

Subscribe to RSS
DOI: 10.1055/s-0045-1814756
Biliary Drainage in Altered Anatomy: A Comprehensive Literature Review
Authors

Abstract
Endoscopic retrograde cholangiopancreatography (ERCP), introduced in 1968, remains the gold standard for managing pancreatobiliary disorders, achieving success rates of nearly 95% in patients with normal anatomy. However, modern surgical interventions, such as Roux-en-Y gastric bypass (RYGB), hepaticojejunostomy, pancreaticoduodenectomy (Whipple procedure), and Billroth II gastrectomy, result in surgically altered anatomies (SAA), complicating biliary interventions due to anatomical distortions, including long afferent limbs and sharp intestinal angulations. Device-assisted enteroscopy-based ERCP (DAE-ERCP), including double-balloon, single-balloon, and spiral enteroscopy, has improved access in SAA, especially RYGB patients, with technical success rates as high as 95%; however, it remains technically demanding and time-intensive. Laparoscopy-assisted ERCP demonstrates a higher technical success rate (>95%), but carries increased invasiveness, prolonged procedure times, and higher adverse event rates, limiting its routine use. Endoscopic ultrasound-guided biliary drainage, comprising rendezvous technique, transmural drainage such as choledochoduodenostomy (CDS) and hepaticogastrostomy (HGS), and antegrade interventions, has emerged as a reliable alternative, showing superior technical success and lower complication rates compared with percutaneous transhepatic biliary drainage. Specifically, EUS-guided transmural techniques (HGS, CDS) offer effective internal drainage in anatomies where conventional approaches fail. The recently developed EUS-directed transgastric ERCP procedure, utilizing lumen-apposing metal stents to create temporary gastro-gastric or jejuno-gastric fistulas, has revolutionized biliary interventions in RYGB, achieving high technical and clinical success rates. Novel and hybrid approaches, including magnetic compression anastomosis, artificial intelligence-assisted navigation, and biodegradable stents, continue to enhance therapeutic possibilities, underscoring an evolving multidisciplinary landscape for biliary interventions in surgically altered anatomy.
Keywords
ERCP - biliary drainage - surgically altered anatomy - device-assisted enteroscopy - EDGE procedure - EUS-guided biliary drainage - Roux-en-Y gastric bypassIntroduction
Since its inception in 1968, endoscopic retrograde cholangiopancreatography (ERCP) has been regarded as the gold standard for diagnosing and managing pancreatobiliary diseases, with success rates close to 95% in cases with normal anatomy.[1] [2] The advent of modern surgical techniques, such as Roux-en-Y gastric bypass (RYGB), hepaticojejunostomy with Roux-en-Y, pancreaticoduodenectomy (Whipple procedure), and Billroth II gastrectomy, poses increasing challenges to the successful execution of ERCP-related procedures. These surgeries result in surgically altered anatomy (SAA), characterized by long afferent limbs, acute angulations of the small bowel, and biliodigestive anastomoses (BDA), all of which complicate identification and cannulation of the biliary tract.[3]
Over recent decades, the rise in pancreaticoduodenectomies has been accompanied by biliary complications, such as biliary leaks, which occur in 2 to 9% of cases, most commonly at the site of hepaticojejunostomy.[4] With the ongoing obesity pandemic, one expects a steady increase in bariatric surgeries, and hence, the prevalence of SAA is expected to rise further.[5] Given the heightened risk of biliary complications associated with morbid obesity and rapid weight loss, the demand for technically complex endoscopic interventions in patients with SAA will continue to grow.[6]
Endoscopic access and therapeutic interventions in patients with SAA remain technically complex, often requiring device-assisted enteroscopy (DAE), laparoscopy-assisted ERCP (LA-ERCP), endoscopic-ultrasound-guided biliary drainage (EUS-BD), or percutaneous and surgical alternatives. As the prevalence of altered anatomy continues to rise due to growing surgical volumes, understanding the evolving strategies, success rates, limitations, and innovations in biliary intervention is critical.
This review aims to provide a comprehensive overview of the challenges, available techniques, and clinical outcomes associated with biliary interventions in patients with SAA.
Anatomical Considerations
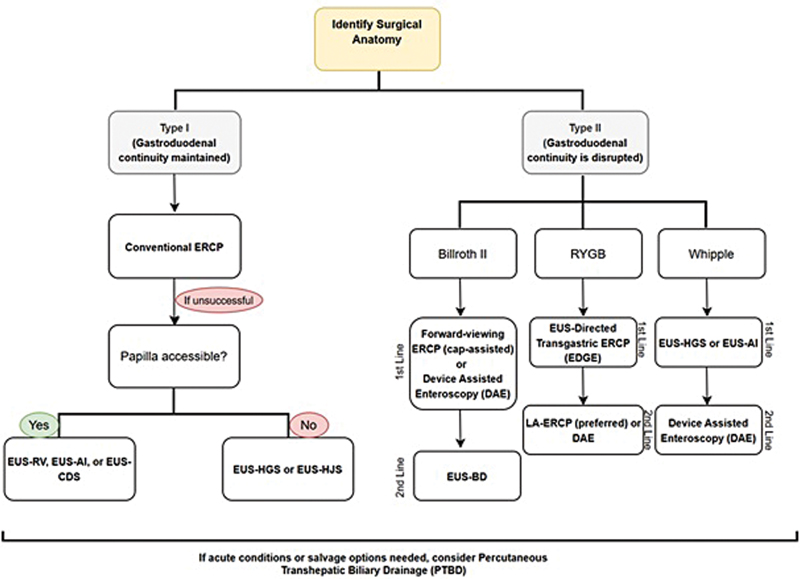
Effective biliary drainage in patients with SAA primarily depends on overcoming three critical challenges: navigating the afferent limb to reach the biliopancreatoenteric anastomosis or ampulla, achieving successful cannulation of the bile or pancreatic ducts within the new anatomical orientation, and performing the necessary diagnostic or therapeutic interventions safely.[7] To guide the endoscopic approach, surgical anatomies have been grouped into two categories,[8] as shown in [Fig. 1]:

Type I: In this group, the duodenum remains in continuation with the gastric remnant. This occurs in procedures where the stomach (or part of it) is still connected to the duodenum. Examples are sleeve gastrectomy (vertical sleeve resection of the stomach) and Billroth I gastrectomy (distal gastrectomy with gastroduodenostomy).
Type II: In this group, the normal gastric-duodenal pathway is disrupted, which means the duodenum and papilla are not in continuity with the upper GI tract. The stomach may be bypassed, removed, or separated from the duodenum. Examples include Billroth II gastrectomy (gastrojejunostomy with an afferent loop), RYGB for obesity (gastrojejunostomy with an excluded stomach and a long Roux limb), Roux-en-Y hepaticojejunostomy (surgical biliary bypass, often after bile duct injury, liver transplantation, or tumor), and Whipple procedure (pancreaticoduodenectomy with gastrojejunostomy and hepaticojejunostomy).[9]
Conventional Endoscopic Retrograde Cholangiopancreatography in Altered Anatomy
A side-viewing duodenoscope is typically the instrument of choice for performing ERCP due to its ability to visualize the biliary anastomosis site, allowing biliary drainage to be achieved using conventional cannulation techniques even in altered anatomy.[10]
In Type I reconstructions, those maintaining continuity between stomach and duodenum, such as Billroth I gastrectomy or sleeve gastrectomy, a standard side-viewing duodenoscope can often reach the papilla with minimal issue, with comparable success rates.[9]
However, Type II anatomies in which the duodenum is excluded or relocated (e.g., Billroth II gastrojejunostomy, RYGB, Whipple procedure) will present major challenges in maneuvering the duodenoscope to the papilla.[9] Hence, duodenoscopes, gastroscopes, and colonoscopes have been used across different studies in patients with SAA, but there is no clear consensus established regarding the optimal endoscopic approach.
In Billroth II anatomy, the difficulty arises from the challenge of selectively intubating the afferent limb due to the sharp angulation between the gastric remnant and small bowel and the limited visualization of the papilla, which is often hidden behind mucosal folds. Hence, the conventional side-viewing scope is difficult to use as it presents a side view, is rigid, and relatively large diameter, thereby increasing the risk of injury to the small bowel or gastrojejunal anastomosis.[11] Fugazza et al examined a new technique, underwater cap-assisted ERCP (u-ERCP), in which a transparent plastic cap is fitted onto the tip of a forward-viewing endoscope (gastroscope or colonoscope). In six patients with SAA, they reported 100% technical success with no adverse events.[12] Lee et al similarly evaluated the use of a cap-assisted regular colonoscope for ERCP and reported an intubation success rate of 74.4% without adverse events, with side-to-side jejunojejunostomy showing the highest rates.[13] The transparent cap enhances papilla visualization and stability, facilitating deep biliary cannulation by maintaining the catheter tip in the optimal position for the common bile duct access. Cannulation can then be achieved either by directly pushing the catheter or by suctioning the papilla into the cap for passive advancement.[14] Additionally, in a recent single-center study comparing cap-assisted gastroscopes and duodenoscopes, both had similar success and complication rates on patients with Billroth II anatomy, though duodenoscopes had shorter cannulation times, potentially reducing pancreatitis risk.[10]
According to the European Society of Gastrointestinal Endoscopy (ESGE) guidelines from 2016, experienced endoscopists prefer side-viewing endoscopes due to the presence of an elevator and a large working channel, which helps in better papilla identification.[15] However, in Billroth II anatomy, limited visibility with the side-viewing scope makes forward-viewing endoscopes relatively easier and safer to use.[12] A meta-analysis in 2018 reported higher success rates with forward-viewing endoscopy (with or without cap) compared with side-viewing scopes in Billroth II anatomy (90.3 vs. 86.8%, cannulation up to 93.7% with cap), making it a safer first option for less experienced endoscopists.[16]
Traditional ERCP using a standard duodenoscope is technically challenging in RYGB patients due to the need to navigate through lengthy Roux limbs (80–150 cm) to access the papilla.[17] Various attempts have been recorded with pediatric colonoscopes dating back to as early as 1988.[18] However, even combined techniques have also shown only a 33 to 67% success rate despite multiple attempts, with the lowest being with a conventional duodenoscope.[17]
In the Whipple procedure (pancreaticoduodenectomy), ERCP is also faced with significant challenges, such as inability to access the affected limb and identification of the ductal anastomosis (choledochojejunostomy or pancreaticojejunostomy). Despite using gastroscopes or enteroscopes, afferent limb intubation remained difficult. Overall technical success rate ranged from 51 to 62% across various studies, with complication rates at 2%.[19]
These limitations prompted the development of DAE and alternate access methods discussed below.
Device-Assisted Enteroscopy-ERCP
Enteroscopes were originally utilized for the diagnosis and management of small bowel disorders.[17] However, a case series by Aabakken et al in 2006 demonstrated that double-balloon enteroscopy (DBE) is a safe and feasible option for achieving endoscopic access and biliary cannulation in patients with Roux-en-Y anatomy.[20] Since then, different balloon-assisted or rotational overtube-assisted techniques, such as DBE, single-balloon enteroscopy (SBE), and spiral enteroscopy (SE), have been increasingly utilized to perform ERCP, particularly in patients with RYGB.[17] A schematic illustration is summarized in [Fig. 2]. While traditional long enteroscopes (200 cm) with smaller channels (2.8 mm) limited the use of standard ERCP tools, the development of short DBE and SBE scopes (155 cm) with wider 3.2 mm channels has helped overcome these limitations.[9]

Among DAE systems, DBE uses balloons on both the endoscope and the overtube, while SBE has a single balloon on the overtube, simplifying setup and reducing procedure time. DBE advances through a push-and-pull mechanism using alternating balloon inflation, whereas SBE relies on tip angulation and bowel wall suction (“hook-and-suck”) for scope stability. SE uses a rotating overtube to pleat the bowel onto the endoscope, allowing deep advancement with a clockwise rotation combined with forward pressure. These techniques offer deeper small bowel access, expanding therapeutic ERCP options in patients with complex postsurgical anatomy.[21]
In Type I reconstructions, DAE-ERCP is hardly ever required.[22] In Type II anatomy, the success rate of DAE-ERCP is the highest in Billroth II anatomy, followed by pancreaticoduodenectomy and Roux-en-Y hepaticojejunostomy, with the lowest success rates in patients with RYGB. Cannulation rates appeared to be equivalent in patients with both native papilla and biliary-enteric or pancreaticoenteric anastomosis. This was mostly dependent on limb length.[23]
While DAE achieves technical success rates of 95 to 100% in Billroth II and overcomes the anatomical challenges of the afferent limb, it remains technically demanding and limited by a lack of en face papillary views.[24] A meta-analysis by Skinner et al reported a 70% success rate for device-assisted ERCP (SBE, DBE, spiral) in RYGB patients, with no significant differences between enteroscope types or access routes.[23] Similar findings by De Koning and Moreels showed lower success with long-limb RYGB and comparable adverse event rates for DBE (10%) and SBE (8%), mostly managed conservatively.[25] In Whipple anatomy, SBE has shown technical success rates of up to 90% without serious adverse events.[26] ERCP with DBE is limited by its small channel size, allowing only 7-Fr stents and fewer accessory options. While the overtube helps maintain scope position and aids cannulation by allowing torque, the endoscopic view remains oblique rather than en face, even in optimal conditions. Similar drawbacks are seen in SBE.[27] Although insertion success rates were similar for both long and short DBEs, Katanuma and Isayama noted that short DBEs were more operator-friendly due to enhanced control, increased insertion force, and improved compatibility with therapeutic devices.[28] The major published outcomes of DAE in SAA are summarized in [Tables 1] to [3], stratified by double-balloon, single-balloon, and SE, respectively.
|
First author (year) |
Study type |
Anatomy |
Endoscopy success rate |
ERCP Success rate |
Adverse events |
AGREE classification |
|---|---|---|---|---|---|---|
|
Long scope DBE |
||||||
|
Aabakken (2007)[20] |
Retrospective |
Variable |
93% (14/15) |
80% (12/15) |
0% |
Mild/Moderate: No major AEs reported |
|
Emmett (2007)[95] |
Retrospective |
Variable |
80% (4/5) |
80% (4/5) |
0% |
Mild/Moderate: No major AEs reported |
|
Maaser (2008)[96] |
Retrospective |
Variable |
73% (8/11) |
NR |
0% |
Mild/Moderate: No AEs reported |
|
Mönkemüller (2009)[97] |
Retrospective |
Variable |
94.1% (16/17) |
NR |
5.8% (1/17); perforation necessitating surgery (1) |
Severe: 1 perforation requiring surgery (Grade 3) |
|
Moreels (2009)[98] |
Retrospective |
Variable |
86.70% |
NR |
6.6% (1/15); perforation requiring surgery (1) |
Severe: 1 perforation requiring surgery (Grade 3) |
|
Parlak (2011)[99] |
Retrospective |
RYHJ |
92.90% |
NR |
4.8% (1/21); retroperitoneal air |
Mild: Retroperitoneal air (Grade 1–2) |
|
Raithel (2011)[100] |
Retrospective |
Variable |
74% |
NR |
5.8% (5/86); perforation necessitating surgery (2); bleeding(1); pancreatitis(2) |
Mild/Moderate: Perforation requiring surgery (Grade 3), bleeding (Grade 2), pancreatitis (Grade 2) |
|
Liu (2017)[101] |
Retrospective |
RYGB |
75.6% (65/86) |
NR |
2/86 procedures (2%) |
Mild: 2/86 procedures (2%) AE, likely Grade 1–2 |
|
Kashani (2018)[102] |
Retrospective |
RYGB |
93.8% (121/129) |
NR |
Overall adverse event rates were 11% (12/109) and 5% (1/20) for operators A and B |
Mild/Moderate: 11% (12/109) AE Operator A; 5% (1/20) Operator B |
|
Short scope DBE |
||||||
|
Shimatani (2009)[103] |
Retrospective |
Variable |
97% (100/103) |
NR |
5% (5/103); Perforation (5) with 1 requiring surgery |
Mild/Severe: 5% (5/103); 1 required surgery (Grade 3) |
|
Tsujino (2010)[104] |
Retrospective |
Variable |
100% (6/6) |
NR |
33% (2/6); Cholangitis (1); retroperitoneal air (2) |
Moderate/Severe: 33% (2/6); cholangitis (Grade 2), retroperitoneal air (Grade 1–2 |
|
Cho (2011)[105] |
Retrospective |
Variable |
86.2% (25/29) |
NR |
0% (0/29) |
Mild: 0% AE |
|
Itoi (2010)[106] |
Retrospective |
Variable |
100% (9/9) |
NR |
0% |
Mild: 0% AE |
|
Osoegawa (2012)[107] |
Retrospective |
Variable |
96% (47/49) |
NR |
2.1% (1/47); Perforation requiring surgery (1) |
Moderate/Severe: 2.1% (1/47); perforation requiring surgery (Grade 3) |
|
Park (2013)[108] |
Retrospective |
Variable |
80% (8/10) |
NR |
0% |
Mild: 0% AE |
|
Siddiqui (2013)[109] |
Retrospective |
Variable |
89% (71/79) |
NR |
5% (4/79); Pancreatitis (3); bleeding (1) |
Mild/Moderate: 5% (4/79); pancreatitis (Grade 2), bleeding (Grade 2) |
|
Tsutsumi (2015)[110] |
Retrospective |
Variable |
98.6% (71/72) |
NR |
3% with cholangitis (conservative management) |
Mild/Moderate: 3% cholangitis, conservative (Grade 1–2 |
|
Cheng (2015)[111] |
Retrospective |
Bilroth II |
94.8% (73/77) |
NR |
6.50% |
Mild/Moderate: 6.5% AE |
|
Shimatani (2016)[112] |
Prospective |
Variable |
97.7% (304/311) |
NR |
10.6% (33 patients) |
Mild/Moderate: 10.6% AE |
|
Uchida (2020)[113] |
Retrospective |
Variable |
94.3% (759/805) |
NR |
5.50% |
Mild/Moderate: 5.5% AE |
|
Ishihara (2021)[114] |
Retrospective |
Variable |
92% |
NR |
6.80% |
Mild/Moderate: 6.8% AE |
Notes: Endoscopy success rate refers to technical success (successful advancement to the papilla or biliary anastomosis). ERCP success rate refers to therapeutic success (successful cannulation and/or completion of intended intervention). Adverse events are stratified by severity according to the AGREE classification.
|
First author (year) |
Study type |
Anatomy |
Endoscopy success rate |
ERCP success rate |
Adverse events |
AGREE classification |
|---|---|---|---|---|---|---|
|
Single-balloon enteroscopy |
||||||
|
Neumann (2009)[115] |
Retrospective |
Variable |
77% (10/13) |
NR |
0% |
0% |
|
Itoi (2010)[116] |
Retrospective |
Variable |
92.3% (12/13) |
NR |
0% |
0% |
|
Wang (2010)[117] |
Retrospective |
Variable |
81.3% (13/16) |
NR |
12.5% (2/16); pancreatitis (2) |
0% |
|
Itoi (2011)[106] |
Retrospective |
Variable |
100% (15/15) |
NR |
0% |
0% |
|
Saleem (2010)[118] |
Retrospective |
Variable |
75% (42/56) |
NR |
0% |
0% |
|
Kianicka (2013)[119] |
Retrospective |
Variable |
100% (15/15) |
NR |
0% |
0% |
|
Azeem (2013)[120] |
Retrospective |
Variable |
91.4% (53/58) |
NR |
0% |
0% |
|
Tomizawa (2014)[121] |
Retrospective |
Variable |
68% (15/22) |
NR |
0% |
0% |
Notes: Endoscopy success rate refers to technical success (successful advancement to the papilla or biliary anastomosis). ERCP success rate refers to therapeutic success (successful cannulation and/or completion of intended intervention). Adverse events are stratified by severity according to the AGREE classification.
|
First author (year) |
Study type |
Anatomy |
Endoscopy success rate |
ERCP success rate |
Adverse events |
AGREE classification |
|---|---|---|---|---|---|---|
|
Spiral enteroscopy |
||||||
|
Wagh (2012)[122] |
Prospective |
Variable |
77% (10/13) |
NR |
0% |
0% |
|
Lennon (2012)[123] |
Retrospective |
RYGB |
28% (7/25) |
NR |
0% |
0% |
|
Shah (2013)[124] |
Retrospective |
RYGB |
62% (16/26) |
NR |
Overall 12% including DBE and SBE; perforation (2), abdominal pain (3), throat pain (4), pancreatitis (5), bleeding (1), death (1) |
0% |
|
Zouhairi (2015)[125] |
Retrospective |
RYGB |
64.3% (27/42) |
NR |
23.8% admissions, including 7.1% post-ERCP pancreatitis |
0% |
|
Ali (2018)[31] |
Retrospective |
RYGB ± others |
86% (27/31) |
NR |
0% |
0% |
|
Al-Toma (2022)[126] |
Prospective |
Variable (20% altered anatomy) |
70.3% (total enteroscopy) |
NR |
15.9% minor, 0% major |
0% |
|
Schneider (2023)[127] |
Retrospective |
RYGB + Bilroth II |
72.2% (26/36) |
NR |
2.8% major (delayed post-sphincterotomy bleeding) |
0% |
|
SAMISEN-B (2024)[128] |
Prospective |
RYGB + Billroth II |
54% (48/88) |
NR |
14% overall, 7% serious (1 MSE-related perforation) |
0% |
|
Nennstiel (2025)[129] |
Retrospective |
RYGB |
73.1% (19/26) |
NR |
11.5% overall (1 enteroscopy-related laceration, 1 post-ERCP pancreatitis, 1 anesthesia complication) |
0% |
Abbreviations: DBE, double-balloon enteroscopy; ERCP, endoscopic retrograde cholangiopancreatography; NR, not reported; SBE, single-balloon enteroscopy; SE, spiral enteroscopy.
Notes: Endoscopy success rate refers to technical success (successful advancement to the papilla or biliary anastomosis). ERCP success rate refers to therapeutic success (successful cannulation and/or completion of intended intervention). Adverse events are stratified by severity according to the AGREE classification.
Elevator Limitation in DAE Scopes
Several studies have highlighted that a major technical limitation of DAE systems, including SBE and DBE, is the absence of a distal elevator mechanism. Unlike conventional side-viewing duodenoscopes, DAE scopes do not provide elevator control at the instrument tip, which restricts the maneuverability and precise orientation of accessories within the papilla or bile duct. This limitation poses significant challenges during selective biliary cannulation, sphincterotomy, and stent deployment, particularly in patients with SAA.[23] [29] The lack of an elevator consequently contributes to the lower therapeutic success rates and longer procedural times observed in DAE-ERCP compared with standard duodenoscope-assisted ERCP.[30] [31]
Laparoscopy-Assisted ERCP
First described in 2002, LA-ERCP is a hybrid approach that employs minimally invasive surgery to allow passage of a standard duodenoscope through the stomach rather than transorally.[32] This procedure involves creating a gastrostomy through which a standard duodenoscope can be advanced to access the duodenum via the remnant stomach.[33]
Particularly effective in RYGB patients, it allows direct inspection of the abdominal cavity, facilitates the use of conventional ERCP tools, and avoids the delays associated with traditional gastrostomy-based approaches. When performed in experienced centers, it offers high success rates with same-day or next-day discharge in most cases.[27]
LA-ERCP has shown superior technical success in managing pancreaticobiliary diseases in RYGB patients, with rates exceeding 95%, compared with 60 to 70% with DAE techniques.[34] A recent meta-analysis demonstrated that both technical and clinical success rates were significantly higher with LA-ERCP compared with DAE-ERCP. Interestingly, it also reported a lower adverse event rate with LA-ERCP, contradicting earlier studies that had favored EA-ERCP for its safety profile.[35]
In contrast, the study by Gkolfakis et al reported a higher incidence of adverse events following interventional procedures overall, suggesting that the increased risk was more related to the access route (LA or EUS-guided) than to ERCP itself. LA-ERCP is associated with a greater risk of intra-abdominal infections, abscess formation, perforation, and hematomas.[36] The fact that it requires laparoscopy makes it more invasive than enteroscopy-assisted techniques. Supine positioning, limited access due to drapes, and poorly placed gastrostomies, especially near the pylorus, can hinder duodenoscope advancement. Optimal outcomes depend on precise surgical planning, with lateral gastrostomy placement along the greater curvature facilitating smoother scope passage.[27]
With these contradictions, there has been a growing shift toward less invasive, endoscopy-only approaches such as EUS-BD and EUS-directed transgastric ERCP (EDGE) as discussed later.
EUS-Guided Biliary Drainage
EUS-BD has been extensively reported since its first description by Giovannini et al in 2001.[37] In the last two decades, it has become one of the main alternatives for patients with unsuccessful ERCP from various reasons, or inaccessible papilla because of duodenal strictures, or surgically modified anatomy.[38] In a retrospective comparative study by Hakuta et al, EUS-BD demonstrated a higher technical success rate compared with DAE-ERCP, with no significant differences in clinical outcomes or adverse events. The findings suggest that EUS-BD may be a particularly effective option in patients with an intact papilla, where DAE-ERCP tends to have lower technical success.[39]
EUS-BD techniques create a new conduit from the biliary system to the gastrointestinal tract under EUS guidance, avoiding the need to reach the papilla. Broadly, EUS-BD can be achieved via three approaches: (1) EUS-guided rendezvous, (2) EUS-transmural drainage, and (3) EUS-guided antegrade interventions,[9] as summarized in [Fig. 3].

EUS-rendezvous (EUS-RV): This procedure involves EUS-guided bile duct puncture and advancement of a guidewire into the duct, which is then used to facilitate a second attempt at biliary cannulation, thus serving as a salvage technique in cases where standard deep cannulation has failed.[40] EUS-RV can be divided into an intrahepatic biliary duct (IHBD) approach and an extrahepatic biliary duct (EHBD) approach.[41] A recent meta-analysis comparing EUS-guided rendezvous (EUS-RV) and percutaneous transhepatic biliary (PTB)-RV showed comparable technical success rates (88.7% versus 94.1%) and overall adverse event rates (9.8% versus 13.4%), suggesting that EUS-RV is an effective salvage option after failed cannulation, but with careful technique.[42]
EUS-transmural drainage: This technique involves creating a direct fistulous tract between the biliary system and the gastrointestinal lumen to facilitate drainage via stent placement. The tract is typically established between the extrahepatic common bile duct and the duodenum (EUS-choledochoduodenostomy [EUS-CDS]) or between the left intrahepatic bile duct and the stomach (EUS-hepaticogastrostomy [EUS-HGS]). Recently, a connection between the biliary tree and the Roux limb (EUS-hepaticojejunostomy [EUS-HJS]) has gained popularity.[43] A recent multicenter study on EUS-HJS in post-gastrectomy patients showed 100% technical and 80% clinical success, with a 33% adverse event rate, comparable to EUS-HGS. While it offers advantages over percutaneous transhepatic biliary drainage (PTBD)—such as internal drainage and easier reintervention—it remains technically demanding and requires further evaluation in larger studies.[38]
EUS-guided antegrade intervention (EUS-AI): It is a minimally invasive alternative in which the echoendoscope is used to create a temporary fistula between the intestine and the bile duct, allowing antegrade traversal of a stricture or papilla to place a stent or dilate the obstruction from the proximal side.[44]
All the above procedures can be employed in patients with native gastrointestinal anatomy when ERCP fails or when anatomical challenges such as ampullary distortion, diverticula, or the presence of duodenal stents hinder conventional access.[43] In Type I anatomies, where the papilla is endoscopically reachable, EUS-RV, EUS-AI, and EUS-CDS can be considered as an alternative in cases of failed ERCP.[9] [41] EUS-RV may be feasible in some type II cases; however, when the papilla is inaccessible, alternative approaches such as EUS-guided antegrade stenting or transmural techniques like EUS-HGS or EUS-HJS are required.[9] [Table 4] summarizes the major published studies evaluating EUS-BD in patients with SAA.
|
First author (year) |
Study type |
No. of patients |
Anatomy |
Endoscopy success rate (technical and clinical) |
ERCP success rate |
Adverse events |
AGREE classification |
|---|---|---|---|---|---|---|---|
|
Weilert (2011)[130] |
Antegrade approach |
6 |
RY gastric bypass |
TS = 67%; CS = NA |
NR |
Liver hematoma—1 case |
Moderate |
|
Iwashita (2013)[131] |
Antegrade approach |
101 |
RY gastrojejunostomy, Whipple's |
TS = 100%; CS = NA |
NR |
Mild pancreatitis—2 |
Mild |
|
Itoi (2014)[132] |
Antegrade approach |
28 |
RY, gastric bypass, Billroth reconstruction |
TS = 60%; CS = NA |
NR |
Nil |
Nil |
|
Khashab (2016)[52] |
Antegrade approach |
49 |
RY reconstruction, RYGB, Whipple, B-II |
TS = 98%; CS = 88% |
NR |
20% |
Moderate |
|
Miranda-García (2016)[133] |
Antegrade approach |
7 |
Biliary enteric anastomosis (details N/A) |
TS = 57%; CA = 100% |
NR |
70% bleeding, stent migration |
Severe |
|
Iwashita (2016)[44] |
Antegrade approach |
29 |
GR with RY-19; GR with BII-3; GR with jejunal interposition-2; PD-4; BDR with HJ-1 |
79% |
NR |
17% bile peritonitis, cholecystitis, elevated CRP |
Moderate |
|
James (2018)[134] |
Antegrade approach |
29 |
RYGB, RY, B-II reconstruction, Whipple |
TS = 95%; CS = 95% |
NR |
15% abdominal pain, mild pancreatitis, mild cholangitis |
Mild |
|
Hosmer (2018)[135] |
Antegrade approach |
9 |
RYGB, RY |
TS = 100%; CS = NA |
NR |
11% cholangitis |
Mild |
|
Mukai (2019)[136] |
Antegrade approach |
48 |
RY, RYGB, Whipple, B-II |
TS = 91.9%; CS = 91.9% |
NR |
8.1% Biliary peritonitis |
Moderate |
|
Huang (2020)[137] |
Transmural drainage; EUV RV-8; EUS-HG = 14; EUS-CD = 11 |
60 |
Billroth I, Billroth II, RYGB, RYHJ Roux-en-Y choledochojejunostomy |
TS = 93.3%; CS = 84.9% |
NR |
9.09% hemorrhage, cholangitis |
Moderate |
|
Minaga (2020)[138] |
Transmural stenting—24; Antegrade stenting—2; combination of transmural and antegrade—14 |
40 |
Gastrectomy with RY, Billroth-II, pancreaticoduodenectomy, RYHJ |
TS = 100%; CSB = 95% |
NR |
15% bile leak, biliary peritonitis, pneumoperitoneum |
Moderate to severe |
Abbreviations: CS, clinical success ERCP, endoscopic retrograde cholangiopancreatography; EUS, endoscopic ultrasound; NR, not reported; TS, technical success.
Endoscopy success rate refers to technical success (successful advancement to the papilla or biliary anastomosis). ERCP success rate refers to therapeutic success (successful cannulation and/or completion of intended intervention). Adverse events are stratified by severity according to the AGREE classification.
Some studies were conducted to see the combined effectiveness of EUS-AI with a self-expandable metal stent (SEMS) and EUS-HGS (or EUS-HJS). In 2017, Ogura et al conducted a multicenter pilot study on EUS-HJS with antegrade stenting for malignant biliary obstruction, achieving an 85.7% technical success rate. Adverse events occurred in 10.2% of patients, mainly hyperamylasemia and one case of bleeding. Stent dysfunction in seven cases was managed with cleaning or replacement.[45] In 2019, Yang et al introduced EUS-directed transenteric ERCP (EDEE) using a lumen-apposing metal stent (LAMS) to access the biliary tree in altered, non-RYGB anatomy. In this study of 18 patients, fistulas were created in all, with 94% success and only two mild adverse events, which were medically managed.[46]
In the meta-analysis by Facciorusso et al, PTBD was found to be similar to EUS-HGS and EUS-CDS in terms of technical and clinical success, but a trend toward higher adverse event rates was noted with PTBD.[47] Similarly, another study conducted by Iwashita et al showed similar success rates between EUS-AI and PTBD, with PTBD showing greater adverse events.[48] A recent meta-analysis of eight studies comparing EUS-BD and ERCP/PTBD demonstrated that EUS BD outperformed ERCP-BD and PTBD in reducing stent dysfunction, postprocedural pancreatitis, and tumor ingrowth or overgrowth.[49] Importantly, EUS-BD provides internal drainage, an advantage over PTBD in terms of patient comfort and convenience (no external catheter). This has led both the European and American endoscopy societies to endorse EUS-BD as an alternative to PTBD after failed ERCP, in centers with appropriate expertise.[50]
Complications associated with EUS-BD include bile leakage into the peritoneum, peritonitis, pneumoperitoneum, bleeding, and stent misdeployment. A systematic review of EUS-BD documented bile leak in ∼2.2% and infection/cholangitis in ∼1% as the most common early AE.[51] Khashab et al compared EUS-guided biliary interventions with enteroscopy-assisted ERCP in 98 patients with SAA, finding higher clinical success (88 vs. 59.1%) and shorter procedure times with EUS, but a higher rate of adverse events (20 vs. 4%).[52]
In pooled data, overall EUS-BD adverse event rates around 15 to 20% are reported, though most are manageable with conservative measures or endoscopic/radiologic intervention. Recent innovations aim to reduce these risks, like dedicated EUS biliary stents with anti-migratory flaps and the increasing use of LAMS for a secure tract.[9] Despite these encouraging results, the procedure's technical complexity necessitates expert-level proficiency in EUS-guided interventions and careful patient selection through multidisciplinary assessment.[53]
Distinction between Motorized and Manual Spiral Enteroscopy Studies
SE techniques can be broadly divided into manual SE and motorized spiral enteroscopy (MSE), which differ significantly in design, efficiency, and clinical outcomes. Manual SE employs a manually rotated spiral overtube to advance the enteroscope by pleating the small bowel. Early studies using the manual spiral system reported technical success rates of 65 to 85%, therapeutic success of 60 to 75%, and adverse event rates of approximately 5 to 10% in Roux-en-Y anatomy.[54] [55] [56] However, manual SE was physically demanding, had a steep learning curve, and was limited by overtube instability.
In contrast, MSE represents a major technological advancement, incorporating a motor-driven spiral segment integrated into the endoscope that allows controlled rotation via a foot pedal. More recent studies of MSE, including a prospective single-center analysis, a systematic review and meta-analysis, and the multicenter SAMISEN-B registry, have demonstrated substantially improved performance, with technical success rates of 90 to 100%, therapeutic success of 80 to 95%, and a shorter learning curve of approximately 10 to 15 cases.[57] [58] [59] [60]
Adverse events remain comparable to manual SE (6–12%), primarily minor mucosal trauma or transient bleeding ([Table 5]).
|
Parameter |
Manual spiral enteroscopy |
Motorized spiral enteroscopy |
|---|---|---|
|
65–85% |
90–100% |
|
|
60–75% |
80–95% |
|
|
Steep; 25–30 cases for proficiency |
Shorter; 10–15 cases |
|
|
Procedure time[58] |
Longer; manual advancement |
20–30% shorter due to controlled motor drive |
|
5–10%; mucosal trauma, minor bleeding |
6–12%; mostly minor, rarely serious |
EDGE Procedure
EDGE, first described by Kedia et al in 2013, involved a two-stage approach using an EUS-guided gastrostomy followed by antegrade ERCP with a side-viewing duodenoscope to reach the papilla. This procedure involved the use of a PEG tube followed by a fully covered self-expanding metal stent (FCSEMS). While EDGE offers technical success rates >95%, comparable to ERCP in standard anatomy and superior to DAE-ERCP (60–70%), it is limited by its classical two-stage nature, making it less suitable in emergent scenarios like acute cholangitis.[61]
The advent of tissue anchoring techniques such as endoscopic suturing, however, has advanced the EDGE technique to a single-stage version. In 2014, Kedia et al advanced the EDGE technique by introducing a single-stage version (SS-EDGE) by using LAMS. This upgraded technique involves creating a gastro-gastric (G–G) or jejuno-gastric (J–G) fistula with the excluded stomach using an EUS-guided LAMS placement, followed by anchoring of the stent using dedicated clips made for stent anchoring, such as Stent-fix (Ovesco, Germany) or using endoscopic suturing (Boston Scientific, Massachusetts, United States).[62]
In a large multicenter study by Runge et al involving 178 patients (mean age: 58 years, 79% women), the EDGE procedure achieved a 98% technical success rate with an average procedure time of 92 minutes. Periprocedural adverse events occurred in 15.7% of patients, including 2.2% with severe events managed laparoscopically. Among those who underwent follow-up testing, persistent fistula was identified in 10%, with successful endoscopic closure achieved in all treated cases.[63]
In a recent meta-analysis of 16 studies (470 patients), EDGE demonstrated high technical (96%) and clinical (91%) success rates with a 17% adverse event rate, comparable to LA-ERCP but superior to E-ERCP in efficacy. EDGE also offered lower costs, shorter procedure times, and hospital stays.[64] Also, a 2018 multicenter study found EDGE had 100% success versus 60% for enteroscopy (p < 0.001), with shorter procedure time (50 vs. 91 minutes) and shorter median hospitalization (1 vs. 10.5 days).[65]
The primary concern based on the above studies has been stent dislodgment or leakage leading to peritonitis, and the potential for a persistent fistula that could enable to regain weight in bariatric patients. To counter this, some protocols use an initial slim endoscope or perform ERCP in a second session.[66] Anchoring techniques have also been employed: suturing the LAMS in place, or immediately exchanging the LAMS for a fully covered esophageal stent or a double-pigtail after ERCP to maintain the tract.[17] Another study by Hsueh et al attempted to use 20-mm LAMS to reduce stent migration.[67]
Risk of LAMS Migration with Immediate Balloon Dilation
Immediate balloon dilation of a newly deployed LAMS at the index EDGE session has been repeatedly implicated as a major risk factor for intraprocedural stent dislodgement and early migration. The proposed mechanism is mechanical dilation and passage of a duodenoscope through an immature fistulous tract can exert shear forces on the LAMS flanges before adequate tissue apposition and tract maturation have occurred, leading to flange separation or proximal displacement. Several clinical series and multicenter reports therefore reported higher rates of LAMS dislodgement with single-session (index) dilation/ERCP and consequently adopted alternative strategies (delayed ERCP or active fixation) to improve safety.[68] [69] [70] Contemporary guidelines and technical reviews now recommend avoiding routine balloon dilation and same-session duodenoscope passage when possible, instead delaying therapeutic ERCP for a short interval (commonly 7–14 days) to allow tract maturation; when same-session therapy is unavoidable, operators should consider larger-diameter LAMS, and use adjunctive anchoring/fixation techniques (endoscopic suturing, through-the-scope clips or double-pigtail stents) to mitigate migration risk.[71] [72] In short, real-world practice has shifted toward a “safety-first” approach—avoid immediate aggressive dilation at the index session when feasible, delay ERCP to allow tract healing, or employ reliable anchoring strategies if immediate therapy is clinically necessary.
Another key concern is the development of a persistent fistula, defined as a gastro-gastric or jejuno-gastric fistula that fails to close either by primary or secondary intention. Persistent fistulas are theoretically worrisome because they may functionally reverse the bypass and lead to weight regain, while also necessitating additional endoscopic interventions for closure.[73] This has raised an ongoing debate over whether the fistula should be actively closed at the time of ERCP (primary closure) or allowed to heal spontaneously (secondary intention). Comparative analyses have shown no clear advantage of primary closure over secondary intention. Ghandour et al found closure did not reduce fistula formation, which was instead predicted by longer stent dwell times.[74] [75] Similarly, Bertran-Rodriguez et al reported no difference in fistula or weight outcomes between closure and no closure.[67]
To minimize fistula-related issues, Wang et al suggested the GATE strategy (gastric access temporary for endoscopy). In GATE, after completing ERCP, the LAMS is promptly exchanged for a double-pigtail stent to maintain drainage but encourage fistula closure once removed. In this case series of 10 GATE patients, all had confirmed fistula closure, and no significant weight change occurred.[76]
In summary, EDGE has become an attractive first-line option for RYGB patients at centers with advanced endosonography expertise. It achieves near-surgical success rates with a single endoscopic team. The 2024 ASGE guideline explicitly recommends considering EDGE (also termed EUS-directed transgastric ERCP) over laparoscopic or enteroscopy-assisted methods in RYGB anatomy, given its high efficacy when performed in experienced centers.[50] The main caveats are ensuring appropriate patient selection (those who can tolerate a transmural fistula) and having robust protocols to manage the fistula (removal and closure) after the ERCP is done. With growing experience, EDGE has proven safe and effective, solidifying its role in the algorithm for bariatric anatomy and biliary access.
Procedures such as DAE-ERCP, advanced EUS-BD, and EDGE are technically demanding and exhibit a steep learning curve. Outcomes are significantly influenced by the experience of the operator and the expertise of the center. For instance, ERCP success rates are notably higher in centers with greater case volumes and experienced endoscopist.[77] Similarly, EUS-BD procedures demonstrate improved efficiency and reduced complication rates as the operator gains experience, with a learning plateau typically observed after ∼32 cases.[78] These factors underscore the importance of considering operator and institutional experience when evaluating reported success rates.
Percutaneous Transhepatic Biliary Drainage
Even with the advent of advanced endoscopic techniques, percutaneous and surgical interventions remain important in the SAA biliary drainage toolkit—particularly in urgent settings or when endoscopic methods are unavailable. PTBD has long been the fallback for failed ERCP. In this procedure, an interventional radiologist inserts a needle through the liver into an intrahepatic bile duct under fluoroscopy or combined imaging and fluoroscopic guidance, typically placing a catheter that drains bile to an external bag.[79]
A multicenter retrospective study of 630 patients (411 endoscopic, 219 PTBD) reported overall endoscopic success of 57% (highest in Billroth-II: 70.5%; lowest in Roux-en-Y: 49.5%). PTBD achieved a higher technical success rate of 91% but carried more complications (11.6 vs. 7.1%), with duodenoscopes in Billroth-II reconstructions showing a higher risk. Cumulative success after repeat endoscopic attempts was only 39%. While PTBD remains an effective salvage option, its higher morbidity, repeat intervention requirements, and impact on quality of life limit its role to a salvage option. In contrast, endoscopic techniques, despite lower success, are preferred due to lower morbidity, especially in well-selected patients.[3]
PTBD is often preferred in hemodynamically unstable patients, those unfit for general anesthesia, or when malignancy is suspected or EUS-BD is unavailable. Traditionally, the second-line option after failed ERCP, it offers high success rates but carries increased risks of bleeding, dislodgement, and peritonitis.[50] Even when compared with newer techniques, PTBD demonstrates less favorable outcomes. While Pleasant et al reported comparable success to LA-ERCP, PTBD was linked to higher complications and repeat interventions.[80] Another study showed EUS-BD to be more cost-effective compared with PTBD.[81]
For these reasons, ASGE 2024 guidelines advocated for EUS-BD over PTBD after a failed ERCP, provided appropriate expertise is available.[50] PTBD still has a crucial role in emergencies like severe cholangitis when endoscopic options are not immediately at hand.
Some studies have looked into the hybrid approaches for PTBD, such as the rendezvous technique, which involves both an interventional radiologist (IR) and an endoscopist. In this, IR advances a guidewire via PTBD into the duodenum, allowing the endoscopist to retrieve it and place a stent across the papilla or anastomosis. This improves technical success (80–90%) and significantly lowers complication rates compared with PTBD alone. Completing both steps in a single session also reduces catheter-related and septic complications and shortens hospital stay.[82]
Another hybrid approach is the PATENT technique (percutaneous-assisted transprosthetic endoscopic therapy), pioneered by Baron and Song.[83] In this, a percutaneous gastrostomy is created endoscopically or radiologically into the excluded stomach of an RYGB patient. Through this tract, a fully covered metal stent is placed, forming a stable path into the remnant stomach, and then a duodenoscope is inserted through the stent for ERCP. Early PATENT reports showed feasibility but also noted issues like stent migration and stoma infection. With the advent of LAMS, the EUS-guided version of PATENT (i.e., EDGE) has largely replaced it, being simpler and entirely endoscopic.[17]
Cost-effectiveness and Resource Considerations
While EDGE offers higher technical and clinical success rates compared with DAE–ERCP and PTBD, its widespread adoption is limited by the need for specialized EUS expertise, availability of LAMS, and endoscopy infrastructure. In low-resource settings, particularly in parts of Asia and other developing regions, PTBD remains a more feasible option due to lower equipment costs and broader procedural availability, despite its higher patient discomfort and risk of external drains.[84] Economic analyses suggest that EDGE may be cost-effective in high-volume tertiary centers with trained personnel, but the upfront investment and resource intensity restrict its applicability in many resource-limited hospitals.[85]
Hybrid, Novel, and Experimental Techniques
The field of therapeutic endoscopy is continuously evolving, and several novel technologies on the horizon may further improve biliary access in altered anatomy.
3D-guided technologies: To enhance EUS-BD and surgical accuracy, advanced imaging is being incorporated, such as using CT/MRI during the procedure to better identify the site for hepaticogastrostomy.[86] Zhang et al explored the feasibility of real-time continuous image-guided ERCP and concluded it to be an effective approach with reduced X-ray exposure and contrast agents.[87] Such technology may reduce the time and risk of LA-ERCP by mapping adhesions and target structures before making incisions.
Artificial intelligence (AI)-assisted navigation: AI is being explored to assist endoscopists in recognizing postsurgical anatomy and locating the correct limb or anastomosis. Kim et al developed an AI-assisted system using convolutional neural networks to help endoscopists identify the ampulla of Vater (AOV) and assess cannulation difficulty during ERCP. The AI model achieved high accuracy, with a 91.4% success rate in ampulla detection and performed comparably to expert endoscopists. It also showed promising results in predicting difficult cannulation cases, suggesting that AI could enhance procedural efficiency and safety in complex endoscopic settings.[88]
Biodegradable stents: A persistent issue in managing benign biliary strictures (such as biliary-enteric anastomotic strictures) is the need for multiple interventions to place and remove stents. Biodegradable biliary stents offer a promising solution. These stents, made of polymers like polydioxanone, maintain duct patency initially but then gradually dissolve, obviating the need for endoscopic removal. Early reports in patients with SAA have been encouraging. In a series of seven patients with benign biliary strictures and altered anatomy, biodegradable stents were deployed via DBE with 100% technical success; none required a second ERCP for stent removal.[89]
Magnetic compression anastomosis: It is a novel minimally invasive technique for restoring continuity across completely obstructed ducts or anastomoses, especially in benign biliary strictures refractory to standard approaches. The method involves placing two magnets on either side of the occlusion—typically via PTBD into the proximal bile duct and endoscopically into the bowel, which gradually forms a fistula through ischemic necrosis of the intervening tissue. Clinical success rates of up to 87.5% have been reported, with low recurrence and minimal complications, making it a promising option in complex cases.[90] [91]
In summary, the coming years are likely to bring multiple innovations that make biliary drainage in SAA safer, easier, and more universally available. Robotic enteroscopy and AI may help more endoscopists succeed in difficult anatomies. New anastomosis techniques like magnetic compression could offer nonsurgical cures for occluded passages. And improved stents—whether dissolving or medicated—will enhance long-term outcomes. These hybrid and experimental techniques continue the trend of multidisciplinary innovation in this challenging field. [Fig. 4] depicts our proposed algorithm for biliary drainage in SAA based on our review of the currently available techniques.
Long-Term Outcomes in EDGE and DAE-ERCP
Most published literature on EDGE and DAE–ERCP primarily emphasizes technical and short-term clinical success, such as immediate biliary cannulation or stent placement. However, long-term outcomes, including stent patency, recurrence of biliary strictures, and the need for repeat interventions, are critical for informing clinical decision-making and modality selection. In EDGE, LAMS generally maintain patency in the short term, but follow-up studies report variable rates of stent occlusion and recurrent strictures, particularly if the fistulous tract closes prematurely or tract maturation is incomplete.[92] DAE-ERCP, while effective in altered anatomy, may be limited by restricted accessory maneuverability and higher rates of incomplete drainage or stricture recurrence.[93] [94] In resource-limited settings, PTBD remains an alternative with durable patency, though it carries long-term risks such as infection, external drain complications, and patient discomfort.[84] Collectively, these data suggest that, beyond immediate procedural success, clinicians must consider long-term patency, stricture recurrence, and anticipated reinterventions when choosing between EDGE, DAE-ERCP, and PTBD, particularly in populations with SAA or limited access to specialized endoscopy services.
Conclusion
Biliary drainage in patients with SAA remains a complex challenge that is becoming increasingly relevant in the wake of rising bariatric and oncologic surgical procedures. Traditional ERCP demonstrates high success in Type I anatomies but faces significant limitations in Type II reconstructions due to altered intestinal continuity and anatomical complexity. Device-DAE-ERCP, while effective in some scenarios, remains technically demanding and time-consuming, with variable success rates. The emergence of EUS-BD, including rendezvous, transmural, and antegrade techniques, has offered a minimally invasive and effective alternative, with favorable outcomes compared with percutaneous approaches. In particular, the EDGE procedure has revolutionized management in RYGB patients by facilitating high-success ERCP access. While each approach has merits, tailoring intervention strategies based on the specific surgical anatomy, clinical urgency, and institutional expertise is essential. This review reports the definitions as used in each individual study, while emphasizing that differences in clinical success criteria should be considered when interpreting and comparing outcomes across studies. A multidisciplinary, anatomy-based algorithmic approach involving gastroenterologists, interventional radiologists, and surgeons—combined with growing access to EUS-specific tools—will help optimize outcomes in these complex patients. Continued innovation and prospective comparative studies are needed to standardize techniques and refine practice guidelines in this evolving field.
Conflict of Interest
None.
-
References
- 1 Tanisaka Y, Mizuide M, Fujita A. et al. Recent advances of interventional endoscopic retrograde cholangiopancreatography and endoscopic ultrasound for patients with surgically altered anatomy. J Clin Med 2021; 10 (08) 1624
- 2 Enochsson L, Swahn F, Arnelo U, Nilsson M, Löhr M, Persson G. Nationwide, population-based data from 11,074 ERCP procedures from the Swedish Registry for Gallstone Surgery and ERCP. Gastrointest Endosc 2010; 72 (06) 1175-1184 , 1184.e1–1184.e3
- 3 Nennstiel S, Freivogel K, Faber A. et al. Endoscopic and percutaneous biliary interventions in patients with altered upper gastrointestinal anatomy-the Munich Multicenter Experience. Surg Endosc 2021; 35 (12) 6853-6864
- 4 Rapp GA, Nelson KJ, Imagawa DK, Huang JY, Lee JG. Management of an accessory bile duct leak following pancreaticoduodenectomy: a novel approach utilizing a percutaneous and endoscopic rendezvous. ACG Case Rep J 2017; 4 (01) e2
- 5 Alalwan AA, Friedman J, Park H, Segal R, Brumback BA, Hartzema AG. US national trends in bariatric surgery: a decade of study. Surgery 2021; 170 (01) 13-17
- 6 Evans JA, Muthusamy VR, Acosta RD. et al; American Society for Gastrointestinal Endoscopy Standards of Practice Committee. The role of endoscopy in the bariatric surgery patient. Gastrointest Endosc 2015; 81 (05) 1063-1072
- 7 Krutsri C, Kida M, Yamauchi H, Iwai T, Imaizumi H, Koizumi W. Current status of endoscopic retrograde cholangiopancreatography in patients with surgically altered anatomy. World J Gastroenterol 2019; 25 (26) 3313-3333
- 8 Sundaram S, Kale A. Endoscopic ultrasound guided biliary drainage in surgically altered anatomy: a comprehensive review of various approaches. World J Gastrointest Endosc 2023; 15 (03) 122-132
- 9 Spadaccini M, Giacchetto CM, Fiacca M. et al. Endoscopic biliary drainage in surgically altered anatomy. Diagnostics (Basel) 2023; 13 (24) 3623
- 10 Lee KH, Yim GH, Han J, Jeong HT. Clinical outcomes of endoscopic retrograde cholangiopancreatography after Billroth II anastomosis: a comparison of gastroscope and duodenoscope. BMC Gastroenterol 2025; 25 (01) 373
- 11 Park TY, Song TJ. Recent advances in endoscopic retrograde cholangiopancreatography in Billroth II gastrectomy patients: a systematic review. World J Gastroenterol 2019; 25 (24) 3091-3107
- 12 Fugazza A, Anderloni A, Paduano D. et al. Underwater cap-assisted endoscopic retrograde cholangiopancreatography in patients with surgically altered anatomy: a pilot study. Endoscopy 2021; 53 (09) 927-931
- 13 Lee KJ, Park SW, Jang HJ. et al. Successful intubation using a cap-assisted colonoscope for endoscopic retrograde cholangiopancreatography in patients undergoing Roux-en-Y reconstruction. J Clin Med 2023; 12 (04) 1353
- 14 Ki HS, Park CH, Jun CH. et al. Feasibility of cap-assisted endoscopic retrograde cholangiopancreatography in patients with altered gastrointestinal anatomy. Gut Liver 2015; 9 (01) 109-112
- 15 Testoni PA, Mariani A, Aabakken L. et al. Papillary cannulation and sphincterotomy techniques at ERCP: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy 2016; 48 (07) 657-683
- 16 Park TY, Bang CS, Choi SH. et al. Forward-viewing endoscope for ERCP in patients with Billroth II gastrectomy: a systematic review and meta-analysis. Surg Endosc 2018; 32 (11) 4598-4613
- 17 Khara HS, Parvataneni S, Park S, Choi J, Kothari TH, Kothari ST. Review of ERCP techniques in Roux-en-Y gastric bypass patients: highlight on the novel EUS-directed transgastric ERCP (EGDE) technique. Curr Gastroenterol Rep 2021; 23 (07) 10
- 18 Gostout CJ, Bender CE. Cholangiopancreatography, sphincterotomy, and common duct stone removal via Roux-en-Y limb enteroscopy. Gastroenterology 1988; 95 (01) 156-163
- 19 Lichtenstein DR. Post-surgical anatomy and ERCP. Tech Gastrointest Endosc 2007; 9 (02) 114-124
- 20 Aabakken L, Bretthauer M, Line PD. Double-balloon enteroscopy for endoscopic retrograde cholangiography in patients with a Roux-en-Y anastomosis. Endoscopy 2007; 39 (12) 1068-1071
- 21 Cho E. Enteroscopy assisted ERCP. Int J Gastrointest Interv 2023; 12 (01) 79-80
- 22 Enestvedt BK, Kothari S, Pannala R. et al; ASGE Technology Committee. Devices and techniques for ERCP in the surgically altered GI tract. Gastrointest Endosc 2016; 83 (06) 1061-1075
- 23 Skinner M, Popa D, Neumann H, Wilcox CM, Mönkemüller K. ERCP with the overtube-assisted enteroscopy technique: a systematic review. Endoscopy 2014; 46 (07) 560-572
- 24 Yamauchi H, Kida M, Imaizumi H. et al. Innovations and techniques for balloon-enteroscope-assisted endoscopic retrograde cholangiopancreatography in patients with altered gastrointestinal anatomy. World J Gastroenterol 2015; 21 (21) 6460-6469
- 25 De Koning M, Moreels TG. Comparison of double-balloon and single-balloon enteroscope for therapeutic endoscopic retrograde cholangiography after Roux-en-Y small bowel surgery. BMC Gastroenterol 2016; 16 (01) 98
- 26 Garcés-Durán R, Monino L, Deprez PH, Piessevaux H, Moreels TG. Endoscopic treatment of biliopancreatic pathology in patients with Whipple's pancreaticoduodenectomy surgical variants: Lessons learned from single-balloon enteroscopy-assisted ERCP. Hepatobiliary Pancreat Dis Int 2024; 23 (05) 509-514
- 27 Samarasena JB, Nguyen NT, Lee JG. Endoscopic retrograde cholangiopancreatography in patients with Roux-en-Y anatomy. J Interv Gastroenterol 2012; 2 (02) 78-83
- 28 Katanuma A, Isayama H. Current status of endoscopic retrograde cholangiopancreatography in patients with surgically altered anatomy in Japan: questionnaire survey and important discussion points at Endoscopic Forum Japan 2013. Dig Endosc 2014; 26 (Suppl. 02) 109-115
- 29 Katanuma A, Maguchi H, Yane K. et al. ERCP using balloon-assisted enteroscopy in patients with surgically altered anatomy: Current status and future prospects. Dig Endosc 2015; 27 (S1): 63-72
- 30 Shah RJ, Smolkin M, Yen R. et al. A multicenter study of outcomes of device-assisted enteroscopy ERCP in patients with surgically altered anatomy. Gastrointest Endosc 2013; 77 (04) 593-600
- 31 Ali MF, Modayil R, Gurram KC, Brathwaite CEM, Friedel D, Stavropoulos SN. Spiral enteroscopy–assisted ERCP in bariatric-length Roux-en-Y anatomy: a large single-center series and review of the literature (with video). Gastrointest Endosc 2018; 87 (05) 1241-1247
- 32 Peters M, Papasavas PK, Caushaj PF, Kania RJ, Gagné DJ. Laparoscopic transgastric endoscopic retrograde cholangiopancreatography for benign common bile duct stricture after Roux-en-Y gastric bypass. Surg Endosc 2002; 16 (07) 1106-1106
- 33 Kim JH, Yang MJ. Recent advances of endoscopic retrograde cholangiopancreatography in surgically altered anatomy. Int J Gastrointest Interv 2021; 10 (03) 106-113
- 34 Banerjee N, Parepally M, Byrne TK, Pullatt RC, Coté GA, Elmunzer BJ. Systematic review of transgastric ERCP in Roux-en-Y gastric bypass patients. Surg Obes Relat Dis 2017; 13 (07) 1236-1242
- 35 Gellért B, Rancz A, Hoferica J. et al. Understanding the role of different ERCP techniques in post-Roux-en-Y gastric bypass patients: a systematic review and meta-analysis. Obes Surg 2025; 35 (01) 285-304
- 36 Gkolfakis P, Papaefthymiou A, Facciorusso A. et al. Comparison between enteroscopy-, laparoscopy- and endoscopic ultrasound-assisted endoscopic retrograde cholangio-pancreatography in patients with surgically altered anatomy: a systematic review and meta-analysis. Life (Basel) 2022; 12 (10) 1646
- 37 Giovannini M, Moutardier V, Pesenti C, Bories E, Lelong B, Delpero JR. Endoscopic ultrasound-guided bilioduodenal anastomosis: a new technique for biliary drainage. Endoscopy 2001; 33 (10) 898-900
- 38 Balducci D, Ratone JP, Schaefer M. et al. EUS-guided hepaticojejunostomy in patients with history of total gastrectomy: a multicenter retrospective feasibility study (with video). Gastrointest Endosc 2025; 101 (01) 117-122
- 39 Hakuta R, Ishida K, Nakai Y. et al. A retrospective comparative study of biliary drainage using balloon endoscopy and endoscopic ultrasound for malignant obstruction in patients with surgically altered anatomy. Surg Endosc 2024; 38 (12) 7269-7277
- 40 Iwashita T, Uemura S, Tezuka R. et al. Endoscopic ultrasound-guided rendezvous techniques for difficult biliary cannulation: technical review. Dig Endosc 2025; 37 (01) 68-76
- 41 Martin A, Kistler CA, Wrobel P, Yang JF, Siddiqui AA. Endoscopic ultrasound-guided pancreaticobiliary intervention in patients with surgically altered anatomy and inaccessible papillae: a review of current literature. Endosc Ultrasound 2016; 5 (03) 149-156
- 42 Yoon SB, Yang MJ, Shin DW. et al. Endoscopic ultrasound-rendezvous versus percutaneous-endoscopic rendezvous endoscopic retrograde cholangiopancreatography for bile duct access: systematic review and meta-analysis. Dig Endosc 2024; 36 (02) 129-140
- 43 Jovani M, Ichkhanian Y, Vosoughi K, Khashab MA. EUS-guided biliary drainage for postsurgical anatomy. Endosc Ultrasound 2019; 8 (7, Suppl 1): S57-S66
- 44 Iwashita T, Nakai Y, Hara K, Isayama H, Itoi T, Park DH. Endoscopic ultrasound-guided antegrade treatment of bile duct stone in patients with surgically altered anatomy: a multicenter retrospective cohort study. J Hepatobiliary Pancreat Sci 2016; 23 (04) 227-233
- 45 Ogura T, Kitano M, Takenaka M. et al. Multicenter prospective evaluation study of endoscopic ultrasound-guided hepaticogastrostomy combined with antegrade stenting (with video). Dig Endosc 2018; 30 (02) 252-259
- 46 Yang J, James T, Baron TH. et al. Tu1983 EUS-guided creation of entero-enterostomy using lumen apposing metal stents for pancreaticobiliary access in non-RYGB surgical anatomy patients. Gastrointest Endosc 2019; 89 (06) AB642-AB643
- 47 Facciorusso A, Mangiavillano B, Paduano D. et al. Methods for drainage of distal malignant biliary obstruction after ERCP failure: a systematic review and network meta-analysis. Cancers (Basel) 2022; 14 (13) 3291
- 48 Iwashita T, Uemura S, Mita N. et al. Endoscopic ultrasound guided-antegrade biliary stenting vs percutaneous transhepatic biliary stenting for unresectable distal malignant biliary obstruction in patients with surgically altered anatomy. J Hepatobiliary Pancreat Sci 2020; 27 (12) 968-976
- 49 Zafar Y, Azam H, Azhar MAB. et al. Efficacy of endoscopic ultrasound-guided biliary drainage of malignant biliary obstruction: a systematic review and meta-analysis of randomized controlled trials. Clin Endosc 2025; 58 (04) 533-543
- 50 Pawa S, Marya NB, Thiruvengadam NR. et al; ASGE Standards of Practice Committee, (ASGE Standards of Practice Committee Chair). American Society for Gastrointestinal Endoscopy guideline on the role of therapeutic EUS in the management of biliary tract disorders: summary and recommendations. Gastrointest Endosc 2024; 100 (06) 967-979
- 51 Giri S, Mohan BP, Jearth V. et al. Adverse events with EUS-guided biliary drainage: a systematic review and meta-analysis. Gastrointest Endosc 2023; 98 (04) 515-523.e18
- 52 Khashab MA, El Zein MH, Sharzehi K. et al. EUS-guided biliary drainage or enteroscopy-assisted ERCP in patients with surgical anatomy and biliary obstruction: an international comparative study. Endosc Int Open 2016; 4 (12) E1322-E1327
- 53 Makar M, Yodice M, Still M. et al. Management and outcomes of antithrombotic therapy in EUS-guided gallbladder drainage. Gastrointest Endosc 2025; 101 (01) 123-128
- 54 Ali MF, Modayil R, Gurram KC, Brathwaite CEM, Friedel D, Stavropoulos SN. Spiral enteroscopy-assisted ERCP in bariatric-length Roux-en-Y anatomy: a large single-center series and review of the literature (with video). Gastrointest Endosc 2018; 87 (05) 1241-1247
- 55 Desai SV, Naveed M, Jazwinski A, Jowell PS, Branch MS. Spiral enteroscopy versus laparoscopic-assisted endoscopy for completion of ERCP in patients with Roux-en-Y gastric bypass surgery. Gastrointest Endosc 2011; 73 (4 Suppl): AB122
- 56 Moreels TG. Altered anatomy: enteroscopy and ERCP procedure. Best Pract Res Clin Gastroenterol 2012; 26 (03) 347-357
- 57 Falt P, Urban O. Motorized spiral enteroscopy - a prospective analysis of 82 procedures at a single tertiary center. Scand J Gastroenterol 2023; 58 (10) 1207-1212
- 58 Beyna T. et al. Motorized spiral enteroscopy-assisted ERCP in patients with surgically altered anatomy. World J Gastrointest Endosc 2025
- 59 Papaefthymiou A, Ramai D, Maida M. et al. Performance and safety of motorized spiral enteroscopy: a systematic review and meta-analysis. Gastrointest Endosc 2023; 97 (05) 849-858.e5
- 60 Moreels TG, Aabakken L, Arvanitaki M, Knabe M, Beyna T. Enteroscopy-assisted ERCP in patients with surgically altered anatomy: Multicenter prospective registry (SAMISEN-B) using motorized spiral enteroscopy. Endosc Int Open 2024; 12 (11) 1392-1400
- 61 Kedia P, Kumta NA, Widmer J. et al. Endoscopic ultrasound-directed transgastric ERCP (EDGE) for Roux-en-Y anatomy: a novel technique. Endoscopy 2015; 47 (02) 159-163
- 62 Kedia P, Sharaiha RZ, Kumta NA, Kahaleh M. Internal EUS-directed transgastric ERCP (EDGE): game over. Gastroenterology 2014; 147 (03) 566-568
- 63 Runge TM, Chiang AL, Kowalski TE. et al. Endoscopic ultrasound-directed transgastric ERCP (EDGE): a retrospective multicenter study. Endoscopy 2021; 53 (06) 611-618
- 64 Deliwala SS, Mohan BP, Yarra P. et al. Efficacy & safety of EUS-directed transgastric endoscopic retrograde cholangiopancreatography (EDGE) in Roux-en-Y gastric bypass anatomy: a systematic review & meta-analysis. Surg Endosc 2023; 37 (06) 4144-4158
- 65 Bukhari M, Kowalski T, Nieto J. et al. An international, multicenter, comparative trial of EUS-guided gastrogastrostomy-assisted ERCP versus enteroscopy-assisted ERCP in patients with Roux-en-Y gastric bypass anatomy. Gastrointest Endosc 2018; 88 (03) 486-494
- 66 Ngamruengphong S, Nieto J, Kunda R. et al. Endoscopic ultrasound-guided creation of a transgastric fistula for the management of hepatobiliary disease in patients with Roux-en-Y gastric bypass. Endoscopy 2017; 49 (06) 549-552
- 67 Hsueh W, Krafft MR, Abdelqader A, Nasr J. Su1167 EUS-directed transgastric ERCP with 20 mm lumen-apposing metal stents in patients with Roux-en-Y gastric bypass, are we closer to perfection?. Gastrointest Endosc 2019; 89 (06) AB297
- 68 Krafft MR, Fang W, Nasr JY. Shortened-interval dual-session EDGE reduces the risk of LAMS dislodgement while facilitating timely ERCP. Dig Dis Sci 2021; 66 (08) 2776-2785
- 69 Kedia P, Tyberg A, Kumta NA. et al. EUS-directed transgastric ERCP for Roux-en-Y gastric bypass anatomy: a minimally invasive approach. Gastrointest Endosc 2015; 82 (03) 560-565
- 70 Tyberg A, Nieto J, Salgado S. et al. Endoscopic ultrasound (EUS)-directed transgastric endoscopic retrograde cholangiopancreatography or EUS: mid-term analysis of an emerging procedure. Clin Endosc 2017; 50 (02) 185-190
- 71 Fortunato C, Noronha Ferreira C, Moura M, Almeida A, Tato Marinho R, Correia L. Multimodal endoscopic management of fistula after sleeve gastrectomy involving a novel esophageal stent. GE Port J Gastroenterol 2024; 32 (03) 205-211
- 72 Honda H, Mosko JD, Kobayashi R. et al. Endoscopic ultrasound-directed transgastric endoscopic retrograde cholangiopancreatography for patients with Roux-en-Y gastric bypass anatomy: technical overview. Clin Endosc 2022; 55 (06) 736-741
- 73 Krafft MR, Lorenze A, Croglio MP, Fang W, Baron TH, Nasr JY. “Innocent as a LAMS”: Does spontaneous fistula closure (secondary intention), after EUS-directed transgastric ERCP (EDGE) via 20-mm lumen-apposing metal stent, confer an increased risk of persistent fistula and unintentional weight gain?. Dig Dis Sci 2022; 67 (06) 2337-2346
- 74 Ghandour B, Keane MG, Shinn B. et al; EDGE Study Group. Factors predictive of persistent fistulas in EUS-directed transgastric ERCP: a multicenter matched case-control study. Gastrointest Endosc 2023; 97 (02) 260-267
- 75 Bertran-Rodriguez C, Modi K, Shah S, Sawas T, Kedia P, Taunk P. S1626 efficacy of primary closure vs secondary closure to prevent persistent fistulas in patients that have undergone EUS-directed transgastric ERCP: a multicenter retrospective cohort study. Am J Gastroenterol 2024; 119 (10S): S1183-S1185
- 76 Wang TJ, Thompson CC, Ryou M. Gastric access temporary for endoscopy (GATE): a proposed algorithm for EUS-directed transgastric ERCP in gastric bypass patients. Surg Endosc 2019; 33 (06) 2024-2033
- 77 van der Wiel SE, Rauws E, Van Gool S. et al. Impact of ERCP simulator training on early ERCP learning curves of novice trainees: a cohort study. Endosc Int Open 2023; 11 (08) E690-E696
- 78 Tyberg A, Mishra A, Cheung M. et al. Learning curve for EUS-guided biliary drainage: What have we learned?. Endosc Ultrasound 2020; 9 (06) 392-396
- 79 Chandrashekhara SH, Gamanagatti S, Singh A, Bhatnagar S. Current status of percutaneous transhepatic biliary drainage in palliation of malignant obstructive jaundice: a review. Indian J Palliat Care 2016; 22 (04) 378-387
- 80 Pleasant T, Jiang D, Pawa S, Powell MS, Jahann DA, Pawa R. Outcomes of laparoscopic-assisted endoscopic retrograde cholangiopancreatography versus percutaneous transhepatic biliary drainage in patients with Roux-en-Y gastric bypass surgery. Gastrointest Endosc 2021; 93 (06) AB147
- 81 Gandhi D, Thiruvengadam N, Marya N, Pawa S, Saumoy M, Adler D. Cost-effectiveness of endoscopic ultrasound-guided biliary drainage versus percutaneous transhepatic biliary drainage in malignant biliary obstruction after failed endoscopic retrograde cholangiopancreatography. Gastrointest Endosc 2024; 99 (06) AB918
- 82 Chan TT, Chew M, Tang R. Troubleshooting difficult bile duct access: advanced ERCP cannulation techniques, percutaneous biliary drainage, or EUS-guided rendezvous technique?. Gastroenterol Insights 2021; 12 (04) 405-422
- 83 Baron TH, Song LM. Percutaneous assisted transprosthetic endoscopic therapy (PATENT): expanding gut access to infinity and beyond! (with video). Gastrointest Endosc 2012; 76 (03) 641-644
- 84 Chen GF, Yu WD, Wang JR, Qi FZ, Qiu YD. The methods of preoperative biliary drainage for resectable hilar cholangiocarcinoma patients: a protocol for systematic review and meta analysis. Medicine (Baltimore) 2020; 99 (21) e20237
- 85 James HJ, James TW, Wheeler SB, Spencer JC, Baron TH. Cost-effectiveness of endoscopic ultrasound-directed transgastric ERCP compared with device-assisted and laparoscopic-assisted ERCP in patients with Roux-en-Y anatomy. Endoscopy 2019; 51 (11) 1051-1058
- 86 Gruionu LG, Saftoiu A, Gruionu G. A novel fusion imaging system for endoscopic ultrasound. Endosc Ultrasound 2016; 5 (01) 35-42
- 87 Zhang DY, Yang S, Geng HX. et al. Real-time continuous image guidance for endoscopic retrograde cholangiopancreatography based on 3D/2D registration and respiratory compensation. World J Gastroenterol 2023; 29 (20) 3157-3167
- 88 Kim T, Kim J, Choi HS. et al. Artificial intelligence-assisted analysis of endoscopic retrograde cholangiopancreatography image for identifying ampulla and difficulty of selective cannulation. Sci Rep 2021; 11 (01) 8381
- 89 Kotha S, Berry P, Raja U, Wong T. Benign biliary strictures: utility of novel biodegradable biliary stents in surgically altered anatomy. Endoscopy 2021; 53 (08) E281-E282
- 90 Jang SI, Cho JH, Lee DK. Magnetic compression anastomosis for the treatment of post-transplant biliary stricture. Clin Endosc 2020; 53 (03) 266-275
- 91 Bekci T, Onder RO. Harnessing magnetic forces: discovery and development of biliary strictures treatment with compression anastomosis. Cerasus J Med 2024; 1 (03) 151-162
- 92 Hanscom M, Law R. Living on the EDGE: preparing for long-term success following EDGE procedure. Endosc Int Open 2023; 11 (05) E527-E528
- 93 Weng H, Fan QQ, Gu J. et al. Efficacy and long-term outcomes of single-balloon enteroscopy-assisted treatment for biliary obstruction after choledochojejunostomy. Surg Endosc 2024; 38 (11) 6282-6293
- 94 Li H, Khalaf K, Devloo R, Teshima C, May GR, Calo N. Long-term outcomes of double-balloon enteroscopy–endoscopic retrograde cholangiopancreatography for patients with hepaticojejunostomy anastomotic strictures: a retrospective cohort study. Gastrointest Endosc 2025; 101 (05) S412
- 95 Emmett DS, Mallat DB. Double-balloon ERCP in patients who have undergone Roux-en-Y surgery: a case series. Gastrointest Endosc 2007; 66 (05) 1038-1041
- 96 Maaser C, Lenze F, Bokemeyer M. et al. Double balloon enteroscopy: a useful tool for diagnostic and therapeutic procedures in the pancreaticobiliary system. Am J Gastroenterol 2008; 103 (04) 894-900
- 97 Mönkemüller K, Fry LC, Bellutti M, Neumann H, Malfertheiner P. ERCP with the double balloon enteroscope in patients with Roux-en-Y anastomosis. Surg Endosc 2009; 23 (09) 1961-1967
- 98 Moreels TG, Hubens GJ, Ysebaert DK, Op de Beeck B, Pelckmans PA. Diagnostic and therapeutic double-balloon enteroscopy after small bowel Roux-en-Y reconstructive surgery. Digestion 2009; 80 (03) 141-147
- 99 Parlak E, Disibeyaz S, Oztas E. et al. Endoscopic treatment of biliary disorders in patients with Roux-en-Y hepaticojejunostomy via a permanent access loop. Endoscopy 2011; 43 (01) 73-76
- 100 Raithel M, Dormann H, Naegel A. et al. Double-balloon-enteroscopy-based endoscopic retrograde cholangiopancreatography in post-surgical patients. World J Gastroenterol 2011; 17 (18) 2302-2314
- 101 Liu K, Joshi V, Saxena P, Kaffes AJ. Predictors of success for double balloon-assisted endoscopic retrograde cholangiopancreatography in patients with Roux-en-Y anastomosis. Dig Endosc 2017; 29 (02) 190-197
- 102 Kashani A, Abboud G, Lo SK, Jamil LH. Double balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography in Roux-en-Y gastric bypass anatomy: expert vs. novice experience. Endosc Int Open 2018; 6 (07) E885-E891
- 103 Shimatani M, Matsushita M, Takaoka M. et al. Effective “short” double-balloon enteroscope for diagnostic and therapeutic ERCP in patients with altered gastrointestinal anatomy: a large case series. Endoscopy 2009; 41 (10) 849-854
- 104 Tsujino T, Yamada A, Isayama H. et al. Experiences of biliary interventions using short double-balloon enteroscopy in patients with Roux-en-Y anastomosis or hepaticojejunostomy. Dig Endosc 2010; 22 (03) 211-216
- 105 Cho S, Kamalaporn P, Kandel G, Kortan P, Marcon N, May G. ‘Short’ double-balloon enteroscope endoscopic retrograde cholangiopancreatography in patients with a surgically altered upper gastrointestinal tract. Can J Gastroenterol 2011; 25 (11) 615-619
- 106 Itoi T, Ishii K, Sofuni A. et al. Long- and short-type double-balloon enteroscopy-assisted therapeutic ERCP for intact papilla in patients with a Roux-en-Y anastomosis. Surg Endosc 2011; 25 (03) 713-721
- 107 Osoegawa T, Motomura Y, Akahoshi K. et al. Improved techniques for double-balloon-enteroscopy-assisted endoscopic retrograde cholangiopancreatography. World J Gastroenterol 2012; 18 (46) 6843-6849
- 108 Park JH, Ye BD, Byeon JS. et al. Approaching pancreatic duct through pancreaticojejunostomy site with double ballon enteroscope in patients with Roux-en-Y anatomy. Hepatogastroenterology 2013; 60 (127) 1753-1758
- 109 Siddiqui AA, Chaaya A, Shelton C. et al. Utility of the short double-balloon enteroscope to perform pancreaticobiliary interventions in patients with surgically altered anatomy in a US multicenter study. Dig Dis Sci 2013; 58 (03) 858-864
- 110 Tsutsumi K, Kato H, Muro S. et al. ERCP using a short double-balloon enteroscope in patients with prior pancreatoduodenectomy: higher maneuverability supplied by the efferent-limb route. Surg Endosc 2015; 29 (07) 1944-1951
- 111 Cheng CL, Liu NJ, Tang JH. et al. Double-balloon enteroscopy for ERCP in patients with Billroth II anatomy: results of a large series of papillary large-balloon dilation for biliary stone removal. Endosc Int Open 2015; 3 (03) E216-E222
- 112 Shimatani M, Hatanaka H, Kogure H. et al; Japanese DB-ERC Study Group. Diagnostic and therapeutic endoscopic retrograde cholangiography using a short-type double-balloon endoscope in patients with altered gastrointestinal anatomy: a multicenter prospective study in Japan. Am J Gastroenterol 2016; 111 (12) 1750-1758
- 113 Uchida D, Tsutsumi K, Kato H. et al. Potential factors affecting results of short-type double-balloon endoscope-assisted endoscopic retrograde cholangiopancreatography. Dig Dis Sci 2020; 65 (05) 1460-1470
- 114 Ishihara Y, Matsumoto K, Kato H. et al. Treatment outcomes, including risk factors of stone recurrence, for hepatolithiasis using balloon-assisted endoscopy in patients with hepaticojejunostomy (with video). Surg Endosc 2021; 35 (04) 1895-1902
- 115 Neumann H, Fry LC, Meyer F, Malfertheiner P, Mönkemüller K. Endoscopic retrograde cholangiopancreatography using the single balloon enteroscope technique in patients with Roux-en-Y anastomosis. Digestion 2009; 80 (01) 52-57
- 116 Itoi T, Ishii K, Sofuni A. et al. Single-balloon enteroscopy-assisted ERCP in patients with Billroth II gastrectomy or Roux-en-Y anastomosis (with video). Am J Gastroenterol 2010; 105 (01) 93-99
- 117 Wang AY, Sauer BG, Behm BW. et al. Single-balloon enteroscopy effectively enables diagnostic and therapeutic retrograde cholangiography in patients with surgically altered anatomy. Gastrointest Endosc 2010; 71 (03) 641-649
- 118 Saleem A, Baron TH, Gostout CJ. et al. Endoscopic retrograde cholangiopancreatography using a single-balloon enteroscope in patients with altered Roux-en-Y anatomy. Endoscopy 2010; 42 (08) 656-660
- 119 Kianička B, Lata J, Novotný I, Dítě P, Vaníček J. Single balloon enteroscopy for endoscopic retrograde cholangiography in patients with Roux-en-Y hepaticojejuno anastomosis. World J Gastroenterol 2013; 19 (44) 8047-8055
- 120 Azeem N, Tabibian JH, Baron TH. et al. Use of a single-balloon enteroscope compared with variable-stiffness colonoscopes for endoscopic retrograde cholangiography in liver transplant patients with Roux-en-Y biliary anastomosis. Gastrointest Endosc 2013; 77 (04) 568-577
- 121 Tomizawa Y, Sullivan CT, Gelrud A. Single balloon enteroscopy (SBE) assisted therapeutic endoscopic retrograde cholangiopancreatography (ERCP) in patients with Roux-en-Y anastomosis. Dig Dis Sci 2014; 59 (02) 465-470
- 122 Wagh MS, Draganov PV. Prospective evaluation of spiral overtube-assisted ERCP in patients with surgically altered anatomy. Gastrointest Endosc 2012; 76 (02) 439-443
- 123 Lennon AM, Kapoor S, Khashab M. et al. Spiral assisted ERCP is equivalent to single balloon assisted ERCP in patients with Roux-en-Y anatomy. Dig Dis Sci 2012; 57 (05) 1391-1398
- 124 Shah RJ, Smolkin M, Yen R. et al. A multicenter, U.S. experience of single-balloon, double-balloon, and rotational overtube-assisted enteroscopy ERCP in patients with surgically altered pancreaticobiliary anatomy (with video). Gastrointest Endosc 2013; 77 (04) 593-600
- 125 Zouhairi ME, Watson JB, Desai SV. et al. Rotational assisted endoscopic retrograde cholangiopancreatography in patients with reconstructive gastrointestinal surgical anatomy. World J Gastrointest Endosc 2015; 7 (03) 278-282
- 126 Al-Toma A, Beaumont H, Koornstra JJ. et al. The performance and safety of motorized spiral enteroscopy, including in patients with surgically altered gastrointestinal anatomy: a multicenter prospective study. Endoscopy 2022; 54 (11) 1034-1042
- 127 Schneider M, Höllerich J, Gerges C, Balasus N, Neuhaus H, Beyna T. Motorized spiral enteroscopy-assisted ERCP in surgically altered anatomy: early experience from a retrospective cohort study. Endoscopy 2023; 55 (05) 476-481
- 128 Moreels TG, Aabakken L, Arvanitakis M, Knabe M, Beyna T. Correction: enteroscopy-assisted ERCP in patients with surgically altered anatomy: multicenter prospective registry (SAMISEN-B) using motorized spiral enteroscopy. Endosc Int Open 2024; 12 (11) C10-C10
- 129 Nennstiel S, Fried R, Herner A, Schlag C. Motorized spiral enteroscopy assisted endoscopic retrograde cholangiography in patients with Roux-en-Y-anatomy. World J Gastrointest Endosc 2025; 17 (08) 102787
- 130 Weilert F, Binmoeller KF, Marson F, Bhat Y, Shah JN. Endoscopic ultrasound-guided anterograde treatment of biliary stones following gastric bypass. Endoscopy 2011; 43 (12) 1105-1108
- 131 Iwashita T, Yasuda I, Doi S. et al. Endoscopic ultrasound-guided antegrade treatments for biliary disorders in patients with surgically altered anatomy. Dig Dis Sci 2013; 58 (08) 2417-2422
- 132 Itoi T, Sofuni A, Tsuchiya T, Ijima M, Iwashita T. Endoscopic ultrasonography-guided transhepatic antegrade stone removal in patients with surgically altered anatomy: case series and technical review (with videos). J Hepatobiliary Pancreat Sci 2014; 21 (12) E86-E93
- 133 Miranda-García P, Gonzalez JM, Tellechea JI, Culetto A, Barthet M. EUS hepaticogastrostomy for bilioenteric anastomotic strictures: a permanent access for repeated ambulatory dilations? Results from a pilot study. Endosc Int Open 2016; 4 (04) E461-E465
- 134 James TW, Fan YC, Baron TH. EUS-guided hepaticoenterostomy as a portal to allow definitive antegrade treatment of benign biliary diseases in patients with surgically altered anatomy. Gastrointest Endosc 2018; 88 (03) 547-554
- 135 Hosmer A, Abdelfatah MM, Law R, Baron TH. Endoscopic ultrasound-guided hepaticogastrostomy and antegrade clearance of biliary lithiasis in patients with surgically-altered anatomy. Endosc Int Open 2018; 6 (02) E127-E130
- 136 Mukai S, Itoi T, Sofuni A. et al. EUS-guided antegrade intervention for benign biliary diseases in patients with surgically altered anatomy (with videos). Gastrointest Endosc 2019; 89 (02) 399-407
- 137 Huang P, Zhang H, Zhang XF, Lv W, Fan Z. Application and value of endoscopic ultrasonography guided biliary interventional therapy in patients with biliary obstruction and surgically altered anatomy. Surg Laparosc Endosc Percutan Tech 2020; 30 (05) 454-458
- 138 Minaga K, Takenaka M, Ogura T. et al. Endoscopic ultrasound-guided biliary drainage for malignant biliary obstruction with surgically altered anatomy: a multicenter prospective registration study. Therap Adv Gastroenterol 2020; 13: 1756284820930964
Address for correspondence
Publication History
Article published online:
09 January 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Tanisaka Y, Mizuide M, Fujita A. et al. Recent advances of interventional endoscopic retrograde cholangiopancreatography and endoscopic ultrasound for patients with surgically altered anatomy. J Clin Med 2021; 10 (08) 1624
- 2 Enochsson L, Swahn F, Arnelo U, Nilsson M, Löhr M, Persson G. Nationwide, population-based data from 11,074 ERCP procedures from the Swedish Registry for Gallstone Surgery and ERCP. Gastrointest Endosc 2010; 72 (06) 1175-1184 , 1184.e1–1184.e3
- 3 Nennstiel S, Freivogel K, Faber A. et al. Endoscopic and percutaneous biliary interventions in patients with altered upper gastrointestinal anatomy-the Munich Multicenter Experience. Surg Endosc 2021; 35 (12) 6853-6864
- 4 Rapp GA, Nelson KJ, Imagawa DK, Huang JY, Lee JG. Management of an accessory bile duct leak following pancreaticoduodenectomy: a novel approach utilizing a percutaneous and endoscopic rendezvous. ACG Case Rep J 2017; 4 (01) e2
- 5 Alalwan AA, Friedman J, Park H, Segal R, Brumback BA, Hartzema AG. US national trends in bariatric surgery: a decade of study. Surgery 2021; 170 (01) 13-17
- 6 Evans JA, Muthusamy VR, Acosta RD. et al; American Society for Gastrointestinal Endoscopy Standards of Practice Committee. The role of endoscopy in the bariatric surgery patient. Gastrointest Endosc 2015; 81 (05) 1063-1072
- 7 Krutsri C, Kida M, Yamauchi H, Iwai T, Imaizumi H, Koizumi W. Current status of endoscopic retrograde cholangiopancreatography in patients with surgically altered anatomy. World J Gastroenterol 2019; 25 (26) 3313-3333
- 8 Sundaram S, Kale A. Endoscopic ultrasound guided biliary drainage in surgically altered anatomy: a comprehensive review of various approaches. World J Gastrointest Endosc 2023; 15 (03) 122-132
- 9 Spadaccini M, Giacchetto CM, Fiacca M. et al. Endoscopic biliary drainage in surgically altered anatomy. Diagnostics (Basel) 2023; 13 (24) 3623
- 10 Lee KH, Yim GH, Han J, Jeong HT. Clinical outcomes of endoscopic retrograde cholangiopancreatography after Billroth II anastomosis: a comparison of gastroscope and duodenoscope. BMC Gastroenterol 2025; 25 (01) 373
- 11 Park TY, Song TJ. Recent advances in endoscopic retrograde cholangiopancreatography in Billroth II gastrectomy patients: a systematic review. World J Gastroenterol 2019; 25 (24) 3091-3107
- 12 Fugazza A, Anderloni A, Paduano D. et al. Underwater cap-assisted endoscopic retrograde cholangiopancreatography in patients with surgically altered anatomy: a pilot study. Endoscopy 2021; 53 (09) 927-931
- 13 Lee KJ, Park SW, Jang HJ. et al. Successful intubation using a cap-assisted colonoscope for endoscopic retrograde cholangiopancreatography in patients undergoing Roux-en-Y reconstruction. J Clin Med 2023; 12 (04) 1353
- 14 Ki HS, Park CH, Jun CH. et al. Feasibility of cap-assisted endoscopic retrograde cholangiopancreatography in patients with altered gastrointestinal anatomy. Gut Liver 2015; 9 (01) 109-112
- 15 Testoni PA, Mariani A, Aabakken L. et al. Papillary cannulation and sphincterotomy techniques at ERCP: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy 2016; 48 (07) 657-683
- 16 Park TY, Bang CS, Choi SH. et al. Forward-viewing endoscope for ERCP in patients with Billroth II gastrectomy: a systematic review and meta-analysis. Surg Endosc 2018; 32 (11) 4598-4613
- 17 Khara HS, Parvataneni S, Park S, Choi J, Kothari TH, Kothari ST. Review of ERCP techniques in Roux-en-Y gastric bypass patients: highlight on the novel EUS-directed transgastric ERCP (EGDE) technique. Curr Gastroenterol Rep 2021; 23 (07) 10
- 18 Gostout CJ, Bender CE. Cholangiopancreatography, sphincterotomy, and common duct stone removal via Roux-en-Y limb enteroscopy. Gastroenterology 1988; 95 (01) 156-163
- 19 Lichtenstein DR. Post-surgical anatomy and ERCP. Tech Gastrointest Endosc 2007; 9 (02) 114-124
- 20 Aabakken L, Bretthauer M, Line PD. Double-balloon enteroscopy for endoscopic retrograde cholangiography in patients with a Roux-en-Y anastomosis. Endoscopy 2007; 39 (12) 1068-1071
- 21 Cho E. Enteroscopy assisted ERCP. Int J Gastrointest Interv 2023; 12 (01) 79-80
- 22 Enestvedt BK, Kothari S, Pannala R. et al; ASGE Technology Committee. Devices and techniques for ERCP in the surgically altered GI tract. Gastrointest Endosc 2016; 83 (06) 1061-1075
- 23 Skinner M, Popa D, Neumann H, Wilcox CM, Mönkemüller K. ERCP with the overtube-assisted enteroscopy technique: a systematic review. Endoscopy 2014; 46 (07) 560-572
- 24 Yamauchi H, Kida M, Imaizumi H. et al. Innovations and techniques for balloon-enteroscope-assisted endoscopic retrograde cholangiopancreatography in patients with altered gastrointestinal anatomy. World J Gastroenterol 2015; 21 (21) 6460-6469
- 25 De Koning M, Moreels TG. Comparison of double-balloon and single-balloon enteroscope for therapeutic endoscopic retrograde cholangiography after Roux-en-Y small bowel surgery. BMC Gastroenterol 2016; 16 (01) 98
- 26 Garcés-Durán R, Monino L, Deprez PH, Piessevaux H, Moreels TG. Endoscopic treatment of biliopancreatic pathology in patients with Whipple's pancreaticoduodenectomy surgical variants: Lessons learned from single-balloon enteroscopy-assisted ERCP. Hepatobiliary Pancreat Dis Int 2024; 23 (05) 509-514
- 27 Samarasena JB, Nguyen NT, Lee JG. Endoscopic retrograde cholangiopancreatography in patients with Roux-en-Y anatomy. J Interv Gastroenterol 2012; 2 (02) 78-83
- 28 Katanuma A, Isayama H. Current status of endoscopic retrograde cholangiopancreatography in patients with surgically altered anatomy in Japan: questionnaire survey and important discussion points at Endoscopic Forum Japan 2013. Dig Endosc 2014; 26 (Suppl. 02) 109-115
- 29 Katanuma A, Maguchi H, Yane K. et al. ERCP using balloon-assisted enteroscopy in patients with surgically altered anatomy: Current status and future prospects. Dig Endosc 2015; 27 (S1): 63-72
- 30 Shah RJ, Smolkin M, Yen R. et al. A multicenter study of outcomes of device-assisted enteroscopy ERCP in patients with surgically altered anatomy. Gastrointest Endosc 2013; 77 (04) 593-600
- 31 Ali MF, Modayil R, Gurram KC, Brathwaite CEM, Friedel D, Stavropoulos SN. Spiral enteroscopy–assisted ERCP in bariatric-length Roux-en-Y anatomy: a large single-center series and review of the literature (with video). Gastrointest Endosc 2018; 87 (05) 1241-1247
- 32 Peters M, Papasavas PK, Caushaj PF, Kania RJ, Gagné DJ. Laparoscopic transgastric endoscopic retrograde cholangiopancreatography for benign common bile duct stricture after Roux-en-Y gastric bypass. Surg Endosc 2002; 16 (07) 1106-1106
- 33 Kim JH, Yang MJ. Recent advances of endoscopic retrograde cholangiopancreatography in surgically altered anatomy. Int J Gastrointest Interv 2021; 10 (03) 106-113
- 34 Banerjee N, Parepally M, Byrne TK, Pullatt RC, Coté GA, Elmunzer BJ. Systematic review of transgastric ERCP in Roux-en-Y gastric bypass patients. Surg Obes Relat Dis 2017; 13 (07) 1236-1242
- 35 Gellért B, Rancz A, Hoferica J. et al. Understanding the role of different ERCP techniques in post-Roux-en-Y gastric bypass patients: a systematic review and meta-analysis. Obes Surg 2025; 35 (01) 285-304
- 36 Gkolfakis P, Papaefthymiou A, Facciorusso A. et al. Comparison between enteroscopy-, laparoscopy- and endoscopic ultrasound-assisted endoscopic retrograde cholangio-pancreatography in patients with surgically altered anatomy: a systematic review and meta-analysis. Life (Basel) 2022; 12 (10) 1646
- 37 Giovannini M, Moutardier V, Pesenti C, Bories E, Lelong B, Delpero JR. Endoscopic ultrasound-guided bilioduodenal anastomosis: a new technique for biliary drainage. Endoscopy 2001; 33 (10) 898-900
- 38 Balducci D, Ratone JP, Schaefer M. et al. EUS-guided hepaticojejunostomy in patients with history of total gastrectomy: a multicenter retrospective feasibility study (with video). Gastrointest Endosc 2025; 101 (01) 117-122
- 39 Hakuta R, Ishida K, Nakai Y. et al. A retrospective comparative study of biliary drainage using balloon endoscopy and endoscopic ultrasound for malignant obstruction in patients with surgically altered anatomy. Surg Endosc 2024; 38 (12) 7269-7277
- 40 Iwashita T, Uemura S, Tezuka R. et al. Endoscopic ultrasound-guided rendezvous techniques for difficult biliary cannulation: technical review. Dig Endosc 2025; 37 (01) 68-76
- 41 Martin A, Kistler CA, Wrobel P, Yang JF, Siddiqui AA. Endoscopic ultrasound-guided pancreaticobiliary intervention in patients with surgically altered anatomy and inaccessible papillae: a review of current literature. Endosc Ultrasound 2016; 5 (03) 149-156
- 42 Yoon SB, Yang MJ, Shin DW. et al. Endoscopic ultrasound-rendezvous versus percutaneous-endoscopic rendezvous endoscopic retrograde cholangiopancreatography for bile duct access: systematic review and meta-analysis. Dig Endosc 2024; 36 (02) 129-140
- 43 Jovani M, Ichkhanian Y, Vosoughi K, Khashab MA. EUS-guided biliary drainage for postsurgical anatomy. Endosc Ultrasound 2019; 8 (7, Suppl 1): S57-S66
- 44 Iwashita T, Nakai Y, Hara K, Isayama H, Itoi T, Park DH. Endoscopic ultrasound-guided antegrade treatment of bile duct stone in patients with surgically altered anatomy: a multicenter retrospective cohort study. J Hepatobiliary Pancreat Sci 2016; 23 (04) 227-233
- 45 Ogura T, Kitano M, Takenaka M. et al. Multicenter prospective evaluation study of endoscopic ultrasound-guided hepaticogastrostomy combined with antegrade stenting (with video). Dig Endosc 2018; 30 (02) 252-259
- 46 Yang J, James T, Baron TH. et al. Tu1983 EUS-guided creation of entero-enterostomy using lumen apposing metal stents for pancreaticobiliary access in non-RYGB surgical anatomy patients. Gastrointest Endosc 2019; 89 (06) AB642-AB643
- 47 Facciorusso A, Mangiavillano B, Paduano D. et al. Methods for drainage of distal malignant biliary obstruction after ERCP failure: a systematic review and network meta-analysis. Cancers (Basel) 2022; 14 (13) 3291
- 48 Iwashita T, Uemura S, Mita N. et al. Endoscopic ultrasound guided-antegrade biliary stenting vs percutaneous transhepatic biliary stenting for unresectable distal malignant biliary obstruction in patients with surgically altered anatomy. J Hepatobiliary Pancreat Sci 2020; 27 (12) 968-976
- 49 Zafar Y, Azam H, Azhar MAB. et al. Efficacy of endoscopic ultrasound-guided biliary drainage of malignant biliary obstruction: a systematic review and meta-analysis of randomized controlled trials. Clin Endosc 2025; 58 (04) 533-543
- 50 Pawa S, Marya NB, Thiruvengadam NR. et al; ASGE Standards of Practice Committee, (ASGE Standards of Practice Committee Chair). American Society for Gastrointestinal Endoscopy guideline on the role of therapeutic EUS in the management of biliary tract disorders: summary and recommendations. Gastrointest Endosc 2024; 100 (06) 967-979
- 51 Giri S, Mohan BP, Jearth V. et al. Adverse events with EUS-guided biliary drainage: a systematic review and meta-analysis. Gastrointest Endosc 2023; 98 (04) 515-523.e18
- 52 Khashab MA, El Zein MH, Sharzehi K. et al. EUS-guided biliary drainage or enteroscopy-assisted ERCP in patients with surgical anatomy and biliary obstruction: an international comparative study. Endosc Int Open 2016; 4 (12) E1322-E1327
- 53 Makar M, Yodice M, Still M. et al. Management and outcomes of antithrombotic therapy in EUS-guided gallbladder drainage. Gastrointest Endosc 2025; 101 (01) 123-128
- 54 Ali MF, Modayil R, Gurram KC, Brathwaite CEM, Friedel D, Stavropoulos SN. Spiral enteroscopy-assisted ERCP in bariatric-length Roux-en-Y anatomy: a large single-center series and review of the literature (with video). Gastrointest Endosc 2018; 87 (05) 1241-1247
- 55 Desai SV, Naveed M, Jazwinski A, Jowell PS, Branch MS. Spiral enteroscopy versus laparoscopic-assisted endoscopy for completion of ERCP in patients with Roux-en-Y gastric bypass surgery. Gastrointest Endosc 2011; 73 (4 Suppl): AB122
- 56 Moreels TG. Altered anatomy: enteroscopy and ERCP procedure. Best Pract Res Clin Gastroenterol 2012; 26 (03) 347-357
- 57 Falt P, Urban O. Motorized spiral enteroscopy - a prospective analysis of 82 procedures at a single tertiary center. Scand J Gastroenterol 2023; 58 (10) 1207-1212
- 58 Beyna T. et al. Motorized spiral enteroscopy-assisted ERCP in patients with surgically altered anatomy. World J Gastrointest Endosc 2025
- 59 Papaefthymiou A, Ramai D, Maida M. et al. Performance and safety of motorized spiral enteroscopy: a systematic review and meta-analysis. Gastrointest Endosc 2023; 97 (05) 849-858.e5
- 60 Moreels TG, Aabakken L, Arvanitaki M, Knabe M, Beyna T. Enteroscopy-assisted ERCP in patients with surgically altered anatomy: Multicenter prospective registry (SAMISEN-B) using motorized spiral enteroscopy. Endosc Int Open 2024; 12 (11) 1392-1400
- 61 Kedia P, Kumta NA, Widmer J. et al. Endoscopic ultrasound-directed transgastric ERCP (EDGE) for Roux-en-Y anatomy: a novel technique. Endoscopy 2015; 47 (02) 159-163
- 62 Kedia P, Sharaiha RZ, Kumta NA, Kahaleh M. Internal EUS-directed transgastric ERCP (EDGE): game over. Gastroenterology 2014; 147 (03) 566-568
- 63 Runge TM, Chiang AL, Kowalski TE. et al. Endoscopic ultrasound-directed transgastric ERCP (EDGE): a retrospective multicenter study. Endoscopy 2021; 53 (06) 611-618
- 64 Deliwala SS, Mohan BP, Yarra P. et al. Efficacy & safety of EUS-directed transgastric endoscopic retrograde cholangiopancreatography (EDGE) in Roux-en-Y gastric bypass anatomy: a systematic review & meta-analysis. Surg Endosc 2023; 37 (06) 4144-4158
- 65 Bukhari M, Kowalski T, Nieto J. et al. An international, multicenter, comparative trial of EUS-guided gastrogastrostomy-assisted ERCP versus enteroscopy-assisted ERCP in patients with Roux-en-Y gastric bypass anatomy. Gastrointest Endosc 2018; 88 (03) 486-494
- 66 Ngamruengphong S, Nieto J, Kunda R. et al. Endoscopic ultrasound-guided creation of a transgastric fistula for the management of hepatobiliary disease in patients with Roux-en-Y gastric bypass. Endoscopy 2017; 49 (06) 549-552
- 67 Hsueh W, Krafft MR, Abdelqader A, Nasr J. Su1167 EUS-directed transgastric ERCP with 20 mm lumen-apposing metal stents in patients with Roux-en-Y gastric bypass, are we closer to perfection?. Gastrointest Endosc 2019; 89 (06) AB297
- 68 Krafft MR, Fang W, Nasr JY. Shortened-interval dual-session EDGE reduces the risk of LAMS dislodgement while facilitating timely ERCP. Dig Dis Sci 2021; 66 (08) 2776-2785
- 69 Kedia P, Tyberg A, Kumta NA. et al. EUS-directed transgastric ERCP for Roux-en-Y gastric bypass anatomy: a minimally invasive approach. Gastrointest Endosc 2015; 82 (03) 560-565
- 70 Tyberg A, Nieto J, Salgado S. et al. Endoscopic ultrasound (EUS)-directed transgastric endoscopic retrograde cholangiopancreatography or EUS: mid-term analysis of an emerging procedure. Clin Endosc 2017; 50 (02) 185-190
- 71 Fortunato C, Noronha Ferreira C, Moura M, Almeida A, Tato Marinho R, Correia L. Multimodal endoscopic management of fistula after sleeve gastrectomy involving a novel esophageal stent. GE Port J Gastroenterol 2024; 32 (03) 205-211
- 72 Honda H, Mosko JD, Kobayashi R. et al. Endoscopic ultrasound-directed transgastric endoscopic retrograde cholangiopancreatography for patients with Roux-en-Y gastric bypass anatomy: technical overview. Clin Endosc 2022; 55 (06) 736-741
- 73 Krafft MR, Lorenze A, Croglio MP, Fang W, Baron TH, Nasr JY. “Innocent as a LAMS”: Does spontaneous fistula closure (secondary intention), after EUS-directed transgastric ERCP (EDGE) via 20-mm lumen-apposing metal stent, confer an increased risk of persistent fistula and unintentional weight gain?. Dig Dis Sci 2022; 67 (06) 2337-2346
- 74 Ghandour B, Keane MG, Shinn B. et al; EDGE Study Group. Factors predictive of persistent fistulas in EUS-directed transgastric ERCP: a multicenter matched case-control study. Gastrointest Endosc 2023; 97 (02) 260-267
- 75 Bertran-Rodriguez C, Modi K, Shah S, Sawas T, Kedia P, Taunk P. S1626 efficacy of primary closure vs secondary closure to prevent persistent fistulas in patients that have undergone EUS-directed transgastric ERCP: a multicenter retrospective cohort study. Am J Gastroenterol 2024; 119 (10S): S1183-S1185
- 76 Wang TJ, Thompson CC, Ryou M. Gastric access temporary for endoscopy (GATE): a proposed algorithm for EUS-directed transgastric ERCP in gastric bypass patients. Surg Endosc 2019; 33 (06) 2024-2033
- 77 van der Wiel SE, Rauws E, Van Gool S. et al. Impact of ERCP simulator training on early ERCP learning curves of novice trainees: a cohort study. Endosc Int Open 2023; 11 (08) E690-E696
- 78 Tyberg A, Mishra A, Cheung M. et al. Learning curve for EUS-guided biliary drainage: What have we learned?. Endosc Ultrasound 2020; 9 (06) 392-396
- 79 Chandrashekhara SH, Gamanagatti S, Singh A, Bhatnagar S. Current status of percutaneous transhepatic biliary drainage in palliation of malignant obstructive jaundice: a review. Indian J Palliat Care 2016; 22 (04) 378-387
- 80 Pleasant T, Jiang D, Pawa S, Powell MS, Jahann DA, Pawa R. Outcomes of laparoscopic-assisted endoscopic retrograde cholangiopancreatography versus percutaneous transhepatic biliary drainage in patients with Roux-en-Y gastric bypass surgery. Gastrointest Endosc 2021; 93 (06) AB147
- 81 Gandhi D, Thiruvengadam N, Marya N, Pawa S, Saumoy M, Adler D. Cost-effectiveness of endoscopic ultrasound-guided biliary drainage versus percutaneous transhepatic biliary drainage in malignant biliary obstruction after failed endoscopic retrograde cholangiopancreatography. Gastrointest Endosc 2024; 99 (06) AB918
- 82 Chan TT, Chew M, Tang R. Troubleshooting difficult bile duct access: advanced ERCP cannulation techniques, percutaneous biliary drainage, or EUS-guided rendezvous technique?. Gastroenterol Insights 2021; 12 (04) 405-422
- 83 Baron TH, Song LM. Percutaneous assisted transprosthetic endoscopic therapy (PATENT): expanding gut access to infinity and beyond! (with video). Gastrointest Endosc 2012; 76 (03) 641-644
- 84 Chen GF, Yu WD, Wang JR, Qi FZ, Qiu YD. The methods of preoperative biliary drainage for resectable hilar cholangiocarcinoma patients: a protocol for systematic review and meta analysis. Medicine (Baltimore) 2020; 99 (21) e20237
- 85 James HJ, James TW, Wheeler SB, Spencer JC, Baron TH. Cost-effectiveness of endoscopic ultrasound-directed transgastric ERCP compared with device-assisted and laparoscopic-assisted ERCP in patients with Roux-en-Y anatomy. Endoscopy 2019; 51 (11) 1051-1058
- 86 Gruionu LG, Saftoiu A, Gruionu G. A novel fusion imaging system for endoscopic ultrasound. Endosc Ultrasound 2016; 5 (01) 35-42
- 87 Zhang DY, Yang S, Geng HX. et al. Real-time continuous image guidance for endoscopic retrograde cholangiopancreatography based on 3D/2D registration and respiratory compensation. World J Gastroenterol 2023; 29 (20) 3157-3167
- 88 Kim T, Kim J, Choi HS. et al. Artificial intelligence-assisted analysis of endoscopic retrograde cholangiopancreatography image for identifying ampulla and difficulty of selective cannulation. Sci Rep 2021; 11 (01) 8381
- 89 Kotha S, Berry P, Raja U, Wong T. Benign biliary strictures: utility of novel biodegradable biliary stents in surgically altered anatomy. Endoscopy 2021; 53 (08) E281-E282
- 90 Jang SI, Cho JH, Lee DK. Magnetic compression anastomosis for the treatment of post-transplant biliary stricture. Clin Endosc 2020; 53 (03) 266-275
- 91 Bekci T, Onder RO. Harnessing magnetic forces: discovery and development of biliary strictures treatment with compression anastomosis. Cerasus J Med 2024; 1 (03) 151-162
- 92 Hanscom M, Law R. Living on the EDGE: preparing for long-term success following EDGE procedure. Endosc Int Open 2023; 11 (05) E527-E528
- 93 Weng H, Fan QQ, Gu J. et al. Efficacy and long-term outcomes of single-balloon enteroscopy-assisted treatment for biliary obstruction after choledochojejunostomy. Surg Endosc 2024; 38 (11) 6282-6293
- 94 Li H, Khalaf K, Devloo R, Teshima C, May GR, Calo N. Long-term outcomes of double-balloon enteroscopy–endoscopic retrograde cholangiopancreatography for patients with hepaticojejunostomy anastomotic strictures: a retrospective cohort study. Gastrointest Endosc 2025; 101 (05) S412
- 95 Emmett DS, Mallat DB. Double-balloon ERCP in patients who have undergone Roux-en-Y surgery: a case series. Gastrointest Endosc 2007; 66 (05) 1038-1041
- 96 Maaser C, Lenze F, Bokemeyer M. et al. Double balloon enteroscopy: a useful tool for diagnostic and therapeutic procedures in the pancreaticobiliary system. Am J Gastroenterol 2008; 103 (04) 894-900
- 97 Mönkemüller K, Fry LC, Bellutti M, Neumann H, Malfertheiner P. ERCP with the double balloon enteroscope in patients with Roux-en-Y anastomosis. Surg Endosc 2009; 23 (09) 1961-1967
- 98 Moreels TG, Hubens GJ, Ysebaert DK, Op de Beeck B, Pelckmans PA. Diagnostic and therapeutic double-balloon enteroscopy after small bowel Roux-en-Y reconstructive surgery. Digestion 2009; 80 (03) 141-147
- 99 Parlak E, Disibeyaz S, Oztas E. et al. Endoscopic treatment of biliary disorders in patients with Roux-en-Y hepaticojejunostomy via a permanent access loop. Endoscopy 2011; 43 (01) 73-76
- 100 Raithel M, Dormann H, Naegel A. et al. Double-balloon-enteroscopy-based endoscopic retrograde cholangiopancreatography in post-surgical patients. World J Gastroenterol 2011; 17 (18) 2302-2314
- 101 Liu K, Joshi V, Saxena P, Kaffes AJ. Predictors of success for double balloon-assisted endoscopic retrograde cholangiopancreatography in patients with Roux-en-Y anastomosis. Dig Endosc 2017; 29 (02) 190-197
- 102 Kashani A, Abboud G, Lo SK, Jamil LH. Double balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography in Roux-en-Y gastric bypass anatomy: expert vs. novice experience. Endosc Int Open 2018; 6 (07) E885-E891
- 103 Shimatani M, Matsushita M, Takaoka M. et al. Effective “short” double-balloon enteroscope for diagnostic and therapeutic ERCP in patients with altered gastrointestinal anatomy: a large case series. Endoscopy 2009; 41 (10) 849-854
- 104 Tsujino T, Yamada A, Isayama H. et al. Experiences of biliary interventions using short double-balloon enteroscopy in patients with Roux-en-Y anastomosis or hepaticojejunostomy. Dig Endosc 2010; 22 (03) 211-216
- 105 Cho S, Kamalaporn P, Kandel G, Kortan P, Marcon N, May G. ‘Short’ double-balloon enteroscope endoscopic retrograde cholangiopancreatography in patients with a surgically altered upper gastrointestinal tract. Can J Gastroenterol 2011; 25 (11) 615-619
- 106 Itoi T, Ishii K, Sofuni A. et al. Long- and short-type double-balloon enteroscopy-assisted therapeutic ERCP for intact papilla in patients with a Roux-en-Y anastomosis. Surg Endosc 2011; 25 (03) 713-721
- 107 Osoegawa T, Motomura Y, Akahoshi K. et al. Improved techniques for double-balloon-enteroscopy-assisted endoscopic retrograde cholangiopancreatography. World J Gastroenterol 2012; 18 (46) 6843-6849
- 108 Park JH, Ye BD, Byeon JS. et al. Approaching pancreatic duct through pancreaticojejunostomy site with double ballon enteroscope in patients with Roux-en-Y anatomy. Hepatogastroenterology 2013; 60 (127) 1753-1758
- 109 Siddiqui AA, Chaaya A, Shelton C. et al. Utility of the short double-balloon enteroscope to perform pancreaticobiliary interventions in patients with surgically altered anatomy in a US multicenter study. Dig Dis Sci 2013; 58 (03) 858-864
- 110 Tsutsumi K, Kato H, Muro S. et al. ERCP using a short double-balloon enteroscope in patients with prior pancreatoduodenectomy: higher maneuverability supplied by the efferent-limb route. Surg Endosc 2015; 29 (07) 1944-1951
- 111 Cheng CL, Liu NJ, Tang JH. et al. Double-balloon enteroscopy for ERCP in patients with Billroth II anatomy: results of a large series of papillary large-balloon dilation for biliary stone removal. Endosc Int Open 2015; 3 (03) E216-E222
- 112 Shimatani M, Hatanaka H, Kogure H. et al; Japanese DB-ERC Study Group. Diagnostic and therapeutic endoscopic retrograde cholangiography using a short-type double-balloon endoscope in patients with altered gastrointestinal anatomy: a multicenter prospective study in Japan. Am J Gastroenterol 2016; 111 (12) 1750-1758
- 113 Uchida D, Tsutsumi K, Kato H. et al. Potential factors affecting results of short-type double-balloon endoscope-assisted endoscopic retrograde cholangiopancreatography. Dig Dis Sci 2020; 65 (05) 1460-1470
- 114 Ishihara Y, Matsumoto K, Kato H. et al. Treatment outcomes, including risk factors of stone recurrence, for hepatolithiasis using balloon-assisted endoscopy in patients with hepaticojejunostomy (with video). Surg Endosc 2021; 35 (04) 1895-1902
- 115 Neumann H, Fry LC, Meyer F, Malfertheiner P, Mönkemüller K. Endoscopic retrograde cholangiopancreatography using the single balloon enteroscope technique in patients with Roux-en-Y anastomosis. Digestion 2009; 80 (01) 52-57
- 116 Itoi T, Ishii K, Sofuni A. et al. Single-balloon enteroscopy-assisted ERCP in patients with Billroth II gastrectomy or Roux-en-Y anastomosis (with video). Am J Gastroenterol 2010; 105 (01) 93-99
- 117 Wang AY, Sauer BG, Behm BW. et al. Single-balloon enteroscopy effectively enables diagnostic and therapeutic retrograde cholangiography in patients with surgically altered anatomy. Gastrointest Endosc 2010; 71 (03) 641-649
- 118 Saleem A, Baron TH, Gostout CJ. et al. Endoscopic retrograde cholangiopancreatography using a single-balloon enteroscope in patients with altered Roux-en-Y anatomy. Endoscopy 2010; 42 (08) 656-660
- 119 Kianička B, Lata J, Novotný I, Dítě P, Vaníček J. Single balloon enteroscopy for endoscopic retrograde cholangiography in patients with Roux-en-Y hepaticojejuno anastomosis. World J Gastroenterol 2013; 19 (44) 8047-8055
- 120 Azeem N, Tabibian JH, Baron TH. et al. Use of a single-balloon enteroscope compared with variable-stiffness colonoscopes for endoscopic retrograde cholangiography in liver transplant patients with Roux-en-Y biliary anastomosis. Gastrointest Endosc 2013; 77 (04) 568-577
- 121 Tomizawa Y, Sullivan CT, Gelrud A. Single balloon enteroscopy (SBE) assisted therapeutic endoscopic retrograde cholangiopancreatography (ERCP) in patients with Roux-en-Y anastomosis. Dig Dis Sci 2014; 59 (02) 465-470
- 122 Wagh MS, Draganov PV. Prospective evaluation of spiral overtube-assisted ERCP in patients with surgically altered anatomy. Gastrointest Endosc 2012; 76 (02) 439-443
- 123 Lennon AM, Kapoor S, Khashab M. et al. Spiral assisted ERCP is equivalent to single balloon assisted ERCP in patients with Roux-en-Y anatomy. Dig Dis Sci 2012; 57 (05) 1391-1398
- 124 Shah RJ, Smolkin M, Yen R. et al. A multicenter, U.S. experience of single-balloon, double-balloon, and rotational overtube-assisted enteroscopy ERCP in patients with surgically altered pancreaticobiliary anatomy (with video). Gastrointest Endosc 2013; 77 (04) 593-600
- 125 Zouhairi ME, Watson JB, Desai SV. et al. Rotational assisted endoscopic retrograde cholangiopancreatography in patients with reconstructive gastrointestinal surgical anatomy. World J Gastrointest Endosc 2015; 7 (03) 278-282
- 126 Al-Toma A, Beaumont H, Koornstra JJ. et al. The performance and safety of motorized spiral enteroscopy, including in patients with surgically altered gastrointestinal anatomy: a multicenter prospective study. Endoscopy 2022; 54 (11) 1034-1042
- 127 Schneider M, Höllerich J, Gerges C, Balasus N, Neuhaus H, Beyna T. Motorized spiral enteroscopy-assisted ERCP in surgically altered anatomy: early experience from a retrospective cohort study. Endoscopy 2023; 55 (05) 476-481
- 128 Moreels TG, Aabakken L, Arvanitakis M, Knabe M, Beyna T. Correction: enteroscopy-assisted ERCP in patients with surgically altered anatomy: multicenter prospective registry (SAMISEN-B) using motorized spiral enteroscopy. Endosc Int Open 2024; 12 (11) C10-C10
- 129 Nennstiel S, Fried R, Herner A, Schlag C. Motorized spiral enteroscopy assisted endoscopic retrograde cholangiography in patients with Roux-en-Y-anatomy. World J Gastrointest Endosc 2025; 17 (08) 102787
- 130 Weilert F, Binmoeller KF, Marson F, Bhat Y, Shah JN. Endoscopic ultrasound-guided anterograde treatment of biliary stones following gastric bypass. Endoscopy 2011; 43 (12) 1105-1108
- 131 Iwashita T, Yasuda I, Doi S. et al. Endoscopic ultrasound-guided antegrade treatments for biliary disorders in patients with surgically altered anatomy. Dig Dis Sci 2013; 58 (08) 2417-2422
- 132 Itoi T, Sofuni A, Tsuchiya T, Ijima M, Iwashita T. Endoscopic ultrasonography-guided transhepatic antegrade stone removal in patients with surgically altered anatomy: case series and technical review (with videos). J Hepatobiliary Pancreat Sci 2014; 21 (12) E86-E93
- 133 Miranda-García P, Gonzalez JM, Tellechea JI, Culetto A, Barthet M. EUS hepaticogastrostomy for bilioenteric anastomotic strictures: a permanent access for repeated ambulatory dilations? Results from a pilot study. Endosc Int Open 2016; 4 (04) E461-E465
- 134 James TW, Fan YC, Baron TH. EUS-guided hepaticoenterostomy as a portal to allow definitive antegrade treatment of benign biliary diseases in patients with surgically altered anatomy. Gastrointest Endosc 2018; 88 (03) 547-554
- 135 Hosmer A, Abdelfatah MM, Law R, Baron TH. Endoscopic ultrasound-guided hepaticogastrostomy and antegrade clearance of biliary lithiasis in patients with surgically-altered anatomy. Endosc Int Open 2018; 6 (02) E127-E130
- 136 Mukai S, Itoi T, Sofuni A. et al. EUS-guided antegrade intervention for benign biliary diseases in patients with surgically altered anatomy (with videos). Gastrointest Endosc 2019; 89 (02) 399-407
- 137 Huang P, Zhang H, Zhang XF, Lv W, Fan Z. Application and value of endoscopic ultrasonography guided biliary interventional therapy in patients with biliary obstruction and surgically altered anatomy. Surg Laparosc Endosc Percutan Tech 2020; 30 (05) 454-458
- 138 Minaga K, Takenaka M, Ogura T. et al. Endoscopic ultrasound-guided biliary drainage for malignant biliary obstruction with surgically altered anatomy: a multicenter prospective registration study. Therap Adv Gastroenterol 2020; 13: 1756284820930964