

Subscribe to RSS
DOI: 10.4103/ajns.AJNS_273_17
Adult achondroplasia patient with extensive long segment severe C1 to C6 segment spinal canal stenosis: Unique presentation
Authors

Achondroplasia represents the common variety of skeletal dysplasia causing short-limb dwarfism. It may be associated with congenial craniovertebral junction anomaly, including atlantoaxial dislocation, Os odointoideum or basilar invagination or acquired as a result of the previous foramen magnum region surgery. However, long segment cervical compression from the first cervical vertebra region to sixth cervical region, such extensive compression producing myelopathy is not reported, and current case represents first case in the western literature. He was managed surgically with a good outcome. Perioperative management along with brief review of pertinent literature along with the management of such case is discussed in brief. Anesthetic management of such patient with coexisting extensive cervical compression presents unique challenges in view of the multisystem involvement along with preexisting anatomical and physiological constraints.
Key-words:
Achondroplasia - anesthesia management - dwarfism - long segment cervical compression - myelopathyIntroduction
Achondroplasia is a disorder of endochondral bone ossification, characterized by rhizomelic involvement of the extremity, and hence proximal limb bones, i.e., the humerus and femur are relatively more involved than compared to distal bones.[[1]],[[2]],[[3]] The disproportionate affection of limbs is responsible to produce disproportionate dwarf with overall short stature but a normal-sized torso.[[4]],[[5]] Achondroplasia represents the most common form of short-limbed dwarfism. Its incidence is approximately 1 in 25,000 live births, and equally common in males as females.[[1]]
Genetically, achondroplasia is caused by mutations in the FGFR3 gene, which controls protein synthesis required for growth and maintenance of bone. Clinical findings include delayed motor development, short stature, and large head. It can be detected before birth by the prenatal ultrasound.[[2]] At birth, skull X-ray may show frontal bossing, with enlarged calvarium and mandible with typical hypoplasia of the midface. With hands and feet showing short phalanges and fingers of equal length.[[2]],[[3]] Authors report perioperative management of unique case in adult, who underwent successful cervical laminoplasty with the good neurological outcome.
Case Report
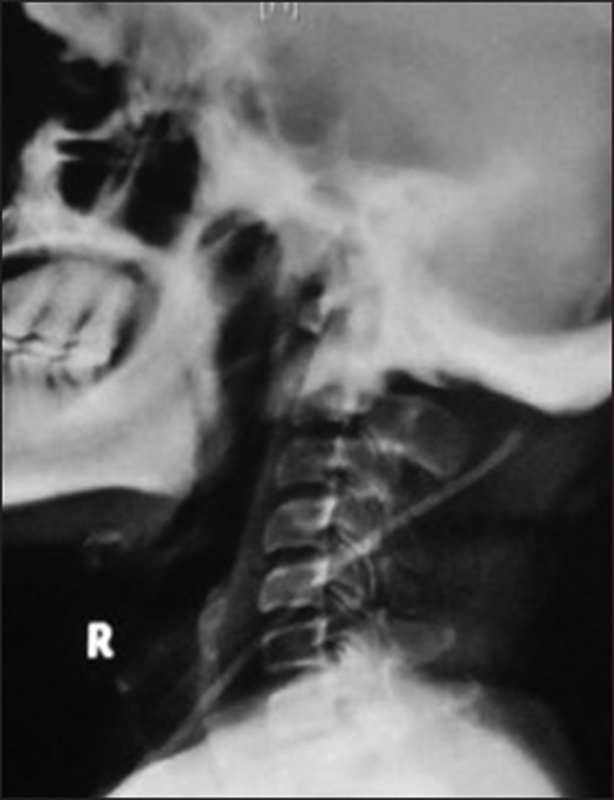
A-35-year-old male, known case of achondroplasia, presented with progressive spastic quadriparesis with difficulty in walking and difficulty in writing for 4 years and wheel-chair bound for 2 months. He had the typical phenotype of achondroplasia, with hypertonia in all four limbs, with grade 3–4/5 with brisk deep tendon jerk and bilateral Babinski's extensor response with a graded sensory loss up to sixth cervical dermatome. X-ray cervical spine showed straightening of the lordotic curve [[Figure 1]]. CT cervical spine revealed spinal canal stenosis at c1 to c6 level, [[Figure 2]] and [[Figure 3]] magnetic resonance imaging (MRI) cervical spine T2-weighted image revealed severe canal stenosis with signal alternation from c1 to c6 level [[Figure 4]], [[Figure 5]]. He underwent c1-c2 laminectomy and c3 to c6 laminoplasty.[[5]]




Discussion
Achondroplasia is the most common type of skeletal dysplasia resulting in short limb dwarfism.[[6]] Spine imaging shows decreased the height of the vertebral body, narrowing of the interpedicular distance, and relatively shorter and thicker pedicle leading to narrow anteroposterior canal diameter causing spinal stenosis.
1991, Ferrante et al. reported in the spinal canal stenosis is a very frequent finding in achondrplastic ossification.[[1]] Spinal stenosis is common association due to achondrplastic ossification of the vertebra.[[1]] However, cervical stenosis mostly occurs at the cervicomedullary junction and upper cervical canal stenosis, is most commonly occur due to the involvement of the first metameres and the craniospinal junction, is more common in infancy or rarely children, while thoracolumbar stenosis occurs in adults. Cervical canal stenosis causing spastic quadriparesis with respiratory insufficiency is quite common in infancy. However, it is not reported in adult until date in western literature.[[1]]
The compression at foramen magnum is attributed by hypertrophy of occipital posterior rim leading to cervicomedullary compression, decrease the transverse diameter of the spinal canal, and hypoplastic arches of the atlas and other vertebra is responsible for spinal stenosis.[[2]] Intraoperatively, Keiper et al. observed compressing agents were an anterior extension of squamous part of the occipital bone, thickened superior rim of the foramen magnum, and dense fibrous epidural band.[[4]] Surgery is usually advocated to relieve pressure on the neural tissue including decompression of foramen magnum and often laminectomy of C1 and other vertebra depending on the extent of spinal stenosis.[[2]] The surgical indications for cervical stenosis depend mainly on the clinical and radiological detailed evaluation. Benglis and Sandberg advocated prophylactic surgery in even asymptomatic patients with osseous compression at foramen magnum, if MRI spine, on T2-weighted image shows signal alteration to avoid sudden neurological deterioration in the event of minor trauma.[[3]] As these cases may suffer with excessive anxiety in addition to neurological deficit warranting detailed counseling and drug management.[[7]] The excessive excess subcutaneous tissues fat deposit and lax skin produce difficulty in peripheral venous cannula placement.[[8]]
The airway management remains most difficult task due to the presence, short neck, and cervical compression.[[9]] We strongly advocate awake fiberoptic intubation with a cervical collar in situ, injection of dexamethasone 4 mg intravenously and skull traction applied with Gardener-wells tongs. Nasogastric tube insertion may be required in the immediate postoperative period and may suffer obstructive sleep apnea is more prevalent necessitating the judicious use of narcotic medication in such cases.[[9]]
Cardiac and respiratory functions may be compromised due to the flattened rib cage, rib hypoplasia; restrictive pulmonary disease needing special anesthetic respiratory care with pressure-controlled ventilation with high respiratory rate and low-tidal-volume was the appropriate and safer strategy for intraoperative and postoperative ventilation. These patients are prone to develop pulmonary complications such as atelectasis with pneumonia hence vigorous chest physiotherapy incentive spirometry and early ambulation with limb physiotherapy to avoid the risk of deep venous thrombosis.[[10]]
Keiper et al.[[4]] analyzed 11 cases infant and noted two cases needed urgent surgery due to severe cervicomedullary compression and another two needed surgery at 3 months of age as they developed opisthotonus. Moreover, advocated suboccipital craniectomy and laminectomy of the atlas. As cases with achondroplasia have a normal lifespan. The symptomatic patient should undergo surgical decompression at the earliest opportunity to provide a good neurological outcome.[[4]]
Conclusion
Peri-operative management including anesthetic consideration of achondroplasia cases remains challenging. Authors strongly advocated awake intubation with fiber-optic tube, with cervical collar in situ, head further immobilized using Gardner-Wells's skull traction and intravenous injection of dexamethasone during intubation of such cases can result in good neurological outcome.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Ferrante L, Acqui M, Mastronardi L, Celli P, Fortuna A. Stenosis of the spinal canal in achondroplasia. Ital J Neurol Sci 1991;12:371-5.
- 2 Jha RM, Klimo P, Smith ER. Foramen magnum stenosis from overgrowth of the opisthion in a child with achondroplasia. J Neurosurg Pediatr 2008;2:136-8.
- 3 Benglis DM, Sandberg DI. Acute neurological deficit after minor trauma in an infant with achondroplasia and cervicomedullary compression. Case report and review of the literature. J Neurosurg 2007;107:152-5.
- 4 Keiper GL Jr., Koch B, Crone KR. Achondroplasia and cervicomedullary compression: Prospective evaluation and surgical treatment. Pediatr Neurosurg 1999;31:78-83.
- 5 Li Q, Kong Q, Zhang L, Sun T, Li T, Gong Q, et al. Discussion of surgical indications for posterior expansive open-door laminoplasty extended to C1 level. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2013;27:1214-20.
- 6 Kaushal A, Haldar R, Ambesh P. Anesthesia for an achondroplastic individual with coexisting atlantoaxial dislocation. Anesth Essays Res 2015;9:443-6.
- 7 Kalla GN, Fening E, Obiaya MO. Anaesthetic management of achondroplasia. Br J Anaesth 1986;58:117-9.
- 8 Jain A, Jain K, Makkar JK, Mangal K. Anaesthetic management of an achondroplastic dwarf undergoing radical nephrectomy. S Afr J Anaesthesiol Analg 2010;16:77-9.
- 9 Krishnan BS, Eipe N, Korula G. Anaesthetic management of a patient with achondroplasia. Paediatr Anaesth 2003;13:547-9.
- 10 Sisk EA, Heatley DG, Borowski BJ, Leverson GE, Pauli RM. Obstructive sleep apnea in children with achondroplasia: Surgical and anesthetic considerations. Otolaryngol Head Neck Surg 1999;120:248-54.
Address for correspondence
Publication History
Article published online:
09 September 2022
© 2019. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Ferrante L, Acqui M, Mastronardi L, Celli P, Fortuna A. Stenosis of the spinal canal in achondroplasia. Ital J Neurol Sci 1991;12:371-5.
- 2 Jha RM, Klimo P, Smith ER. Foramen magnum stenosis from overgrowth of the opisthion in a child with achondroplasia. J Neurosurg Pediatr 2008;2:136-8.
- 3 Benglis DM, Sandberg DI. Acute neurological deficit after minor trauma in an infant with achondroplasia and cervicomedullary compression. Case report and review of the literature. J Neurosurg 2007;107:152-5.
- 4 Keiper GL Jr., Koch B, Crone KR. Achondroplasia and cervicomedullary compression: Prospective evaluation and surgical treatment. Pediatr Neurosurg 1999;31:78-83.
- 5 Li Q, Kong Q, Zhang L, Sun T, Li T, Gong Q, et al. Discussion of surgical indications for posterior expansive open-door laminoplasty extended to C1 level. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2013;27:1214-20.
- 6 Kaushal A, Haldar R, Ambesh P. Anesthesia for an achondroplastic individual with coexisting atlantoaxial dislocation. Anesth Essays Res 2015;9:443-6.
- 7 Kalla GN, Fening E, Obiaya MO. Anaesthetic management of achondroplasia. Br J Anaesth 1986;58:117-9.
- 8 Jain A, Jain K, Makkar JK, Mangal K. Anaesthetic management of an achondroplastic dwarf undergoing radical nephrectomy. S Afr J Anaesthesiol Analg 2010;16:77-9.
- 9 Krishnan BS, Eipe N, Korula G. Anaesthetic management of a patient with achondroplasia. Paediatr Anaesth 2003;13:547-9.
- 10 Sisk EA, Heatley DG, Borowski BJ, Leverson GE, Pauli RM. Obstructive sleep apnea in children with achondroplasia: Surgical and anesthetic considerations. Otolaryngol Head Neck Surg 1999;120:248-54.