

Subscribe to RSS
DOI: 10.1055/s-0045-1814755
Balloon-Assisted Redirection: A Novel Endoscopic Technique for Complex Biliary Injury Post-Cholecystectomy
Authors

Case
A 52-year-old female presented with abdominal pain, nausea, and persistent bilious drainage (200–300 mL/day) for 30 days following open cholecystectomy. Three months earlier, she had biliary pancreatitis and choledocholithiasis, managed by endoscopic retrograde cholangiopancreatography (ERCP) with stone extraction and placement of a 10 Fr × 7 Cm biliary plastic stent. After symptomatic improvement, she underwent elective cholecystectomy at an outside hospital, which was converted into an open procedure due to dense adhesions, and a drain was placed in the gallbladder fossa.
Postoperatively, she continued to have high-output bilious drainage without jaundice. A repeat ERCP elsewhere showed stent migration, a tight common hepatic duct (CHD) proximal CBD stricture, and failure to access the upstream duct. She was referred to our center.
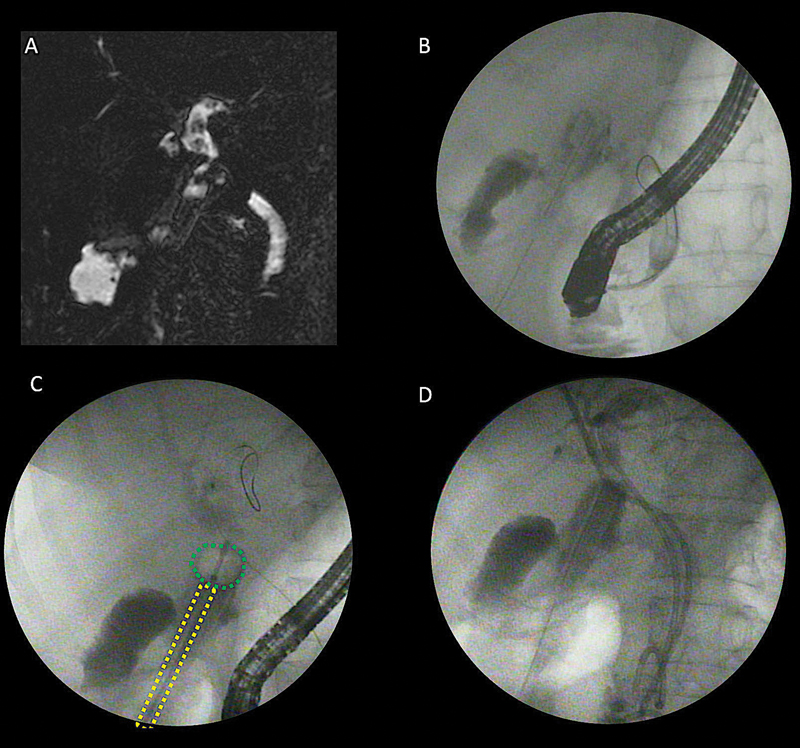
On admission, she was afebrile but nutritionally depleted. Magnetic resonance cholangiopancreatography revealed a 23-mm-long CHD-proximal CBD stricture and peri-cholecystic collection. Given the ongoing bile leak and poor surgical fitness, repeat ERCP was planned. Cholangiogram showed extravasation of contrast from the proximal CBD with a cutoff at the CHD site. The guidewire repeatedly entered into the leak site during ERCP. To prevent the entry of the guidewire into the leak, a novel “balloon-assisted redirection” technique was employed. A 0.025 guidewire (VisiGlide, Olympus, Tokyo, Japan) was passed through a percutaneous drain, followed by a biliary balloon catheter (Extractor, Boston Scientific, Massachusetts, United States). A balloon was positioned at the leak site and inflated (to 10 mm), which enabled the successful entry of the guidewire into the upstream duct. Both right and left ducts were opacified, and two biliary plastic stents were placed ([Fig. 1A–D]; [Video 1]). Bile output reduced to <20 mL/day within a week. The drain was removed at 2 weeks with good clinical recovery.
Practical Implications for Endoscopists
-
Post-cholecystectomy bile duct injuries can be effectively managed with ERCP.
-
However, certain complex bile duct injuries pose significant challenges for endotherapy and often necessitate second surgery, which carries substantial mortality and morbidity.[1]
-
The large defect in CBD prevents successful guidewire passage into the upstream or downstream duct during ERCP or PTBD approach, respectively.
-
The novel balloon-assisted redirection technique, placed through an existing percutaneous drain tract, facilitates guidewire maneuvering and successful entry into the upstream intrahepatic duct during ERCP.
-
Compared with coils or glue used percutaneously to block a leak, the balloon-assisted approach provides a simple, reproducible, and reversible alternative without depositing embolic material.[2] [3]
-
References
- 1 Tringali A, Costa D, Ramai D. Endoscopic management of biliary leaks: Where are we now?. World J Gastrointest Endosc 2025; 17 (07) 107587
- 2 Wahaibi AA, Alnaamani K, Alkindi A, Qarshoubi IA. A novel endoscopic treatment of major bile duct leak. Int J Surg Case Rep 2014; 5 (04) 189-192
- 3 Dutra B, Welborn M, Thosani NC, Badillo R, DaVee T, Bhakta D. Endoscopic coil embolization for refractory intrahepatic biliary duct leak. ACG Case Rep J 2022; 9 (02) e00743
Address for correspondence
Publication History
Article published online:
06 January 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Tringali A, Costa D, Ramai D. Endoscopic management of biliary leaks: Where are we now?. World J Gastrointest Endosc 2025; 17 (07) 107587
- 2 Wahaibi AA, Alnaamani K, Alkindi A, Qarshoubi IA. A novel endoscopic treatment of major bile duct leak. Int J Surg Case Rep 2014; 5 (04) 189-192
- 3 Dutra B, Welborn M, Thosani NC, Badillo R, DaVee T, Bhakta D. Endoscopic coil embolization for refractory intrahepatic biliary duct leak. ACG Case Rep J 2022; 9 (02) e00743