
RSS-Feed abonnieren
DOI: 10.1055/a-2191-2310
Combination of endoscopic full-thickness resection and laparoscopic intragastric surgery for gastric submucosal tumor

Gastric submucosal tumors (SMTs) can be reliably resected in a minimally invasive manner using endoscopic full-thickness resection (EFTR) because, for example, they do not require mesenteric processing. However, there are many issues regarding suture methods, device costs, technique difficulty, and suturing certainty. Laparoscopic intragastric surgery allows secure suturing of the stomach wall from within the stomach by laparoscopy [1]. Although the combination of these two methods has not been reported, our experience indicates that it enables safer and less invasive treatment. We are convinced that this technique is particularly well suited for patients in whom oral tumor retrieval is impossible or suturing is difficult using only a flexible endoscope because a laparoscopic port is required.
CASE 1: A 76-year-old man had a 30-mm SMT with delle at the lesser curvature of the upper gastric body ([Fig. 1]). Emergency surgery was required because of tumor hemorrhage. The patient strongly preferred minimally invasive EFTR instead of gastrectomy. The tumor was smoothly resected, but endoscopic ligation with O-ring closure (E-LOC method) [2] [3] using a flexible endoscope alone was too difficult because of the high number of blood clots. Therefore, we switched to laparoscopic intragastric surgery. The gastric wall was tractioned to the umbilical wound, incised, and laparoscopically sutured in only 13 minutes ([Fig. 2], [Video 1]).


Video 1 This video demonstrates the clinical utility of combining endoscopic full thickness resection and laparoscopic intragastric surgery to treat a gastric submucosal tumor.
Qualität:
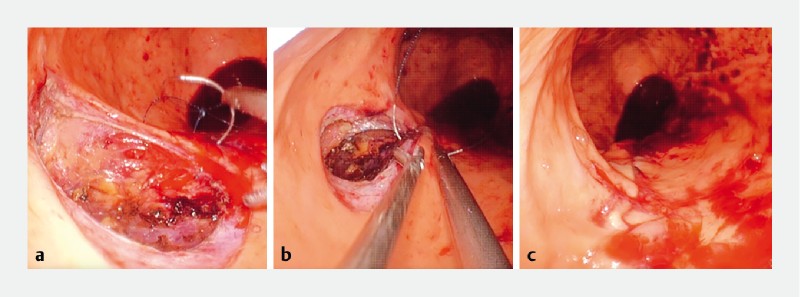
CASE 2: A 75-year-old woman had a 25-mm SMT at the posterior wall of the middle gastric body. After the tumor had been resected by EFTR ([Fig. 3]), the patient’s pharynx was lacerated during insertion of an overtube that was used to orally extract the tumor ([Fig. 4]). We switched to laparoscopic intragastric surgery, which allowed for secure suturing and safe retrieval through the port ([Fig. 5]). Both patients had good postoperative courses. From these experiences, we are convinced that the innovative combination of resection by EFTR and suture and retrieval by laparoscopic intragastric surgery is an effective method.


Endoscopy_UCTN_Code_CCL_1AB_2AD_3AB
E-Videos is an open access online section of the journal Endoscopy, reporting on interesting cases and new techniques in gastroenterological endoscopy. All papers include a high-quality video and are published with a Creative Commons CC-BY license. Endoscopy E-Videos qualify for HINARI discounts and waivers and eligibility is automatically checked during the submission process. We grant 100% waivers to articles whose corresponding authors are based in Group A countries and 50% waivers to those who are based in Group B countries as classified by Research4Life (see: https://www.research4life.org/access/eligibility/).
This section has its own submission website at https://mc.manuscriptcentral.com/e-videos
#
Competing interests
The authors declare that they have no conflict of interest.
-
References
- 1 Ohashi S. Laparoscopic intraluminal (intragastric) surgery for early gastric cancer. A new concept in laparoscopic surgery. Surg Endosc 1995; 9: 169-171
- 2 Nishiyama N, Kobara H, Kobayashi N. et al. Novel endoscopic ligation with O-ring closure involving muscle layer of a gastric artificial defect. Endoscopy 2020; 52: E413-E414
- 3 Kobara H, Nishiyama N, Fujihara S. et al. Traction-assisted endoscopic full-thickness resection followed by O-ring and over-the-scope clip closure in the stomach: an animal experimental study. Endosc Int Open 2021; 9: E51-E57
Corresponding author
Publikationsverlauf
Artikel online veröffentlicht:
14. November 2023
© 2023. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Ohashi S. Laparoscopic intraluminal (intragastric) surgery for early gastric cancer. A new concept in laparoscopic surgery. Surg Endosc 1995; 9: 169-171
- 2 Nishiyama N, Kobara H, Kobayashi N. et al. Novel endoscopic ligation with O-ring closure involving muscle layer of a gastric artificial defect. Endoscopy 2020; 52: E413-E414
- 3 Kobara H, Nishiyama N, Fujihara S. et al. Traction-assisted endoscopic full-thickness resection followed by O-ring and over-the-scope clip closure in the stomach: an animal experimental study. Endosc Int Open 2021; 9: E51-E57