngoscope 2012; 122 (09) 1954-1960
- 15 Xie S, Wang K, Xu H. et al. PRISMA-extracapsular dissection versus superficial parotidectomy in treatment of benign parotid tumors: evidence from 3194 patients. Medicine (Baltimore) 2015; 94 (34) e1237
- 16 Kato MG, Erkul E, Nguyen SA. et al. Extracapsular dissection vs superficial parotidectomy of benign parotid lesions: surgical outcomes and cost-effectiveness analysis. JAMA Otolaryngol Head Neck Surg 2017; 143 (11) 1092-1097
- 17 Quer M, Hernandez-Prera JC, Silver CE. et al. Current trends and controversies in the management of Warthin tumor of the parotid gland. Diagnostics (Basel) 2021; 11 (08) 1467
- 18 Klintworth N, Zenk J, Koch M, Iro H. Postoperative complications after extracapsular dissection of benign parotid lesions with particular reference to facial nerve function. Laryngoscope 2010; 120 (03) 484-490
- 19 Zbären P, Vander Poorten V, Witt RL. et al. Pleomorphic adenoma of the parotid: formal parotidectomy or limited surgery?. Am J Surg 2013; 205 (01) 109-118
- 20 Vanroose R, Scheerlinck J, Coopman R, Nout E. Clinical outcomes and cost-effectiveness of superficial parotidectomy versus extracapsular dissection of the parotid gland: a single-centre retrospective study of 161 patients. Int J Oral Maxillofac Implants 2023; 52 (02) 191-198
- 21 Barca I, Cristofaro MG. Surgical approach to parotid pleomorphic adenoma: a 15-year retrospective cohort study. Br J Oral Maxillofac Surg 2020; 58 (06) 659-662
- 22 Bonavolontà P, Dell'Aversana Orabona G, Maglitto F. et al. Postoperative complications after removal of pleomorphic adenoma from the parotid gland: a long-term follow up of 297 patients from 2002 to 2016 and a review of publications. Br J Oral Maxillofac Surg 2019; 57 (10) 998-1002
- 23 Dell'Aversana Orabona G, Bonavolontà P, Iaconetta G, Forte R, Califano L. Surgical management of benign tumors of the parotid gland: extracapsular dissection versus superficial parotidectomy—our experience in 232 cases. J Oral Maxillofac Surg 2013; 71 (02) 410-413
- 24 Kawata R, Kinoshita I, Omura S. et al. Risk factors of postoperative facial palsy for benign parotid tumors: outcome of 1,018 patients. Laryngoscope 2021; 131 (12) E2857-E2864
- 25 Bartkowiak E, Łuczewski Ł, Chou JT, Wierzbicka M. Is the 3D exoscope better than the surgical microscope in parotid surgery: a prospective, randomized single-center study. Eur Arch Otorhinolaryngol 2022; 279 (02) 1029-1034
- 26 Bär B, Mantsopoulos K, Iro H. Paradigm shift in surgery for benign parotid tumors: 19 years of experience with almost 3000 cases. Laryngoscope 2020; 130 (08) 1941-1946
- 27 Auger SR, Kramer DE, Hardy B. et al. Functional outcomes after extracapsular dissection with partial facial nerve dissection for small and large parotid neoplasms. Am J Otolaryngol 2021; 42 (01) 102770
- 28 Mantsopoulos K, Koch M, Iro H. Extracapsular dissection as sole therapy for small low-grade malignant tumors of the parotid gland. Laryngoscope 2017; 127 (08) 1804-1807
- 29 Allevi F, Borzi P, Valsecchi F. et al. The extracapsular dissection technique in the management of benign tumours of the parotid gland: our experience in 194 patients. J Laryngol Rhinol Otol 2024; 138 (05) 565-569