

Subscribe to RSS
DOI: 10.1055/s-0043-118111
Brain and Spinal Cord MRI in Multiple Sclerosis: an Update
Authors
Correspondence
Publication History
Publication Date:
18 October 2017 (online)
- Abstract
- Introduction
- The Role of Imaging in the Diagnosis of MS
- The Role of Imaging in MS Monitoring
- References
Abstract
Magnetic resonance imaging (MRI) plays an important role in the diagnosis of multiple sclerosis and has been incorporated into the McDonald diagnostic criteria for MS. In particular, for the exclusion of important differential diagnosis and comorbidities, new MRI markers have been established such as the “central vein sign”. In addition to diagnostic purposes, the role of MRI in MS monitoring is becoming increasingly important, particularly for pharmacovigilance. This includes treatment efficacy monitoring, prediction of treatment response and safety monitoring. Quantitative MRI methods and ultra-high-field MRI offer the opportunity for the quantitative assessment of damage in normal-appearing brain tissue. However, the standardization of these techniques with the goal of implementation in clinical routine will be one of the major challenges in the near future.
Introduction
Multiple sclerosis (MS) is the most common chronic-inflammatory demyelinating disease of the central nervous system (CNS) [1]. In addition to clinical presentation and examination of the cerebrospinal fluid, imaging, in particular magnetic resonance imaging (MRI), plays an important role in the diagnosis and disease monitoring of MS [2] [3]. The increased relevance of MRI of the brain and spinal cord in the course of MS diagnosis has had a lasting effect on the design and modification of MS diagnostic criteria (McDonald criteria) [4]. The primary focus is on the detection of chronic inflammatory and neurodegenerative changes in the brain and spinal cord. Alternative pathophysiological theories such as the detection of chronic venous insufficiency have conclusively proved to be clearly wrong [5]. Large cohort studies also showed the prognostic value of MRI markers for long-term disability and the appearance of new clinical relapses. However, the overall prognostic value of MRI measures remains rather limited [6] [7]. Recently, international expert guidelines have clearly defined the role of MRI in diagnosis. Emphasis was placed on the need for standardization of MS imaging regarding image acquisition and examination intervals [8] [9] [10].
Compared to the long-established role of MRI in MS diagnostics, the relevance of imaging for observation or monitoring of the course of the disease had been long neglected. The introduction of new drug therapies with different and ever more effective mechanisms of action made apparent the importance and necessity of stringent treatment monitoring (pharmacovigilance) using MRI [11] [12] [13] [14]. Accordingly, the previously mentioned international expert guidelines have been extended to include MRI follow-up of disease activity within the framework of the MS treatment [8] [9] [10].
Recent developments in MR imaging have significantly influenced the possibilities of improving in vivo detection of MS pathology. Such advances include the use of new pulse sequences, image acquisition at higher field strength and the use of quantitative MRI methods such as MR spectroscopy, diffusion tensor imaging and functional imaging [15] [16] [17] [18] [19] [20] [21]. These new and quantitative MRI methods allow us to investigate MS pathology in CNS structures that remain largely hidden by “conventional” MRI pulse sequences. Among other things, this affects examination of the cortical and deep grey matter as well as normal-appearing white (NAWM) and gray matter (NAGM) appearing on conventional pulse sequences [22] [23] [24] [25].
The aim of this review is to provide an up-to-date overview of the importance of MRI of the brain and spinal cord during the diagnosis and monitoring of MS in the context of recently published expert guidelines.
The Role of Imaging in the Diagnosis of MS
Standardized examination protocol
For several years, there have been increasing national and international efforts to implement a standardized examination protocol. This is essentially due to the body of data that unequivocally demonstrates that image acquisition parameters (e.g., magnetic field strength, local resolution, pulse sequence selection, repositioning) can significantly affect the detection of MS lesions [26] [27] [28].
International expert groups, such as the European MAGNIMS Group and the Canadian/North American Consortium of MS Centers (CMSC), have a introduced a standardized protocol for imaging of the brain ([Table 1]) and the spinal cord ([Table 2]) based on recent developments in the field of MS imaging [4] [5] [6]. These suggestions are increasingly implemented by national specialist groups [29]. There are special issues regarding MRI examination of the optic nerve that should include dedicated pulse sequences as in a standardized acquisition protocol as suggested by international expert panel guidelines [30].
|
Baseline MAGNIMS MRI (4, 5) |
Baseline CMSC MRI (6) |
Follow-up MAGNIMS MRI (4, 5) |
|
|---|---|---|---|
|
Axial PD and/or T2-FLAIR/T2-weighted (T)SE |
Yes |
Yes, 3D sequence |
Recommended |
|
Sagittal 2D or 3D T2-FLAIR |
Yes |
Yes** |
No |
|
2D or 3D T1-weighted after IV contrast* |
Yes |
Yes** , before and after IV contrast |
Yes |
|
2D or isotropic T1-weighted 3D |
Optional |
Yes** |
Optional |
|
2D and/or 3D DIR |
Optional |
No |
Optional |
|
Axial diffusion-weighted |
Optional |
No |
No |
*Standard contrast medium dose (single dose), 0.1 mmol/kg bodyweight
** 3D acquisition before and after IV contrast
MAGNIMS=Magnetic Resonance Imaging in MS, CMSC=Consortium of MS Centers, PD=Proton Density, DIR=Double Inversion Recovery, IV= intravenous
|
Baseline MRI |
Baseline MRI |
|
|---|---|---|
|
MAGNIMS (4, 5) |
CMSC (6) |
|
|
Single-echo T2 |
Sagittal (when combined with STIR) (axial slices optional) |
Sagittal, axial in region of lesions |
|
Dual-echo PD/T2 |
Sagittal |
Alternative to T2 |
|
STIR |
Alternative to PD |
Sagittal |
|
2D or 3D T1 after IV contrast |
Sagittal |
Sagittal, optional |
|
PSIR |
Sagittal, optional |
(PST1-IR) |
MAGNIMS=Magnetic Resonance Imaging in MS, CMSC=Consortium of MS Centers, STIR=Short-Tau Inversion Recovery, PSIR=Phase Sensitive Inversion Recovery, PST1-IR=Phase Sensitive T1 Inversion Recovery, V= intravenous
In Europe, there is consensus that imaging of the brain should take place preferably at 3 Tesla (T) due to the higher signal yield and improved detection of MS lesions compared to lower magnetic field strengths [17] [31]. A spatial resolution with a slice thickness of 3 mm and an in-plane resolution of 1×1 mm is recommended for two-dimensional (2D) pulse sequences. Regardless of field strength, isotropic 3D image acquisition is recommended, especially for the fluid-attenuated inversion recovery (FLAIR) sequence. This allows better contrast yield, multiplanar reconstruction, co-registration of follow-up examinations as well as the application of automated segmentation techniques [8] [32] [33] [34] [35]. Although higher doses of contrast media reveal a greater number of enriched MS lesions, nevertheless a standard dose of 0.1 mmol/kg of body weight is recommended. This should be particularly noted in light of current discussions regarding the accumulation of certain gadolinium-based contrast media in certain deep gray matter brain structures such as the dentate nucleus[8] [36]. In the context of MS diagnosis, spinal cord imaging plays an especially important role. However, compared to brain imaging, imaging of the spinal cord is more demanding, mainly due to increased susceptibility to artifacts (pulsation of the heart and large thoracic vessels, cerebrospinal pulsations) [37]. In contrast to brain imaging, it has not been possible to show conclusively that a higher field strength of 3T results in an improved detection rate for spinal imaging [38]. Just as for cerebral imaging, a standard spatial resolution with a voxel size of 3×1×1 mm is recommended for 2D sequences. The benefit of contrast media for spinal imaging remains unclear and controversial. Only a small fraction of spinal MS lesions shows contrast enhancement and these lesions are also often clinically symptomatic [37] [39].
Imaging in the context of MS diagnosis criteria and differential diagnosis
Localization of MS lesions, the presence of contrast-enhancement, and the formation of new lesions in the course of the disease are crucial for MS diagnosis within the framework of the McDonald criteria regarding the demonstration of dissemination in space (DIS) and in time (DIT) ([Table 3]). By applying the 2010 revision of the McDonald criteria it is now possible to establish the diagnosis of MS in a patient with clinically isolated syndrome and simultaneous presence of lesions with and without contrast-enhancement in the case the contrast-enhancing lesions is asymptomatic. Otherwise, the criterion of DIT is considered to be fulfilled if a new typical T2w lesion or a new contrast-enhancing lesion is present in a follow-up exam without temporal limitation [4]. Typical imaging examples are shown in [Fig. 1]. Important criticisms of the McDonald criteria and recent study results resulted in a recently published work of the European MAGNIMS collaboration which offered an alternative proposal for the detection of DIS which does not differentiate between cortical/juxtacortical and symptomatic/asymptomatic lesions [40].

|
DIT |
A new T2 or CM lesion compared to a previous examination without temporal limitation or a juxtaposition of asymptomatic CM-receptive and T2 lesions |
Evidence meets the criterion of dissemination in time (DIT) |
|
DIS |
At least one T2 hyperintense lesion in at least 2 of the 4 following locations: periventricular, juxtacortical, infratentorial, spinal (a symptomatic brain stem or spinal cord lesion is ruled out) |
Evidence meets the criterion of dissemination in space (DIS) |
The spectrum of differential diagnoses of cerebral and spinal MS pathology is wide and heterogeneous. Please refer to a recently published overview for a detailed description and discussion of the differential diagnoses [41]. Differential diagnosis is also made more difficult by the fact that focal MS lesions can present with different forms and sizes, with different patterns of blood-brain barrier interference/contrastenhancement. In addition to the distinction of rare or atypical variants of idiopathic inflammatory demyelinating lesions (tumefactive demyelination (see [Fig. 2])), “Balo-like lesions”, hemorrhagic encephalomyelitis), emphasis is also put on the differentiation of other inflammatory and vascular lesions [42] [43]. The spinal cord plays a decisive role in this process. In the vast majority of MS patients, the spinal cord (see [Fig. 3]) is frequently affected but it is rarely impacted by vascular diseases [44]. Due to the increased use of higher magnetic field strengths, the diagnostic attribute of the perivascular localization of MS lesions (“central vein sign”) is becoming increasingly important (see [Fig. 4]). Recent data suggest that perivascular lesion distribution is useful in differentiating MS lesions from lesions of other MS differential diagnoses (e.g., vascular lesions, Susac’s syndrome, neuromyelitis optica) [45] [46] [47] [48]. Despite the enthusiasm, however, it should be noted that both the imaging and interpretation of the central vein sign are not yet completely standardized, but international expert groups are currently developing a standard [49].



New imaging technologies for the diagnosis of MS
Recent developments in structural imaging include, but are not limited to, 3D acquisition techniques and the use of (ultra) high-field MRI or a combination of both. A common application is the detection of cortical lesions. Due to increasing evidence that cognitive symptoms (e.g., epilepsy) in MS patients may be related to cortical lesion load advances cortical lesion detection are gaining clinical relevance [50] [51]. Particularly relevant in this respect is the double inversion recovery (DIR) pulse sequence [31], see [Fig. 5]. Furthermore, the detection of leptomeningeal inflammation, which is also presumed to have particular clinical relevance with respect to the disability of MS patients, is becoming increasingly the focus of diagnostics using 3D sequences at higher magnetic field strenghts[52]. However, the benefit of MRI regarding lesion detection (sensitivity, specificity) and the correlation with clinical parameters has been insufficiently investigated and is not clearly clarified [53].

In addition to standard sequences, further contrasts are used in the investigation and characterization of MS-induced parenchymal changes [54]. The following briefly describes some methods which can make a significant contribution to the detection of tissue damage and which can provide quantifying data.
Normal T1w sequences can be combined with a magnetization transfer technique (MT) in which impulse modulation induces energy transfer between protons of macromolecules; these macromolecules thus contribute to the signal arising from the tissue [55]. Demyelination reduces this magnetization transfer effect and it is improved by remyelination. However, examination time is extended by this sequence modulation and the contrast between the cortex and the white matter is decreased, but a contrast enhancement effect can be improved. Therefore, the method should not be applied after administration of i.v. gadolinium based contrast, since the pure contrast effect can no longer be assessed due to the signal modulation of the MT effect. The magnetization transfer ratio (MTR) can be determined without contrast administration, since it results from the signal difference between images with and without MT pulse. However, gradient echo sequences are usually used for the calculation of MTR mapping due to the comparatively stronger MT effect. This method is not used in the clinical routine, since comparability is difficult between different sites, and the MT effect can also be influenced by non MS-related pathologies [56]. Although this method has long been established and is sometimes labeled “old fashioned”, MTR is regaining relevance as a means of detecting remyelination of new neuroprotective MS drugs [57] [58]. Nevertheless, it should be noted that quantitative values in MTR maps are tissue markers and not specific for de- or remyelination.
The detection and quantification of iron deposits in MS lesions and deep grey matter is becoming increasingly important [59] [60]. These iron deposits can fluctuate as part of the temporal development of an MS lesion and thus contribute to its characterization [59] [61]. In addition to the relatively new susceptibility-weighted imaging (SWI) method, its quantifying variant (quantitative susceptibility mapping=QSM) can also be used for this. These methods are highly sensitive to magnetic field disturbances. The SWI method also provides images with a contrast based on the phase shift of the spins in the voxels caused by field disturbances, thereby distinguishing between a diamagnetic magnetic field disturbance (e.g., calcification) and paramagnetic magnetic field disturbance (e.g., iron). In the QSM method, the susceptibility effects leading to a signal loss and the phase shifts are computed into one image; the QSM signal hyperintensity is proportional to the iron concentration in the tissue causing the field disturbance [59] [62]. However, the issue of the clinical relevance of iron detection and its quantification has not yet been conclusively resolved.
Widely used in stroke diagnosis, diffusion-weighted imaging, in which the signal obtained depends on the statistically possible water mobility in the tissue, can provide information about structural tissue changes. If, as in stroke diagnostics, the apparent diffusion coefficient (ADC) is calculated, it is usually possible to distinguish an acute/early subacute lacunar infarction with its ADC reduction from an MS lesion. The ADC values can also be used to assess tissue areas with seemingly normal appearance in the standard sequences, but more complex diffusion techniques such as diffusion-tensor imaging are more suitable for this. These more extensive diffusion measurements make it possible to determine the direction of the preferred water mobility as well as divide it into its longitudinal and transverse components. Changes in the longitudinal component indicate axonal changes and changes in the transverse component can be interpreted as myelin changes [63] [64] [65] [66] [66].
Another quantifying method is MR proton spectroscopy, which provides non-invasive information about metabolic components in the tissue. Due to their structure, the molecules to be determined lead to a defined displacement of the resonance frequency with their fingerprint-like arrangement of the intramolecular chemical bonds which can be detected and whose signal strength at this specific resonance frequency is essentially proportional to the concentration of the molecule in the tissue. The main metabolites are choline as a marker for cell membrane remodeling, creatine/phosphocreatine as a marker for the energy budget, N-acetyl aspartate (NAA) as a marker for neuronal integrety, lactate as an anaerobic glycolysis marker and myoinositol as a marker for activated glial cells. This method can be used on a standard clinical MRI system, but is usually employed only for research purposes and very special clinical issues (eg. differential diagnosis). Acute inflammatory foci may have elevated choline due to the increased cell membrane remodeling, whereas old MS foci are associated with a reduction of all major metabolites. A raised myoinositol level in apparently normal tissue may indicate an increased risk of developing MS in patients with a clinically isolated syndrome [20] [24] [67] [69] [69]. Advances in image acquisition (e.g., ultra-high-field MRI) open up a further development of MR spectroscopy and focus on other metabolites which play a decisive role in the pathophysiology of MS; these include GABA (γ-aminobutyric acid), glutamate and glutathione [70].
Even older MR methods, such as the quantifying determination of T1, T2* and T2 relaxation times as well as their relaxation rates R (1/T), are again being given greater attention due to the increasing quality of the magnetic field homogeneities and sequence development. Thus it was shown that by determining relaxation parameters and calculating synthetic tissue maps, acute inflammatory lesions and their disruption of the blood-brain barrier could also possibly be identified without administration of contrast [71].
The Role of Imaging in MS Monitoring
Compared to its use in MS diagnostics, the role of MRI for MS monitoring purposes has been less investigated. Basically this concerns monitoring of MS treatment. Although the concept of pharmacovigilance is very often used in the context of safety monitoring, it also includes monitoring of MS disease activity and the prediction of treatment response. Standardized data collection is hindered by the fact that MS patients comprise a large and heterogeneous group. The spectrum of currently available MS therapeutics is broad, and the range of patients is heterogeneous with respect to treatment history and comorbidity. This likewise hinders the development of evidence-based guidelines on this issue.
Monitoring disease activity and treatment efficiency
MRI has been established as a method for observing inflammatory disease activity and is routinely used to monitor the effectiveness of MS treatment. Due to its high sensitivity, MRI can detect subclinical disease activity. Important and currently recommended MRI parameters for disease progression are contrast-enhancing as well as active (new or enlarging) T2 lesions [8] [9] [10] [72] [73]. The sensitivity of MRI with regard to the detection of these active T2 lesions within the scope of disease monitoring can be further enhanced by MRI subtraction techniques [74] [75]. Neurodegenerative changes occur very early in the course of the disease, although inflammatory changes are radiologically the forefront in the beginning of the disease [23] [76]. Neurodegenerative changes, such as atrophy and loss of cortical thickness, continue to accelerate during the course of the disease and correlate with clinical findings such as decline in cognition, fatigue, and disease progression [77] [78] [79] [80]. Neurodegeneration is pathophysiologically very complex in MS and can be influenced by various factors such as alcohol consumption, smoking, dehydration, APOE*ε4 or cardiovascular comorbidity [81]. A very important factor is that anti-inflammatory therapies can lead to a clear reduction in brain volume in the first year of treatment, which then stabilizes again in the second year of treatment. This phenomenon is referred to as “pseudoatrophy”; because of this, in addition to the difficulty of standardizing atrophy measurements (e.g., various hardware and software for post-processing and data analysis), interpretation of atrophy (eg, brain volume) data is challenging in clinical practice [77] [80] [81]. This has led to the recommendation that atrophy measurement cannot be used yet as a marker for the monitoring of MS patients [9].
In addition to volumetric methods, there are a number of other quantitative MRI methods with the help of which microstructural pathological changes in MS, especially in NAWM and NAGM, can be detected. These include functional MRI (fMRI), in addition to the previously-described MR spectroscopy, diffusion tensor imaging and the magnetization transfer method. Similar to atrophy measurement, the standardized application of these quantitative MRI methods in clinical routine is a challenge, and is not recommended at present because of the relatively long acquisition time required and the difficulty of adequate standardization [9]. A detailed description of all methods used for MS diagnostics and follow-up observation would go far beyond the focus of this review. Nevertheless, it should be stressed that these methods are of crucial importance for the newer generation of MS therapeutics which are primarily aimed at neuroprotection and remyelination. Conventional MRI markers such as active T2 lesions or contrast-enhancing lesions are not suitable for monitoring neuroprotection and remyelination. Animal experiments and initial human in vivo studies using diffusion tensor imaging, magnetization transfer and myelin water fraction imaging are promising [82] [83].
Prediction of treatment response
In recent years, several attempts have been made to establish a link between MRI parameters of MS disease activity before the start of a treatment and the success of that treatment. There are initial, but inconclusive, hints that disease activity measured by MRI can be helpful in identifying responders or non-responders. However, this strategy has not yet been proven in clinical practice and is therefore not recommended [84]. Likewise, the application of quantitative MRI methods, such as atrophy measurements or spinal imaging is difficult to standardize and not recommended for this clinical situation [9].
One established strategy is the detection of disease activity a few months after the start of treatment (reference MRI) and performance of a follow-up exam approximately 12 months after treatment start. The disease activity detected clinically (clinical relapses) and radiologically (active T2 lesions) between these two MRI examinations can be helpful in predicting the long-term treatment response and, consequently, to distinguish between responders and non-responders. It is important to realize that this concept of predicting treatment outcome has been established exclusively for interferon treatment in treatment naïve patients [85] [86] and is not entirely non-controversial or is not practiced in some countries (including due to resource problems). In addition, this concept has not been established for other (second line) MS drugs with other pharmacodynamic aspects and earlier or later treatment effects [73] [87].
Safety monitoring
The introduction of the new generation of MS therapeutics with an improved efficacy profile and with a shift from immunomodulation to increased immunosuppression has made safety monitoring using MRI more important. The spectrum of safety monitoring includes the detection of clinically relevant non-infectious comorbidity, paradoxical MS disease activity and the identification of opportunistic infections [11] [12] [13] [14].
In general, any morbidity of normal aging healthy individuals can also occur as comorbidity in MS patients, without any association with a particular therapy. This range of comorbidities includes, among others, vascular entities, neoplasms and inflammatory changes. An unwanted or unexpected MS disease activity is not per se a safety problem in MS treatment. Nevertheless, during MS therapy, so-called paradoxical, i.e., excessive, MS disease activity such as tumefactive demyelination can infrequently be observed. This phenomenon has been observed especially in some patients directly after the initiation of fingolimod therapy with tumefactive demyelinating lesions. It is currently unknown why a few MS patients react to this drug with an increase in inflammatory disease activity [88] [89].
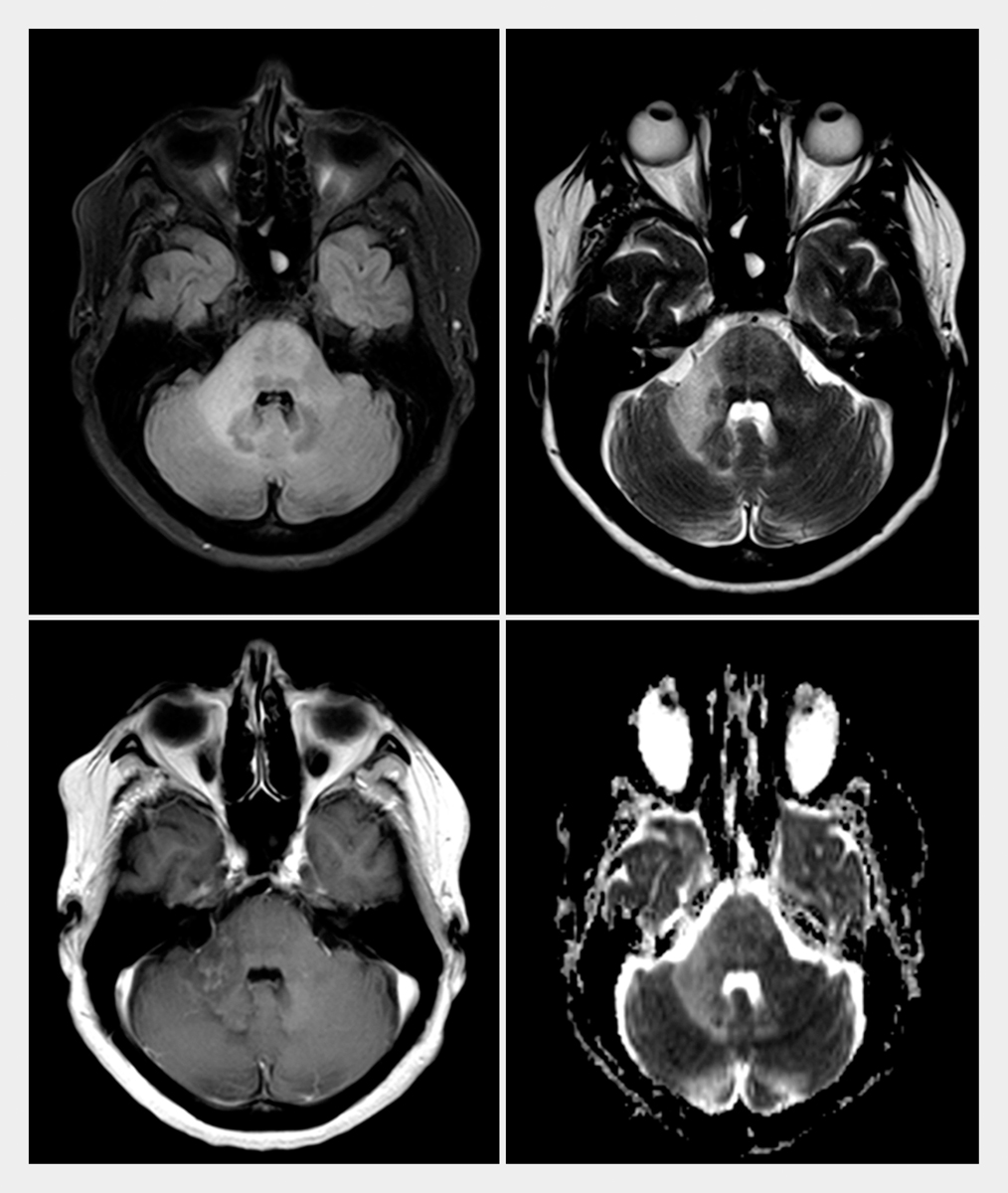
The occurrence of opportunistic infections is a rare but clinically relevant and potentially life-threatening complication of immunosuppressive treatments. Progressive multifocal leukoencephalopathy (PML) is the most frequent opportunistic infection in immunosuppressive therapies in general and in MS therapy in particular [90]. PML arises from a reactivation of the JC virus, a neurotropic polyoma virus, which leads to a lytic infection of white (oligodendrocytes and astrocytes) and grey matter cells, resulting in irreversible demyelination and neuronal damage [91] [92]. It is described as a complication of several MS drugs (e.g., natalizumab, dimethylfumerate, fingolimod), with natalizumab-associated PML being of particular importance with respect to its frequency [93]. As of August 31, 2017, 746 cases of PML have been documented among MS patients receiving natalizumab therapy, a humanized antibody directed against α4 integrin [94]. MRI of the brain is of particular importance in the diagnosis of PML, since it (almost exclusively) affects the brain, but not the optic nerve or spinal cord [95] [96]. Compared to HIV-associated PML, natalizumab-associated PML shows particular imaging findings, especially the relatively frequent occurrence of contrast enhancement within or outside of PML lesions ([Table 4]) [95] [96] [97]. Brain MRI is very sensitive to the detection of these lesions and can identify them at a very early stage while the patient has not yet experienced any clinical symptoms (presymptomatic or asymptomatic PML). Asymptomatic PML lesions are often found in the frontal lobe in the juxtacortical white matter and spreading into the cortical grey matter. However, they may occur more rarely in the deep grey matter or in the posterior fossa (see [Fig. 6]) [97] [98]. Asymptomatic PML patients have a better prognosis than patients with symptomatic PML at the time of diagnosis [99].
|
Multi-sequence protocol for diagnosis and classification of PML |
|
|
Size |
Early stage: Focal lesion <1 cm |
|
Late stage: focal or multifocal lesion up to >3 cm |
|
|
Location |
Frontal > parieto-occiptal > temporal; rarely: infratentorial or deep gray matter |
|
Subcortical white matter with inclusion of U fibers |
|
|
Cortical gray matter frequently also affected |
|
|
Signal intensity |
FLAIR and T2: hyperintense |
|
T1: isointense (early stage), hypointense (later stages) |
|
|
DWI: hyperintense |
|
|
T1 CM: contrast enhancement sign of inflammation in approx. 30% of cases |
|
|
Lesion characteristics |
Sharp boundaries with cortex, indistinct boundaries with white matter |
|
Small T2 lesions (punctate pattern, “milky way”) |
|
|
No atrophy, no mass |
*It is recommended to perform this MRI screening protocol at 3–4 month intervals for patients with an elevated PML risk (high JC virus index, >2 years of natalizumab treatment).
Therefore, European regulatory authorities and international expert groups currently recommend the use of a shortened MRI protocol in high-risk patients every 3–4 months looking for signs of PML ([Table 5]) [9] [100] [101]. In individual cases, it may be very difficult to radiologically distinguish these small focal PML lesions from MS lesions or vascular changes, so that using MRI to support pharmacovigilance requires substantial neuroradiological expertise [102] [103]. Furthermore, other biomarkers such as the CSF JC virus index are currently being used to further support the radiological early diagnosis of PML [104] [105]. Other opportunistic infections are rather rare. Varicella zoster infections are well-documented for fingolimod therapy and very rare cases of Cryptococcal meningitis during natalizumab therapy [106] [107].
|
Multi-sequence protocol for diagnosis and classification of PML |
PML screening protocol* |
|
|---|---|---|
|
Axial T2 FLAIR |
High sensitivity for PML detection |
Recommended |
|
Axial T2-weighted (T)SE |
Detection of classical PML lesion pattern (e.g., small vacuoles, small T2 lesions in the vicinity of the actual PML lesion |
Recommended |
|
T1-weighted after IV contrast* |
Determination of the severity of demyelination (T1 signal intensity) Sign of inflammation (contrast enhancement) |
Not recommended |
|
Axial diffusion weighting |
Detection of active lytic infection with cell swelling and high signal intensity in DWI B1000 image |
Recommended |
*It is recommended to perform this MRI screening protocol at 3-4 month intervals for patients with an elevated PML risk (high JC virus index, >2 years of natalizumab treatment).
Conflict of interest
M. P. Wattjes received consultancy and speaking fees from Biogen, Genzyme, IXICO, Novartis, Roche. P. Raab has nothing to disclose.
-
References
- 1 Compston A, Coles A. Multiple sclerosis. Lancet 2008; 372: 1502-1517
- 2 Wattjes MP, Steenwijk MD, Stangel M. MRI in the Diagnosis and Monitoring of Multiple Sclerosis: An Update. Clin Neuroradiol 2015; 25 (Suppl. 02) 157-165
- 3 Igra MS, Paling D, Wattjes MP. et al. Multiple sclerosis update: Use of MRI for early diagnosis, disease monitoring and assessment of treatment related complications. Br J Radiol 2017; 90: 20160721 10.1259/bjr.20160721
- 4 Polman CH, Reingold SC, Banwell B. et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol 2011; 69: 292-302
- 5 Valdueza JM, Doepp F, Schreiber SJ. et al. What went wrong? The flawed concept of cerebrospinal venous insufficiency. J Cereb Blood Flow Metab 2013; 33: 657-668
- 6 Tintore M, Rovira À, Río J. et al. Defining high, medium and low impact prognostic factors for developing multiple sclerosis. Brain 2015; 138: 1863-1874
- 7 Fisniku LK, Brex PA, Altmann DR. et al. Disability and T2 MRI lesions: a 20-year follow-up of patients with relapse onset of multiple sclerosis. Brain 2008; 131808-131817
- 8 Rovira A, Wattjes MP, Tintoré M. et al. Evidence-based guidelines: MAGNIMS consensus guidelines on the use of MRI in multiple sclerosis-clinical implementation in the diagnostic process. Nat Rev Neurol 2015; 11: 471-482
- 9 Wattjes MP, Rovira A, Miller D. et al. Evidence-based guidelines: MAGNIMS consensus guidelines on the use of MRI in multiple sclerosis--establishing disease prognosis and monitoring patients. Nat Rev Neurol 2015; 11: 597-606
- 10 Traboulsee A, Simon JH, Stone L. et al. Revised recommendations of the consortium of ms centers task force for a standardized mri protocol and clinical guidelines for the diagnosis and follow-up of multiple sclerosis. AJNR Am J Neuroradiol 2016; 37: 394-401
- 11 Kieseier BC, Wiendl H, Hartung HP. et al. Risks and benefits of multiple sclerosis therapies: Need for continual assessment?. Curr Opin Neurol 2011; 24: 238-243
- 12 Dubey D, Cano CA, Stüve O. Update on monitoring and adverse effects of first generation disease modifying therapies and their recently approved versions in relapsing forms of multiple sclerosis. Curr Opin Neurol 2016; 29: 272-277
- 13 Dubey D, Cano CA, Stüve O. Update on monitoring and adverse effects of approved second-generation disease-modifying therapies in relapsing forms of multiple sclerosis. Curr Opin Neurol 2016; 29: 278-285
- 14 Winkelmann A, Loebermann M, Reisinger EC. et al. Disease-modifying therapies and infectious risks in multiple sclerosis. Nat Rev Neurol 2016; 12: 217-233
- 15 Sethi V, Yousry TA, Muhlert N. et al. Improved detection of cortical MS lesions with phase-sensitive inversion recovery MRI. J Neurol Neurosurg Psychiatry 2012; 83: 877-882
- 16 Wattjes MP, Lutterbey GG, Gieseke J. et al. Double inversion recovery brain imaging at 3T: Diagnostic value in the detection of multiple sclerosis lesions. AJNR Am J Neuroradiol 2007; 28: 54-59
- 17 Kilsdonk ID, de Graaf WL, Barkhof F. et al. Inflammation high-field magnetic resonance imaging. Neuroimaging Clin N Am 2012; 22: 135-157
- 18 Wattjes MP, Barkhof F. High field MRI in the diagnosis of multiple sclerosis: High field-high yield?. Neuroradiology 2009; 51: 279-292
- 19 Filippi M, Evangelou N, Kangarlu A. et al. Ultra-high-field MR imaging in multiple sclerosis. J Neurol Neurosurg Psychiatry 2014; 85: 60-66
- 20 Wattjes MP, Harzheim M, Lutterbey GG. et al. High field MR imaging and 1H-MR spectroscopy in clinically isolated syndromes suggestive of multiple sclerosis: Correlation between metabolic alterations and diagnostic MR imaging criteria. J Neurol 2008; 255: 56-63
- 21 Enzinger C, Barkhof F, Ciccarelli O. et al. Nonconventional MRI and microstructural cerebral changes in multiple sclerosis. Nat Rev Neurol 2015; 11: 676-686
- 22 Geurts JJ, Calabrese M, Fisher E. et al. Measurement and clinical effect of grey matter pathology in multiple sclerosis. Lancet Neurol 2012; 11: 1082-1092
- 23 Vigeveno RM, Wiebenga OT, Wattjes MP. et al. Shifting imaging targets in multiple sclerosis: From inflammation to neurodegeneration. J Magn Reson Imaging 2012; 36: 1-19
- 24 Wattjes MP, Harzheim M, Lutterbey GG. et al. Axonal damage but no increased glial cell activity in the normal-appearing white matter of patients with clinically isolated syndromes suggestive of multiple sclerosis using high-field magnetic resonance spectroscopy. AJNR Am J Neuroradiol 2007; 28: 1517-1522
- 25 Pardini M, Sudre CH, Prados F. et al. Relationship of grey and white matter abnormalities with distance from the surface of the brain in multiple sclerosis. J Neurol Neurosurg Psychiatry 2016; 87: 1212-1217
- 26 Wattjes MP, Harzheim M, Lutterbey GG. et al. Does high field MRI allow an earlier diagnosis of multiple sclerosis?. J Neurol 2008; 255: 1159-1163
- 27 Filippi M, Rocca MA, Gasperini C. et al. Interscanner variation in brain MR lesion load measurements in multiple sclerosis using conventional spin-echo, rapid relaxation-enhanced, and fast-FLAIR sequences.. AJNR Am J Neuroradiol 1999; 20: 133-137
- 28 Wattjes MP, Lutterbey GG, Harzheim M. et al. Imaging of inflammatory lesions at 3.0 Tesla in patients with clinically isolated syndromes suggestive of multiple sclerosis: A comparison of fluid-attenuated inversion recovery with T2 turbo spin-echo. Eur Radiol 2006; 16: 1494-1500
- 29 Vågberg M, Axelsson M, Birgander R. et al. Guidelines for the use of magnetic resonance imaging in diagnosing and monitoring the treatment of multiple sclerosis: Recommendations of the Swedish Multiple Sclerosis Association and the Swedish Neuroradiological Society. Acta Neurol Scand 2017; 135: 17-24
- 30 Petzold A, Wattjes MP, Costello F. et al. The investigation of acute optic neuritis: a review and proposed protocol. Nat Rev Neurol 2014; 10: 447-458
- 31 Simon B, Schmidt S, Lukas C. et al. Improved in vivo detection of cortical lesions in multiple sclerosis using double inversion recovery MR imaging at 3T. Eur Radiol 2010; 20: 1675-1683
- 32 Moraal B, Roosendaal SD, Pouwels PJ. et al. Multi-contrast, isotropic, single-slab 3D MR imaging in multiple sclerosis. Eur Radiol 2008; 18: 2311-2320
- 33 Barkhof F, Pouwels PJ, Wattjes MP. The holy grail in diagnostic neuroradiology: 3T or 3D?. Eur Radiol 2011; 21: 449-456
- 34 Moraal B, Wattjes MP, Geurts JJ. et al. Improved detection of active multiple sclerosis lesions: 3D subtraction imaging. Radiology 2010; 255: 154-163
- 35 Schmidt P, Gaser C, Arsic M. et al. An automated tool for detection of FLAIR-hyperintense white-matter lesions in multiple sclerosis. Neuroimage 2012; 59: 3774-3783
- 36 Lukas C, Gold R, Fiehler J. et al Ablagerung von gadoliniumhaltigen Kontrastmitteln im Gehirn nach mehrfacher Anwendung: Konsequenzen für den Einsatz der MRT bei Diagnosestellung und Verlaufsbeurteilung der Multiplen Sklerose?. Akt Neurol 2016; 43: 522-523
- 37 Gass A, Rocca MA, Agosta A. et al. MRI monitoring of pathological changes in the spinal cord in patients with multiple sclerosis. Lancet Neurol 2015; 14: 443-454
- 38 Stankiewicz JM, Neema M, Alsop DC. et al. Spinal cord lesions and clinical status in multiple sclerosis: A 1.5T and 3T MRI study. J Neurol Sci 2009; 279: 99-105
- 39 Bot JC, Barkhof F. Spinal-cord MRI in multiple sclerosis: Conventional and nonconventional MR techniques. Neuroimaging Clin N Am 2009; 19: 81-99
- 40 Filippi M, Rocca MA, Ciccarelli O. et al. MRI criteria for the diagnosis of multiple sclerosis: MAGNIMS consensus guidelines. Lancet Neurol 2016; 15: 292-303
- 41 Dekker I, Wattjes MP. Brain and spinal cord MR imaging features in multiple sclerosis and variants. Neuroimag Clin N Am 2017; 27: 205-227
- 42 Wallner-Blazek M, Rovira A, Fillipp M. et al. Atypical idiopathic inflammatory demyelinating lesions: Prognostic implications and relation to multiple sclerosis. J Neurol 2013; 260: 2016-2022
- 43 Charil A, Yousry TA, Rovaris M. et al. MRI and the diagnosis of multiple sclerosis: Expanding the concept of "no better explanation". Lancet Neurol 2006; 5: 841-852
- 44 Bot JC, Barkhof F, Lycklama à Nijeholt G. et al. Differentiation of multiple sclerosis from other inflammatory disorders and cerebrovascular disease: value of spinal MR imaging. Radiology 2002; 223: 46-56
- 45 Kilsdonk ID, Wattjes MP, Lopez-Soriano A. et al. Improved differentiation between MS and vascular brain lesions using FLAIR* at 7 Tesla. Eur Radiol 2014; 24: 841-849
- 46 Sinnecker T, Dörr J, Pfueller CF. et al. Distinct lesion morphology at 7-T MRI differentiates neuromyelitis optica from multiple sclerosis. Neurology 2012; 79: 708-714
- 47 Kilsdonk ID, Lopez-Soriano A, Kuijer JP. et al. Morphological features of MS lesions on FLAIR* at 7T and their relation to patient characteristics. J Neurol 2014; 261: 1356-1364
- 48 Wuerfel J, Sinnecker T, Ringelstein EB. et al. Lesion morphology at 7 Tesla MRI differentiates Susac syndrome from multiple sclerosis. Mult Scler 2012; 18: 1592-1599
- 49 Sati P, Oh J, Constable RT. et al. The central vein sign and its clinical evaluation for the diagnosis of multiple sclerosis: A consensus statement from the North American Imaging in Multiple Sclerosis Cooperative. Nat Rev Neurol 2016; 12: 714-722
- 50 de Graaf WL, Zwanenburg JJ, Visser F. et al. Lesion detection at seven Tesla in multiple sclerosis using magnetisation prepared 3D-FLAIR and 3D-DIR. Eur Radiol 2012; 22: 221-231
- 51 Kilsdonk ID, Jonkman LE, Klaver R. et al. Increased cortical grey matter lesion detection in multiple sclerosis with 7 T MRI: A post-mortem verification study. Brain 2016; 139: 1472-1481
- 52 Zurawski J, Lassmann H, Bakshi R. Use of magnetic resonance imaging to visualize leptomeningeal inflammation in patients with multiple sclerosis: A review. JAMA Neurol 2017; 74: 100-109
- 53 Kilsdonk ID, Schoonheim M, Wattjes MP. In-vivo imaging of meningeal inflammation in multiple sclerosis: Presence of evidence or evidence of presence?. Mult Scler 2017; 23: 1169-1171
- 54 Giorgio A, De Stefano N. Advanced structural and functional brain MRI in multiple sclerosis. Semin Neurol 2016; 36: 163-176
- 55 Henkelman RM, Huang X, Xiang QS. et al. Quantitative interpretation of magnetization transfer. Magn Reson Med 1993; 29: 759-766
- 56 Brown RA, Narayanan S, Arnold DL. Imaging of repeated episodes of demyelination and remyelination in multiple sclerosis. Neuroimage Clin 2014; 6: 20-25
- 57 Schwartzbach CJ, Grove RA, Brown R. et al. Lesion remyelinating activity of GSK239512 versus placebo in patients with relapsing-remitting multiple sclerosis: A randomised, single-blind, phase II study. J Neurol 2017; 264: 304-315
- 58 Lema A, Bishop C, Malik O. et al. A Comparison of magnetization transfer methods to assess brain and cervical cord microstructure in multiple sclerosis. J Neuroimaging 2017; 27: 221-226
- 59 Ropele S, de Graaf W, Khalil M. et al. MRI assessment of iron deposition in multiple sclerosis. J Magn Reson Imaging 2011; 34: 13-21
- 60 Ropele S, Kilsdonk ID, Wattjes MP. et al. Determinants of iron accumulation in deep grey matter of multiple sclerosis patients. Mult Scler 2014; 20: 1692-1698
- 61 Zhang Y, Gauthier SA, Gupta A. et al. Longitudinal change in magnetic susceptibility of new enhanced multiple sclerosis (MS) lesions measured on serial quantitative susceptibility mapping (QSM). J Magn Reson Imaging 2016; 44: 426-432
- 62 Reichenbach JR. The future of susceptibility contrast for assessment of anatomy and function. Neuroimage 2012; 62: 1311-1315
- 63 Beaulieu C. The basis of anisotropic water diffusion in the nervous system - a technical review. NMR Biomed 2002; 15: 435-455
- 64 Roosendaal SD, Geurts JJ, Vrenken H. et al. Regional DTI differences in multiple sclerosis patients. Neuroimage 2009; 44: 1397-1403
- 65 Eisele P, Szabo K, Griebe M. et al. Reduced diffusion in a subset of acute MS lesions – a serial multiparametric MRI study. AJNR Am J Neuroradiol 2012; 33: 1369-1373
- 66 Eisele P. et al. Cerebrospinal fluid pleocytosis in multiple sclerosis patients with lesions showing reduced diffusion. Mult Scler 2014; 20: 1391-1395
- 67 Brex PA, Gomez-Anson B, Parker GJ. et al. Proton MR spectroscopy in clinically isolated syndromes suggestive of multiple sclerosis. J Neurol Sci 1999; 166: 16-22
- 68 Fernando KT, McLean MA, Chard DT. et al. Elevated white matter myo-inositol in clinically isolated syndromes suggestive of multiple sclerosis. Brain 2004; 127: 1361-1369
- 69 Wattjes MP, Harzheim M, Lutterbey GG. et al. Prognostic value of high-field proton magnetic resonance spectroscopy in patients presenting with clinically isolated syndromes suggestive of multiple sclerosis. Neuroradiology 2008; 50: 123-129
- 70 Prinsen H, de Graaf RA, Mason GF. et al. Reproducibility measurement of glutathione, GABA, and glutamate: Towards in vivo neurochemical profiling of multiple sclerosis with MR spectroscopy at 7T. J Magn Reson Imaging 2017; 45: 187-198
- 71 Hattingen E, Jurcoane A, Nelles M. et al. Quantitative MR imaging of brain tissue and brain pathologies. Clin Neuroradiol 2015; 25 (Suppl. 02) 219-224
- 72 Freedman MS, Selchen D, Arnold DL. et al. Treatment optimization in MS: Canadian MS working group updated recommendations. Can J Neurol Sci 2013; 40: 307-323
- 73 Stangel M, Penner IK, Kallmann BA. et al. Towards the implementation of ‘no evidence of disease activity’ in multiple sclerosis treatment: the multiple sclerosis decision model. Ther Adv Neurol Disord 2015; 8: 3-13
- 74 Moraal B, Wattjes MP, Geurts JJ. et al. Improved detection of active multiple sclerosis lesions: 3D subtraction imaging. Radiology 2010; 255: 154-163
- 75 Battaglini M, Rossi F, Grove RA. et al. Automated identification of brain new lesions in multiple sclerosis using subtraction images. J Magn Reson Imaging 2014; 39: 1543-1549
- 76 Barkhof F, Calabresi PA, Miller DH. et al. Imaging outcomes for neuroprotection and repair in multiple sclerosis trials. Nat Rev Neurol 2009; 5: 256-266
- 77 De Stefano N, Airas L, Grigoriadis N. et al. Clinical relevance of brain volume measures in multiple sclerosis. CNS Drugs 2014; 28: 147-156
- 78 Popescu V, Agosta F, Hulst HE. et al. Brain atrophy and lesion load predict long term disability in multiple sclerosis. J Neurol Neurosurg Psychiatry 2013; 84: 1082-1091
- 79 Calabrese M, Rinaldi F, Mattisi I. et al. Widespread cortical thinning characterizes patients with MS with mild cognitive impairment. Neurology 2010; 74: 321-328
- 80 Vidal-Jordana A, Sastre-Garriga J, Pérez-Miralles F. et al. Early brain pseudoatrophy while on natalizumab therapy is due to white matter volume changes. Mult Scler 2013; 19: 1175-1181
- 81 De Stefano N, Arnold DL. Towards a better understanding of pseudoatrophy in the brain of multiple sclerosis patients. Mult Scler 2015; 21: 675-676
- 82 Absinta M, Sati P, Reich DS. Advanced MRI and staging of multiple sclerosis lesions. Nat Rev Neurol 2016; 12: 358-368
- 83 Mallik S, Samson RS, Wheeler-Kingshott CA. et al. Imaging outcomes for trials of remyelination in multiple sclerosis. J Neurol Neurosurg Psychiatry 2014; 85: 1396-1404
- 84 Healy BC, Glanz BI, Stankiewicz J. et al. A method for evaluating treatment switching criteria in multiple sclerosis. Mult Scler 2010; 16: 1483-1489
- 85 Río J, Castilló J, Rovira A. et al. Measures in the first year of therapy predict the response to interferon β in MS. Mult Scler 2009; 15: 848-853
- 86 Río J, Comabella M, Montalban X. Predicting responders to therapies for multiple sclerosis. Nat Rev Neurol 2009; 5: 553-560
- 87 Dhib-Jalbut S. Mechanisms of action of interferons and glatiramer acetate in multiple sclerosis. Neurology 2002; 58 (Suppl. 04) S3-S9
- 88 Visser F, Wattjes MP, Pouwels PJ. et al. Tumefactive multiple sclerosis lesions under fingolimod treatment. Neurology 2012; 79: 2000-2003
- 89 Pilz G, Harrer A, Wipfler P. et al. Tumefactive MS lesions under fingolimod: A case report and literature review. Neurology 2013; 81: 1654-1658
- 90 Maas RP, Muller-Hansma AH, Esselink RA. et al. Drug-associated progressive multifocal leukoencephalopathy: A clinical, radiological, and cerebrospinal fluid analysis of 326 cases. J Neurol 2016; 263: 2004-2021
- 91 Brew BJ, Davies NW, Cinque P. et al. Progressive multifocal leukoencephalopathy and other forms of JC virus disease. Nat Rev Neurol 2010; 6: 667-679
- 92 Warnke C, Wattjes MP, Adams O. et al. Progressive mutifokale Leukoencephalopathie. Nervenarzt 2016; 87: 1300-1304
- 93 D'Amico E, Zanghì A, Leone C. et al. Treatment-related progressive multifocal leukoencephalopathy in multiple sclerosis: A comprehensive review of current evidence and future needs. Drug Saf 2016; 39: 1163-1174
- 94 Yousry TA, Pelletier D, Cadavid D et al. Magnetic resonance imaging pattern in natalizumab-associated progressive multifocal leukoencephalopathy. Ann Neurol 2012; 72: 779–787
- 95 Yousry TA, Pelletier D, Cadavid D. et al. Magnetic resonance imaging pattern in natalizumab-associated progressive multifocal leukoencephalopathy. Ann Neurol 2012; 72: 779-787
- 96 Wattjes MP, Barkhof F. Diagnosis of natalizumab-associated progressive multifocal leukoencephalopathy using MRI. Curr Opin Neurol 2014; 27: 260-270
- 97 Wattjes MP, Vennegoor A, Steenwijk MD. et al. MRI pattern in asymptomatic natalizumab-associated PML. J Neurol Neurosurg Psychiatry 2015; 86: 793-798
- 98 Wattjes MP, Vennegoor A, Mostert J. et al. Diagnosis of asymptomatic natalizumab-associated PML: Are we between a rock and a hard place?. J Neurol 2014; 261: 1139-1143
- 0099 Dong-Si T, Richman S, Wattjes MP. et al. Outcome and survival of asymptomatic PML in natalizumab-treated MS patients. Ann Clin Transl Neurol 2014; 1: 755-764
- 100 McGuigan C, Craner M, Guadagno J. et al. Stratification and monitoring of natalizumab-associated progressive multifocal leukoencephalopathy risk: Recommendations from an expert group. J Neurol Neurosurg Psychiatry 2016; 87: 117-125
- 101 Wattjes MP, Wijburg MT, Vennegoor A et al. Diagnostic performance of brain MRI in pharmacovigilance of natalizumab-treated MS patients. Mult Scler 2016; 22: 1174–1183
- 102 Wattjes MP, Wijburg MT, Vennegoor A. et al. Diagnostic performance of brain MRI in pharmacovigilance of natalizumab-treated MS patients. Mult Scler 2016; 22: 1174-1183
- 103 Wijburg MT, Witte BI, Vennegoor A. et al. MR imaging criteria differentiating asymptomatic PML from new MS lesions during natalizumab pharmacovigilance. J Neurol Neurosurg Psychiatry 2016; 87: 1138-1145
- 104 Warnke C, von Geldern G, Markwerth P. et al. Cerebrospinal fluid JC virus antibody index for diagnosis of natalizumab-associated progressive multifocal leukoencephalopathy. Ann Neurol 2014; 76: 792-801
- 105 Warnke C, Wijburg MT, Hartung HP. et al. Application of the CSF JCV antibody index to early natalizumab-associated progressive multifocal leukoencephalopathy. J Neurol Neurosurg Psychiatry 2017; pii: jnnp-2016-315298
- 106 Arvin AM, Wolinsky JS, Kappos L. et al. Varicella-zoster virus infections in patients treated with fingolimod: Risk assessment and consensus recommendations for management. JAMA Neurol 2015; 72: 31-39
- 107 Gundacker ND, Jordan SJ, Jones BA. et al. Acute cryptococcal immune reconstitution inflammatory syndrome in a patient on natalizumab. Open Forum Infect Dis 2016; 3: ofw038 10.1093/ofid/ofw038
Correspondence
-
References
- 1 Compston A, Coles A. Multiple sclerosis. Lancet 2008; 372: 1502-1517
- 2 Wattjes MP, Steenwijk MD, Stangel M. MRI in the Diagnosis and Monitoring of Multiple Sclerosis: An Update. Clin Neuroradiol 2015; 25 (Suppl. 02) 157-165
- 3 Igra MS, Paling D, Wattjes MP. et al. Multiple sclerosis update: Use of MRI for early diagnosis, disease monitoring and assessment of treatment related complications. Br J Radiol 2017; 90: 20160721 10.1259/bjr.20160721
- 4 Polman CH, Reingold SC, Banwell B. et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol 2011; 69: 292-302
- 5 Valdueza JM, Doepp F, Schreiber SJ. et al. What went wrong? The flawed concept of cerebrospinal venous insufficiency. J Cereb Blood Flow Metab 2013; 33: 657-668
- 6 Tintore M, Rovira À, Río J. et al. Defining high, medium and low impact prognostic factors for developing multiple sclerosis. Brain 2015; 138: 1863-1874
- 7 Fisniku LK, Brex PA, Altmann DR. et al. Disability and T2 MRI lesions: a 20-year follow-up of patients with relapse onset of multiple sclerosis. Brain 2008; 131808-131817
- 8 Rovira A, Wattjes MP, Tintoré M. et al. Evidence-based guidelines: MAGNIMS consensus guidelines on the use of MRI in multiple sclerosis-clinical implementation in the diagnostic process. Nat Rev Neurol 2015; 11: 471-482
- 9 Wattjes MP, Rovira A, Miller D. et al. Evidence-based guidelines: MAGNIMS consensus guidelines on the use of MRI in multiple sclerosis--establishing disease prognosis and monitoring patients. Nat Rev Neurol 2015; 11: 597-606
- 10 Traboulsee A, Simon JH, Stone L. et al. Revised recommendations of the consortium of ms centers task force for a standardized mri protocol and clinical guidelines for the diagnosis and follow-up of multiple sclerosis. AJNR Am J Neuroradiol 2016; 37: 394-401
- 11 Kieseier BC, Wiendl H, Hartung HP. et al. Risks and benefits of multiple sclerosis therapies: Need for continual assessment?. Curr Opin Neurol 2011; 24: 238-243
- 12 Dubey D, Cano CA, Stüve O. Update on monitoring and adverse effects of first generation disease modifying therapies and their recently approved versions in relapsing forms of multiple sclerosis. Curr Opin Neurol 2016; 29: 272-277
- 13 Dubey D, Cano CA, Stüve O. Update on monitoring and adverse effects of approved second-generation disease-modifying therapies in relapsing forms of multiple sclerosis. Curr Opin Neurol 2016; 29: 278-285
- 14 Winkelmann A, Loebermann M, Reisinger EC. et al. Disease-modifying therapies and infectious risks in multiple sclerosis. Nat Rev Neurol 2016; 12: 217-233
- 15 Sethi V, Yousry TA, Muhlert N. et al. Improved detection of cortical MS lesions with phase-sensitive inversion recovery MRI. J Neurol Neurosurg Psychiatry 2012; 83: 877-882
- 16 Wattjes MP, Lutterbey GG, Gieseke J. et al. Double inversion recovery brain imaging at 3T: Diagnostic value in the detection of multiple sclerosis lesions. AJNR Am J Neuroradiol 2007; 28: 54-59
- 17 Kilsdonk ID, de Graaf WL, Barkhof F. et al. Inflammation high-field magnetic resonance imaging. Neuroimaging Clin N Am 2012; 22: 135-157
- 18 Wattjes MP, Barkhof F. High field MRI in the diagnosis of multiple sclerosis: High field-high yield?. Neuroradiology 2009; 51: 279-292
- 19 Filippi M, Evangelou N, Kangarlu A. et al. Ultra-high-field MR imaging in multiple sclerosis. J Neurol Neurosurg Psychiatry 2014; 85: 60-66
- 20 Wattjes MP, Harzheim M, Lutterbey GG. et al. High field MR imaging and 1H-MR spectroscopy in clinically isolated syndromes suggestive of multiple sclerosis: Correlation between metabolic alterations and diagnostic MR imaging criteria. J Neurol 2008; 255: 56-63
- 21 Enzinger C, Barkhof F, Ciccarelli O. et al. Nonconventional MRI and microstructural cerebral changes in multiple sclerosis. Nat Rev Neurol 2015; 11: 676-686
- 22 Geurts JJ, Calabrese M, Fisher E. et al. Measurement and clinical effect of grey matter pathology in multiple sclerosis. Lancet Neurol 2012; 11: 1082-1092
- 23 Vigeveno RM, Wiebenga OT, Wattjes MP. et al. Shifting imaging targets in multiple sclerosis: From inflammation to neurodegeneration. J Magn Reson Imaging 2012; 36: 1-19
- 24 Wattjes MP, Harzheim M, Lutterbey GG. et al. Axonal damage but no increased glial cell activity in the normal-appearing white matter of patients with clinically isolated syndromes suggestive of multiple sclerosis using high-field magnetic resonance spectroscopy. AJNR Am J Neuroradiol 2007; 28: 1517-1522
- 25 Pardini M, Sudre CH, Prados F. et al. Relationship of grey and white matter abnormalities with distance from the surface of the brain in multiple sclerosis. J Neurol Neurosurg Psychiatry 2016; 87: 1212-1217
- 26 Wattjes MP, Harzheim M, Lutterbey GG. et al. Does high field MRI allow an earlier diagnosis of multiple sclerosis?. J Neurol 2008; 255: 1159-1163
- 27 Filippi M, Rocca MA, Gasperini C. et al. Interscanner variation in brain MR lesion load measurements in multiple sclerosis using conventional spin-echo, rapid relaxation-enhanced, and fast-FLAIR sequences.. AJNR Am J Neuroradiol 1999; 20: 133-137
- 28 Wattjes MP, Lutterbey GG, Harzheim M. et al. Imaging of inflammatory lesions at 3.0 Tesla in patients with clinically isolated syndromes suggestive of multiple sclerosis: A comparison of fluid-attenuated inversion recovery with T2 turbo spin-echo. Eur Radiol 2006; 16: 1494-1500
- 29 Vågberg M, Axelsson M, Birgander R. et al. Guidelines for the use of magnetic resonance imaging in diagnosing and monitoring the treatment of multiple sclerosis: Recommendations of the Swedish Multiple Sclerosis Association and the Swedish Neuroradiological Society. Acta Neurol Scand 2017; 135: 17-24
- 30 Petzold A, Wattjes MP, Costello F. et al. The investigation of acute optic neuritis: a review and proposed protocol. Nat Rev Neurol 2014; 10: 447-458
- 31 Simon B, Schmidt S, Lukas C. et al. Improved in vivo detection of cortical lesions in multiple sclerosis using double inversion recovery MR imaging at 3T. Eur Radiol 2010; 20: 1675-1683
- 32 Moraal B, Roosendaal SD, Pouwels PJ. et al. Multi-contrast, isotropic, single-slab 3D MR imaging in multiple sclerosis. Eur Radiol 2008; 18: 2311-2320
- 33 Barkhof F, Pouwels PJ, Wattjes MP. The holy grail in diagnostic neuroradiology: 3T or 3D?. Eur Radiol 2011; 21: 449-456
- 34 Moraal B, Wattjes MP, Geurts JJ. et al. Improved detection of active multiple sclerosis lesions: 3D subtraction imaging. Radiology 2010; 255: 154-163
- 35 Schmidt P, Gaser C, Arsic M. et al. An automated tool for detection of FLAIR-hyperintense white-matter lesions in multiple sclerosis. Neuroimage 2012; 59: 3774-3783
- 36 Lukas C, Gold R, Fiehler J. et al Ablagerung von gadoliniumhaltigen Kontrastmitteln im Gehirn nach mehrfacher Anwendung: Konsequenzen für den Einsatz der MRT bei Diagnosestellung und Verlaufsbeurteilung der Multiplen Sklerose?. Akt Neurol 2016; 43: 522-523
- 37 Gass A, Rocca MA, Agosta A. et al. MRI monitoring of pathological changes in the spinal cord in patients with multiple sclerosis. Lancet Neurol 2015; 14: 443-454
- 38 Stankiewicz JM, Neema M, Alsop DC. et al. Spinal cord lesions and clinical status in multiple sclerosis: A 1.5T and 3T MRI study. J Neurol Sci 2009; 279: 99-105
- 39 Bot JC, Barkhof F. Spinal-cord MRI in multiple sclerosis: Conventional and nonconventional MR techniques. Neuroimaging Clin N Am 2009; 19: 81-99
- 40 Filippi M, Rocca MA, Ciccarelli O. et al. MRI criteria for the diagnosis of multiple sclerosis: MAGNIMS consensus guidelines. Lancet Neurol 2016; 15: 292-303
- 41 Dekker I, Wattjes MP. Brain and spinal cord MR imaging features in multiple sclerosis and variants. Neuroimag Clin N Am 2017; 27: 205-227
- 42 Wallner-Blazek M, Rovira A, Fillipp M. et al. Atypical idiopathic inflammatory demyelinating lesions: Prognostic implications and relation to multiple sclerosis. J Neurol 2013; 260: 2016-2022
- 43 Charil A, Yousry TA, Rovaris M. et al. MRI and the diagnosis of multiple sclerosis: Expanding the concept of "no better explanation". Lancet Neurol 2006; 5: 841-852
- 44 Bot JC, Barkhof F, Lycklama à Nijeholt G. et al. Differentiation of multiple sclerosis from other inflammatory disorders and cerebrovascular disease: value of spinal MR imaging. Radiology 2002; 223: 46-56
- 45 Kilsdonk ID, Wattjes MP, Lopez-Soriano A. et al. Improved differentiation between MS and vascular brain lesions using FLAIR* at 7 Tesla. Eur Radiol 2014; 24: 841-849
- 46 Sinnecker T, Dörr J, Pfueller CF. et al. Distinct lesion morphology at 7-T MRI differentiates neuromyelitis optica from multiple sclerosis. Neurology 2012; 79: 708-714
- 47 Kilsdonk ID, Lopez-Soriano A, Kuijer JP. et al. Morphological features of MS lesions on FLAIR* at 7T and their relation to patient characteristics. J Neurol 2014; 261: 1356-1364
- 48 Wuerfel J, Sinnecker T, Ringelstein EB. et al. Lesion morphology at 7 Tesla MRI differentiates Susac syndrome from multiple sclerosis. Mult Scler 2012; 18: 1592-1599
- 49 Sati P, Oh J, Constable RT. et al. The central vein sign and its clinical evaluation for the diagnosis of multiple sclerosis: A consensus statement from the North American Imaging in Multiple Sclerosis Cooperative. Nat Rev Neurol 2016; 12: 714-722
- 50 de Graaf WL, Zwanenburg JJ, Visser F. et al. Lesion detection at seven Tesla in multiple sclerosis using magnetisation prepared 3D-FLAIR and 3D-DIR. Eur Radiol 2012; 22: 221-231
- 51 Kilsdonk ID, Jonkman LE, Klaver R. et al. Increased cortical grey matter lesion detection in multiple sclerosis with 7 T MRI: A post-mortem verification study. Brain 2016; 139: 1472-1481
- 52 Zurawski J, Lassmann H, Bakshi R. Use of magnetic resonance imaging to visualize leptomeningeal inflammation in patients with multiple sclerosis: A review. JAMA Neurol 2017; 74: 100-109
- 53 Kilsdonk ID, Schoonheim M, Wattjes MP. In-vivo imaging of meningeal inflammation in multiple sclerosis: Presence of evidence or evidence of presence?. Mult Scler 2017; 23: 1169-1171
- 54 Giorgio A, De Stefano N. Advanced structural and functional brain MRI in multiple sclerosis. Semin Neurol 2016; 36: 163-176
- 55 Henkelman RM, Huang X, Xiang QS. et al. Quantitative interpretation of magnetization transfer. Magn Reson Med 1993; 29: 759-766
- 56 Brown RA, Narayanan S, Arnold DL. Imaging of repeated episodes of demyelination and remyelination in multiple sclerosis. Neuroimage Clin 2014; 6: 20-25
- 57 Schwartzbach CJ, Grove RA, Brown R. et al. Lesion remyelinating activity of GSK239512 versus placebo in patients with relapsing-remitting multiple sclerosis: A randomised, single-blind, phase II study. J Neurol 2017; 264: 304-315
- 58 Lema A, Bishop C, Malik O. et al. A Comparison of magnetization transfer methods to assess brain and cervical cord microstructure in multiple sclerosis. J Neuroimaging 2017; 27: 221-226
- 59 Ropele S, de Graaf W, Khalil M. et al. MRI assessment of iron deposition in multiple sclerosis. J Magn Reson Imaging 2011; 34: 13-21
- 60 Ropele S, Kilsdonk ID, Wattjes MP. et al. Determinants of iron accumulation in deep grey matter of multiple sclerosis patients. Mult Scler 2014; 20: 1692-1698
- 61 Zhang Y, Gauthier SA, Gupta A. et al. Longitudinal change in magnetic susceptibility of new enhanced multiple sclerosis (MS) lesions measured on serial quantitative susceptibility mapping (QSM). J Magn Reson Imaging 2016; 44: 426-432
- 62 Reichenbach JR. The future of susceptibility contrast for assessment of anatomy and function. Neuroimage 2012; 62: 1311-1315
- 63 Beaulieu C. The basis of anisotropic water diffusion in the nervous system - a technical review. NMR Biomed 2002; 15: 435-455
- 64 Roosendaal SD, Geurts JJ, Vrenken H. et al. Regional DTI differences in multiple sclerosis patients. Neuroimage 2009; 44: 1397-1403
- 65 Eisele P, Szabo K, Griebe M. et al. Reduced diffusion in a subset of acute MS lesions – a serial multiparametric MRI study. AJNR Am J Neuroradiol 2012; 33: 1369-1373
- 66 Eisele P. et al. Cerebrospinal fluid pleocytosis in multiple sclerosis patients with lesions showing reduced diffusion. Mult Scler 2014; 20: 1391-1395
- 67 Brex PA, Gomez-Anson B, Parker GJ. et al. Proton MR spectroscopy in clinically isolated syndromes suggestive of multiple sclerosis. J Neurol Sci 1999; 166: 16-22
- 68 Fernando KT, McLean MA, Chard DT. et al. Elevated white matter myo-inositol in clinically isolated syndromes suggestive of multiple sclerosis. Brain 2004; 127: 1361-1369
- 69 Wattjes MP, Harzheim M, Lutterbey GG. et al. Prognostic value of high-field proton magnetic resonance spectroscopy in patients presenting with clinically isolated syndromes suggestive of multiple sclerosis. Neuroradiology 2008; 50: 123-129
- 70 Prinsen H, de Graaf RA, Mason GF. et al. Reproducibility measurement of glutathione, GABA, and glutamate: Towards in vivo neurochemical profiling of multiple sclerosis with MR spectroscopy at 7T. J Magn Reson Imaging 2017; 45: 187-198
- 71 Hattingen E, Jurcoane A, Nelles M. et al. Quantitative MR imaging of brain tissue and brain pathologies. Clin Neuroradiol 2015; 25 (Suppl. 02) 219-224
- 72 Freedman MS, Selchen D, Arnold DL. et al. Treatment optimization in MS: Canadian MS working group updated recommendations. Can J Neurol Sci 2013; 40: 307-323
- 73 Stangel M, Penner IK, Kallmann BA. et al. Towards the implementation of ‘no evidence of disease activity’ in multiple sclerosis treatment: the multiple sclerosis decision model. Ther Adv Neurol Disord 2015; 8: 3-13
- 74 Moraal B, Wattjes MP, Geurts JJ. et al. Improved detection of active multiple sclerosis lesions: 3D subtraction imaging. Radiology 2010; 255: 154-163
- 75 Battaglini M, Rossi F, Grove RA. et al. Automated identification of brain new lesions in multiple sclerosis using subtraction images. J Magn Reson Imaging 2014; 39: 1543-1549
- 76 Barkhof F, Calabresi PA, Miller DH. et al. Imaging outcomes for neuroprotection and repair in multiple sclerosis trials. Nat Rev Neurol 2009; 5: 256-266
- 77 De Stefano N, Airas L, Grigoriadis N. et al. Clinical relevance of brain volume measures in multiple sclerosis. CNS Drugs 2014; 28: 147-156
- 78 Popescu V, Agosta F, Hulst HE. et al. Brain atrophy and lesion load predict long term disability in multiple sclerosis. J Neurol Neurosurg Psychiatry 2013; 84: 1082-1091
- 79 Calabrese M, Rinaldi F, Mattisi I. et al. Widespread cortical thinning characterizes patients with MS with mild cognitive impairment. Neurology 2010; 74: 321-328
- 80 Vidal-Jordana A, Sastre-Garriga J, Pérez-Miralles F. et al. Early brain pseudoatrophy while on natalizumab therapy is due to white matter volume changes. Mult Scler 2013; 19: 1175-1181
- 81 De Stefano N, Arnold DL. Towards a better understanding of pseudoatrophy in the brain of multiple sclerosis patients. Mult Scler 2015; 21: 675-676
- 82 Absinta M, Sati P, Reich DS. Advanced MRI and staging of multiple sclerosis lesions. Nat Rev Neurol 2016; 12: 358-368
- 83 Mallik S, Samson RS, Wheeler-Kingshott CA. et al. Imaging outcomes for trials of remyelination in multiple sclerosis. J Neurol Neurosurg Psychiatry 2014; 85: 1396-1404
- 84 Healy BC, Glanz BI, Stankiewicz J. et al. A method for evaluating treatment switching criteria in multiple sclerosis. Mult Scler 2010; 16: 1483-1489
- 85 Río J, Castilló J, Rovira A. et al. Measures in the first year of therapy predict the response to interferon β in MS. Mult Scler 2009; 15: 848-853
- 86 Río J, Comabella M, Montalban X. Predicting responders to therapies for multiple sclerosis. Nat Rev Neurol 2009; 5: 553-560
- 87 Dhib-Jalbut S. Mechanisms of action of interferons and glatiramer acetate in multiple sclerosis. Neurology 2002; 58 (Suppl. 04) S3-S9
- 88 Visser F, Wattjes MP, Pouwels PJ. et al. Tumefactive multiple sclerosis lesions under fingolimod treatment. Neurology 2012; 79: 2000-2003
- 89 Pilz G, Harrer A, Wipfler P. et al. Tumefactive MS lesions under fingolimod: A case report and literature review. Neurology 2013; 81: 1654-1658
- 90 Maas RP, Muller-Hansma AH, Esselink RA. et al. Drug-associated progressive multifocal leukoencephalopathy: A clinical, radiological, and cerebrospinal fluid analysis of 326 cases. J Neurol 2016; 263: 2004-2021
- 91 Brew BJ, Davies NW, Cinque P. et al. Progressive multifocal leukoencephalopathy and other forms of JC virus disease. Nat Rev Neurol 2010; 6: 667-679
- 92 Warnke C, Wattjes MP, Adams O. et al. Progressive mutifokale Leukoencephalopathie. Nervenarzt 2016; 87: 1300-1304
- 93 D'Amico E, Zanghì A, Leone C. et al. Treatment-related progressive multifocal leukoencephalopathy in multiple sclerosis: A comprehensive review of current evidence and future needs. Drug Saf 2016; 39: 1163-1174
- 94 Yousry TA, Pelletier D, Cadavid D et al. Magnetic resonance imaging pattern in natalizumab-associated progressive multifocal leukoencephalopathy. Ann Neurol 2012; 72: 779–787
- 95 Yousry TA, Pelletier D, Cadavid D. et al. Magnetic resonance imaging pattern in natalizumab-associated progressive multifocal leukoencephalopathy. Ann Neurol 2012; 72: 779-787
- 96 Wattjes MP, Barkhof F. Diagnosis of natalizumab-associated progressive multifocal leukoencephalopathy using MRI. Curr Opin Neurol 2014; 27: 260-270
- 97 Wattjes MP, Vennegoor A, Steenwijk MD. et al. MRI pattern in asymptomatic natalizumab-associated PML. J Neurol Neurosurg Psychiatry 2015; 86: 793-798
- 98 Wattjes MP, Vennegoor A, Mostert J. et al. Diagnosis of asymptomatic natalizumab-associated PML: Are we between a rock and a hard place?. J Neurol 2014; 261: 1139-1143
- 0099 Dong-Si T, Richman S, Wattjes MP. et al. Outcome and survival of asymptomatic PML in natalizumab-treated MS patients. Ann Clin Transl Neurol 2014; 1: 755-764
- 100 McGuigan C, Craner M, Guadagno J. et al. Stratification and monitoring of natalizumab-associated progressive multifocal leukoencephalopathy risk: Recommendations from an expert group. J Neurol Neurosurg Psychiatry 2016; 87: 117-125
- 101 Wattjes MP, Wijburg MT, Vennegoor A et al. Diagnostic performance of brain MRI in pharmacovigilance of natalizumab-treated MS patients. Mult Scler 2016; 22: 1174–1183
- 102 Wattjes MP, Wijburg MT, Vennegoor A. et al. Diagnostic performance of brain MRI in pharmacovigilance of natalizumab-treated MS patients. Mult Scler 2016; 22: 1174-1183
- 103 Wijburg MT, Witte BI, Vennegoor A. et al. MR imaging criteria differentiating asymptomatic PML from new MS lesions during natalizumab pharmacovigilance. J Neurol Neurosurg Psychiatry 2016; 87: 1138-1145
- 104 Warnke C, von Geldern G, Markwerth P. et al. Cerebrospinal fluid JC virus antibody index for diagnosis of natalizumab-associated progressive multifocal leukoencephalopathy. Ann Neurol 2014; 76: 792-801
- 105 Warnke C, Wijburg MT, Hartung HP. et al. Application of the CSF JCV antibody index to early natalizumab-associated progressive multifocal leukoencephalopathy. J Neurol Neurosurg Psychiatry 2017; pii: jnnp-2016-315298
- 106 Arvin AM, Wolinsky JS, Kappos L. et al. Varicella-zoster virus infections in patients treated with fingolimod: Risk assessment and consensus recommendations for management. JAMA Neurol 2015; 72: 31-39
- 107 Gundacker ND, Jordan SJ, Jones BA. et al. Acute cryptococcal immune reconstitution inflammatory syndrome in a patient on natalizumab. Open Forum Infect Dis 2016; 3: ofw038 10.1093/ofid/ofw038