

Subscribe to RSS
DOI: 10.1055/s-0043-1764402
Imaging Features of Rare Hepatic Tumors
Authors


Abstract
Hepatic lesions are commonly encountered in radiology practice. Lesions with classic imaging findings such as hepatocellular carcinoma, cholangiocarcinoma, hemangiomas, focal nodular hyperplasia, and adenomas are well described in literature and easily diagnosed by most experienced radiologists. In the appropriate context, metastases, which are one of the most common lesions encountered by radiologists who practice in predominantly cancer care settings, are also easily diagnosed. However, one may encounter rarer neoplasms which may be challenging to diagnose and manage. Often, these lesions have overlapping imaging features with those of the common lesions mentioned above. Diagnosis of these rarer tumors would require not only interpreting the images in the context of patient's demographics and clinical presentation but also recognizing the unique imaging features of these tumors. The literature is sparse in describing the radiological appearances of these tumors. Diagnosis based solely on imaging criteria is not advised in these instances. Histological confirmation or other prudent follow-up strategies are necessary for confirmation of imaging findings and interpretation. In this article, we will describe known imaging features of a few rarer primary malignant and benign neoplasms in the liver.
Foremost among the worrisome lesions are malignant neoplasms, both epithelial and mesenchymal in origin. Hepatoblastoma, angiosarcomas, epithelioid hemangioendothelioma, perivascular epithelioid cell tumors (PEComas), mucinous cystic neoplasms (MCNs), intraductal papillary mucinous neoplasm (IPMN), and primary hepatic lymphoma are some of the malignant lesions described in this article. Imaging appearances of other benign lesions such as biliary hamartomas and inflammatory pseudotumors are also discussed.
Hepatoblastoma
Hepatoblastoma, although rare, is the most common primary malignant hepatic neoplasm in children, comprising two-thirds of primary liver tumors in this population.[1] However, the incidence of hepatoblastoma has been increasing worldwide.[2] Most cases occur in children less than 5 years old. Adult cases are very rare with fewer than 70 adult cases reported in the literature.
Hepatoblastoma is more common in children born prematurely. It is almost never associated with chronic liver disease. Most cases are sporadic. However, there is an increased incidence in patients with certain genetic abnormalities such as Beckwith-Wiedemann syndrome, trisomy 18, trisomy 21, Li-Fraumeni syndrome, type 1a glycogen storage disease (von Gierke disease), and familial adenomatous polyposis. Screening for hepatoblastoma is considered in such individuals. A recommended strategy is abdominal ultrasound (US) and alpha fetoprotein (AFP) levels every 3 months until 6 to 8 years of age.[3]
Most patients are asymptomatic. Many patients present with an abdominal mass and a diagnosis suspected by imaging and subsequently confirmed by biopsy. Occasionally, nonspecific symptoms such as pain, nausea, and vomiting are seen. Large tumors may present after rupture with acute abdominal pain and intra-abdominal hemorrhage. Serum AFP is usually elevated. Very rarely, patients may also present with sexual precocity due to synthesis of ectopic β-human chorionic gonadotropin.[4] Rarely, ectopic production of adrenocortical hormones and/or ectopic production of parathyroid hormone may lead to Cushing syndrome and hypercalcemia, respectively.[5]
Hepatoblastomas are embryonal tumors that develop from pluripotent cells with the potential to differentiate along several lines. Hence, histologically, it is a complex tumor that may include fetal or embryonal hepatocytes and heterogeneous tissues including cartilage, muscle fibers, squamous epithelium, and bone. Consequently, the imaging features are varied and depend on the histological makeup of the tumors. The most common site of metastasis is the lung, while lymph node involvement is rare.[6]
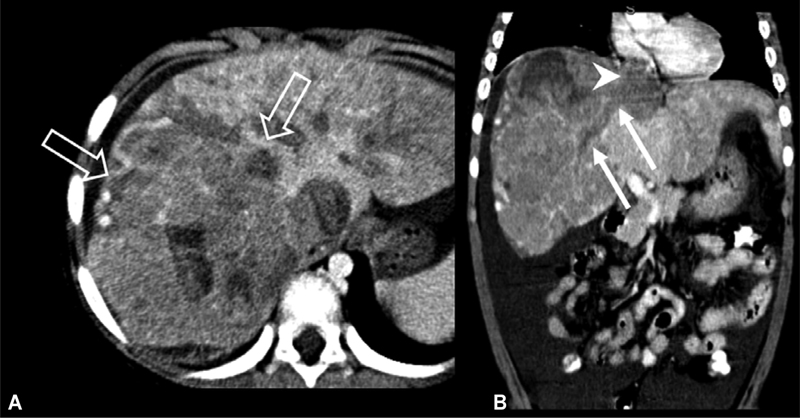
On plain radiographs, hepatomegaly may be recognized in patients with large tumors. Occasionally, these tumors also show specks of calcification on radiographs. US is usually the first imaging study performed in children and hence the most common modality in which the diagnosis of hepatoblastoma is first suggested. These masses are usually large solitary masses of varying echogenicity ([Fig. 1]). Occasionally, they are multifocal, sometimes with smaller satellite lesions. Areas of necrosis and hemorrhage are common. Rarely, hepatoblastomas may infiltrate the entire liver and present as diffusely enlarged liver with heterogeneous and inhomogeneous echotexture. Further evaluation with cross-sectional imaging such as computed tomography (CT), magnetic resonance imaging (MRI), and histological confirmation with liver biopsy is necessary.[7]

Calcifications may be seen on CT scans, particularly in tumors which have mixed mesenchymal elements. Hepatoblastomas show heterogeneous pattern of enhancement, generally hypoenhancing compared with normal liver. Tumor thrombus in portal and hepatic veins are common.
MRI is usually the preferred modality by most pediatric radiologists due to lack of radiation. However, MRI does pose challenges, often requiring sedation and general anesthesia in the pediatric population. Depending on the histologic makeup of the tumor, the tumors are either homogeneous or heterogeneous with varying amounts of hemorrhage, fibrosis, and septae ([Fig. 2]). Septations appear on MRI as hypointense band both on T1- and T2-weighted images. Hepatoblastomas have imaging features similar to those of fibrolamellar carcinoma which should be considered in the differential. The latter condition usually occurs in young adults and teenagers.

Imaging plays a key role in diagnosis and staging of hepatoblastomas. The PRETEXT (PRE-Treatment EXTent of tumor) system is used for risk stratification.[8] In the PRETEXT system, the extent of liver disease is based on the number of sectors of liver involved by the tumor. Annotation is a part of pretext staging to help guide surgical approach which includes assessment of involvement of hepatic veins, vena cava ([Fig. 3]), portal veins, extrahepatic extension, caudate lobe involvement, multiplicity, tumor rupture, and distant metastases. MR angiography is commonly performed to help in planning surgical approach. For patients whose tumor is not resectable at diagnosis, repeat radiologic evaluation after initial chemotherapy is termed POSTTEXT and uses the same criteria as PRETEXT. Assessment of downstaging and timing of resection is assessed on posttreatment cases as well as suitability for liver transplantation or other form of targeted treatment.[9]
The 5-year survival of hepatoblastoma has dramatically increased from 30% reported in the 1980s to approximately 75 to 90% reported in contemporary studies reflecting improvements in pretreatment staging, chemotherapy, surgical techniques, and introduction of liver transplantation for unresectable disease.[2]
Angiosarcoma
Angiosarcomas account for less than 1% of all primary liver tumors.[10] However, it is the most common primary hepatic sarcoma. It almost always portends a poor prognosis. The majority of the untreated patients die within 6 months and most patients die within a year after surgical resection.[11] Angiosarcomas have received attention in recent decades because of its frequent association with several environmental carcinogens such as Thorotrast, vinyl chloride, arsenic compounds, and radiation.[12] Both hemochromatosis and anabolic steroids have been associated with hepatic angiosarcoma. It usually presents in older patients more than 50 years old and is more common in men. Patients often present with abdominal pain, ascites, weight loss, fatigue, jaundice, and occasionally Budd–Chiari syndrome. Thrombocytopenia and hepatomegaly are common in these patients. Metastatic disease is also frequent and is seen in the spleen, lymph nodes, lungs, bones, and adrenal glands.[13] Liver failure and intra-abdominal bleeding are common causes of death.
Hepatic angiosarcomas are primarily composed of vascular or lymphatic endothelial cells and are characterized by abundant blood vessels. Hemorrhage can occur spontaneously. Angiosarcomas form numerous poorly defined variable sized nodules. The entire liver is frequently involved. Better differentiated areas may show large, cavernous spaces lined by atypical endothelial cells. Tumor cells grow along and into the sinusoids and branches of the portal and hepatic veins.[14] These histologic features determine imaging appearances seen on CT and MRI. Although biopsy is commonly utilized to diagnose angiosarcoma, a relatively frequent complication is postbiopsy hemorrhage.
The lesions are generally ill defined, multifocal, and show heterogeneous areas including areas of hemorrhage. On MRI, these lesions may be of mixed signal on precontrast T1- and T2-weighted images particularly due to hemorrhage ([Fig. 4A]). Larger dominant masses demonstrate heterogeneous internal architecture. Nonenhanced CT images can show areas of hemorrhage. On postcontrast studies, enhancing regions show progressive enhancement on portal and delayed phase imaging ([Figs. 4] and [5]).[15] Lack of washout helps in differentiating angiosarcoma from multifocal hepatocellular carcinoma (HCC) in patients with cirrhosis.


Epithelioid Hemangioendothelioma
Epithelioid hemangioendothelioma is a low-grade malignant vascular neoplasm affecting middle-aged patients with a slight female preponderance.[16] [17] Patients often present with nonspecific symptoms including abdominal pain, weight loss, or malaise. Despite being a low-grade tumor, there is a high rate of regional and distant metastases. Histologically, these lesions may be diagnosed as cholangiocarcinoma due to significant overlapping features. Accurate diagnosis may require staining for markers of endothelial cells such as ERG transcription factor, factor VIII-related antigen, and CD 31/34 antigens, which are usually negative in cholangiocarcinoma.[14] Recognition of classic radiologic findings may also be useful in providing accurate diagnosis.
These lesions tend to be multifocal, predominantly peripheral in distribution sometimes coalescing into individual nodules. Occasionally these lesions calcify.[18] Subcapsular lesions usually produce hepatic capsular retraction ([Fig. 6]).[19] On US, the lesions are predominantly hypoechoic or with mixed echotexture.

On MRI, the lesions are usually well-demarcated, hyperintense on T2-weighted sequences. Occasionally, a two-layer halo is described with alternating bands of hypo- and hyperintense signals on T2-weighted images (target sign). The lesions are hypointense on noncontrast T1-weighted sequences. They are hypoenhancing on postcontrast studies sometimes with a ring peripheral enhancement or target pattern of enhancement. Coexistence of the “target sign” on both postcontrast and T2-weighted sequences are considered highly specific for epithelioid hemangioendothelioma ([Fig. 7]). Progressive enhancement and lack of washout is common. Some lesions show minimal or no enhancement on postcontrast studies. Another sign which has been considered specific for epithelioid hemangioendothelioma is the lollipop sign, which consists of a contrast-enhanced vessel ending in a hypoattenuating or hypointense lesion resembling a lollipop.[20] CT enhancement patterns are very similar to that seen on MRI.

Hepatic Perivascular Epithelioid Cell Tumor
PEComas represent a group of neoplasms that show both smooth muscle and melanocytic differentiation.[21] PEComas can show a range of biological behavior ranging from benign tumors to aggressive sarcomas. They can arise in any anatomical site. For example, in the lungs, lymphangioleiomyoma/lymphangioleiomyomatosis and cell sugar tumor of the lung belong to this group of tumors. In the kidneys, angiomyolipoma belong to this group of tumors.[22] PEComas arising in the kidney and liver are commonly composed of epithelioid or spindle cells, mature fat, and thick-walled vessels. Hepatic PEComas are very rare.
Due to its rarity, the natural history of this condition has not been elucidated. However, it has been noted that the lesion is found mainly in females. Clinical presentation is usually with nonspecific abdominal pain. However, most are incidentally diagnosed on imaging for other indications.[23] [24] [25] Tuberous sclerosis is associated with approximately 5 to 15% of hepatic PEComas.
Presence of macroscopic fat in a tumor should alert the radiologist to this condition ([Fig. 8]). However, this is not very specific as some HCC may contain fat. On US, these lesions tend to be expansile masses which are hypoechoic. On CT and MRI, the lesions tend to be large masses and show arterial hyperenhancement. There may or may not be washout on the delayed phase images ([Figs. 9] and [10]). Although most of these tumors are benign, a few of these lesions are malignant and can metastasize ([Fig. 10]).[23] The imaging features can overlap with those of other more common conditions such as focal nodular hyperplasia as shown in the example in [Fig. 9], a HCC as shown in the example in [Fig. 10], or a hemangioma. Biopsy is generally required for diagnosis. Radiologists should be alert to any atypical findings such as normal background liver, macroscopic fat, and enhancement and washout characteristics which do not conform to well-known classic features.



Hepatic Mucinous Cystic Neoplasms
Hepatic MCNs were previously referred to as biliary cystadenomas. These are rare cystic tumors that occur within the liver parenchyma, or less frequently, in the extrahepatic bile ducts. The tumors grow to a large size and require surgical intervention in most cases. MCNs occur in adults and more often in women. These lesions are characterized by presence of ovarian stroma. They are rare, accounting for less than 5% of cystic hepatic masses.[26] [27]
While most MCNs arise from the intrahepatic biliary system, up to 10% of these lesions are extrahepatic in location.[27] [28] On ultrasonography, an MCN is seen as a cystic lesion with thickened and irregular walls with wall nodularity. Internal debris due to hemorrhage or secretions is common.[29] On a CT and MRI scans, these lesions are complex unilocular or multilocular cystic mass with septations. There may be variable amounts of nodular and solid enhancing intracystic components. These lesions may also cause biliary dilatation by causing extrinsic compression.[27] MRI characterizes cyst fluid content by varying signal intensities on T1-weighted images depending on cyst fluid protein content.[30] The cyst wall is usually thickened and nodular. Presence of low-grade metabolic activity on positron emission tomography (PET-CT) may be seen in MCN and does not necessarily suggest malignant degeneration ([Fig. 11]).

The preferred treatment for noninvasive MCNs is resection since malignant transformation is seen in up to 15% of patients.[29] [31] Formal surgical resection with negative margins is recommended. Extrahepatic MCNs ([Fig. 12]) are resected along with the associated bile duct followed by biliary diversion.[28]

Hepatic Mucinous Cystic Neoplasms with Associated Invasive Carcinoma (Cystadenocarcinoma)
MCNs with associated invasive carcinoma were previously referred to as cystadenocarcinomas. These are usually found in older adults. Although these lesions can metastasize, their prognosis is better than that associated with cholangiocarcinoma.
MCNs with associated invasive carcinoma generally have a thick wall that may show large enhancing soft tissue masses protruding from the internal cyst lining. Advanced tumors may show a predominantly solid and enhancing component. PET-CT may show intense increase in metabolic activity ([Fig. 13]). Needle biopsy is not typically performed due to its low diagnostic accuracy and risk of tumor seeding.[32] [33] When imaging findings are nondiagnostic, and invasive carcinoma is suspected, surgical resection is required to confirm the diagnosis.

Intraductal Papillary Neoplasm of the Bile Ducts
Intraductal papillary neoplasm of the bile duct (IPNB) is a recently recognized entity characterized by intraductal mucin-producing tumor. This is considered a biliary equivalent of IPMN in the pancreas and is shown to demonstrate stepwise progression to cholangiocarcinoma.[34] Many different terms have been used to describe IPNB including biliary papilloma, mucin-producing bile duct tumor, and biliary tract IPMN. These tumors are distinguished from MCN by lack of ovarian stroma and communication with bile ducts. Most patients with IPNB are asymptomatic. When they do present, they present with obstructive symptoms such as jaundice and recurrent cholangitis. IPNB is more common in East Asia and shows a slight male preponderance.[35] [36]
On imaging, these patients demonstrate dilation of both upstream and downstream biliary ducts caused by intraductal obstructive growth and copious mucin production. This finding is thought to be specific for IPNB and is not seen in other conditions ([Fig. 14]). Some lesions are predominantly cystic and are thought to arise from peribiliary glands. These lesions may resemble MCN. Communication with biliary tree is a key finding in establishing the diagnosis in such cases. Although IPNB is rare, a radiologist familiar with its manifestation can help with early diagnosis when surgical resection can be curative. MRI with MR cholangiopancreatography is the most sensitive imaging modality for detection of the lesion, followed by CT and US.[37] Complete surgical resection with negative margins (R0 resection) is the standard treatment goal given the high potential for malignancy and for recurrent cholangitis and obstructive jaundice in nonmalignant cases.[38] Tumors involving the extrahepatic bile ducts are treated with Whipple's surgery, whereas tumors confined to intrahepatic bile ducts undergo hepatic resection depending on the degree of biliary involvement highlighting the importance of accurate radiological staging.[11]

Primary Hepatic Lymphoma
Hepatic lymphoma can either be primary or secondary. To be classified as primary hepatic lymphoma, the disease should be limited to the liver and hepatic hilar lymph nodes, with no distant involvement. Primary hepatic lymphoma is rare and account for less than 1% of all cases of non-Hodgkin lymphoma.[39] [40] The most common subtype of primary hepatic lymphoma is diffuse large B cell lymphoma.
Imaging appearances of hepatic lymphoma is varied.[41] They most commonly present as a large solitary hypoenhancing masses on CT and MRI ([Fig. 15]). Up to 33% are multifocal and can present as multiple small discrete nodules ([Fig. 16]). They can be isointense or hyperintense compared with the liver on T2 imaging. Other patterns include diffuse infiltration (with or without hepatomegaly) and a mass in the porta hepatis. They are usually intensely metabolically avid on fluorodeoxyglucose PET-CT.[42]


Inflammatory Pseudotumor
Inflammatory pseudotumor refers to a heterogeneous group of mass-forming lesions that can involve many organs and that are characterized by a prominent inflammatory infiltrate. In the literature, these have been described as synonymous with inflammatory myofibroblastic tumor and xanthogranulomatous tumors or plasma cell granulomas of the liver. These present most commonly in young adults with males affected more than females.[43] The patients usually present with systemic symptoms such as vague upper abdominal discomfort, loss of weight, malaise, and intermittent fever. Liver function tests are usually not useful.
On CT and MRI, these lesions have been described as having a targetoid appearance in a significant proportion of patients studied and suggest this to be a characteristic finding.[44] These tumors have a wide range of imaging appearances with no specific feature that can clinch the diagnosis on radiology alone.[45] Generally, inflammatory pseudotumors have nonspecific imaging findings. These tend to have ill-defined edges, are hypoenhancing, and can resemble common neoplastic conditions such as metastases or cholangiocarcinoma ([Fig. 17]). In view of the lack of specific imaging findings, percutaneous biopsy is key to establish diagnosis. A prudent clinician would consider this diagnosis in patients presenting with significant systemic symptoms and hepatic tenderness.




Conflict of Interest
None declared.
-
References
- 1 Darbari A, Sabin KM, Shapiro CN, Schwarz KB. Epidemiology of primary hepatic malignancies in U.S. children. Hepatology 2003; 38 (03) 560-566
- 2 Kahla JA, Siegel DA, Dai S. et al. Incidence and 5-year survival of children and adolescents with hepatoblastoma in the United States. Pediatr Blood Cancer 2022; 69 (10) e29763
- 3 Trobaugh-Lotrario AD, López-Terrada D, Li P, Feusner JH. Hepatoblastoma in patients with molecularly proven familial adenomatous polyposis: clinical characteristics and rationale for surveillance screening. Pediatr Blood Cancer 2018; 65 (08) e27103
- 4 McArthur JW, Toll GD, Russfield AB, Reiss AM, Quinby WC, Baker WH. Sexual precocity attributable to ectopic gonadotropin secretion by hepatoblastoma. Am J Med 1973; 54 (03) 390-403
- 5 Grunewald TG, von Luettichau I, Welsch U. et al. First report of ectopic ACTH syndrome and PTHrP-induced hypercalcemia due to a hepatoblastoma in a child. Eur J Endocrinol 2010; 162 (04) 813-818
- 6 Raney B. Hepatoblastoma in children: a review. J Pediatr Hematol Oncol 1997; 19 (05) 418-422
- 7 McCarville MB, Roebuck DJ. Diagnosis and staging of hepatoblastoma: imaging aspects. Pediatr Blood Cancer 2012; 59 (05) 793-799
- 8 Towbin AJ, Meyers RL, Woodley H. et al. 2017 PRETEXT: radiologic staging system for primary hepatic malignancies of childhood revised for the Paediatric Hepatic International Tumour Trial (PHITT). Pediatr Radiol 2018; 48 (04) 536-554
- 9 Meyers RL, Czauderna P, Otte JB. Surgical treatment of hepatoblastoma. Pediatr Blood Cancer 2012; 59 (05) 800-808
- 10 Suriawinata AA, Thung SN. Malignant liver tumors. Clin Liver Dis 2002; 6 (02) 527-554, ix ix.
- 11 Kim JR, Lee KB, Kwon W, Kim E, Kim SW, Jang JY. Comparison of the clinicopathologic characteristics of intraductal papillary neoplasm of the bile duct according to morphological and anatomical classifications. J Korean Med Sci 2018; 33 (42) e266
- 12 Sherman M. Vinyl chloride and the liver. J Hepatol 2009; 51 (06) 1074-1081
- 13 Groeschl RT, Miura JT, Oshima K, Gamblin TC, Turaga KK. Does histology predict outcome for malignant vascular tumors of the liver?. J Surg Oncol 2014; 109 (05) 483-486
- 14 Antonescu C. Malignant vascular tumors–an update. Mod Pathol 2014; 27 (Suppl. 01) S30-S38
- 15 Koyama T, Fletcher JG, Johnson CD, Kuo MS, Notohara K, Burgart LJ. Primary hepatic angiosarcoma: findings at CT and MR imaging. Radiology 2002; 222 (03) 667-673
- 16 Makhlouf HR, Ishak KG, Goodman ZD. Epithelioid hemangioendothelioma of the liver: a clinicopathologic study of 137 cases. Cancer 1999; 85 (03) 562-582
- 17 Mehrabi A, Kashfi A, Fonouni H. et al. Primary malignant hepatic epithelioid hemangioendothelioma: a comprehensive review of the literature with emphasis on the surgical therapy. Cancer 2006; 107 (09) 2108-2121
- 18 Ganeshan D, Pickhardt PJ, Morani AC. et al. Hepatic hemangioendothelioma: CT, MR, and FDG-PET-CT in 67 patients-a bi-institutional comprehensive cancer center review. Eur Radiol 2020; 30 (05) 2435-2442
- 19 Zhou L, Cui MY, Xiong J. et al. Spectrum of appearances on CT and MRI of hepatic epithelioid hemangioendothelioma. BMC Gastroenterol 2015; 15: 69
- 20 Alomari AI. The lollipop sign: a new cross-sectional sign of hepatic epithelioid hemangioendothelioma. Eur J Radiol 2006; 59 (03) 460-464
- 21 Liu X, Yu H, Zhang Z. et al. MRI appearances of hepatic epithelioid hemangioendothelioma: a retrospective study of 57 patients. Insights Imaging 2022; 13 (01) 65
- 22 Hornick JL, Fletcher CD. PEComa: what do we know so far?. Histopathology 2006; 48 (01) 75-82
- 23 Cai PQ, Wu YP, Xie CM, Zhang WD, Han R, Wu PH. Hepatic angiomyolipoma: CT and MR imaging findings with clinical-pathologic comparison. Abdom Imaging 2013; 38 (03) 482-489
- 24 Nonomura A, Enomoto Y, Takeda M, Takano M, Morita K, Kasai T. Angiomyolipoma of the liver: a reappraisal of morphological features and delineation of new characteristic histological features from the clinicopathological findings of 55 tumours in 47 patients. Histopathology 2012; 61 (05) 863-880
- 25 Yang X, Li A, Wu M. Hepatic angiomyolipoma: clinical, imaging and pathological features in 178 cases. Med Oncol 2013; 30 (01) 416
- 26 Arnaoutakis DJ, Kim Y, Pulitano C. et al. Management of biliary cystic tumors: a multi-institutional analysis of a rare liver tumor. Ann Surg 2015; 261 (02) 361-367
- 27 Soares KC, Arnaoutakis DJ, Kamel I. et al. Cystic neoplasms of the liver: biliary cystadenoma and cystadenocarcinoma. J Am Coll Surg 2014; 218 (01) 119-128
- 28 Davies W, Chow M, Nagorney D. Extrahepatic biliary cystadenomas and cystadenocarcinoma. Report of seven cases and review of the literature. Ann Surg 1995; 222 (05) 619-625
- 29 Sang X, Sun Y, Mao Y. et al. Hepatobiliary cystadenomas and cystadenocarcinomas: a report of 33 cases. Liver Int 2011; 31 (09) 1337-1344
- 30 Lewin M, Mourra N, Honigman I. et al. Assessment of MRI and MRCP in diagnosis of biliary cystadenoma and cystadenocarcinoma. Eur Radiol 2006; 16 (02) 407-413
- 31 Vyas S, Markar S, Ezzat T. et al. Hepato-biliary cystadenoma with intraductal extension: unusual cause of obstructive jaundice. J Gastrointest Cancer 2012; 43 (Suppl. 01) S32-S37
- 32 Hai S, Hirohashi K, Uenishi T. et al. Surgical management of cystic hepatic neoplasms. J Gastroenterol 2003; 38 (08) 759-764
- 33 Tholomier C, Wang Y, Aleynikova O, Vanounou T, Pelletier JS. Biliary mucinous cystic neoplasm mimicking a hydatid cyst: a case report and literature review. BMC Gastroenterol 2019; 19 (01) 103
- 34 Schlitter AM, Born D, Bettstetter M. et al. Intraductal papillary neoplasms of the bile duct: stepwise progression to carcinoma involves common molecular pathways. Mod Pathol 2014; 27 (01) 73-86
- 35 Zen Y, Jang KT, Ahn S. et al. Intraductal papillary neoplasms and mucinous cystic neoplasms of the hepatobiliary system: demographic differences between Asian and Western populations, and comparison with pancreatic counterparts. Histopathology 2014; 65 (02) 164-173
- 36 Kubota K, Jang JY, Nakanuma Y. et al. Clinicopathological characteristics of intraductal papillary neoplasm of the bile duct: a Japan-Korea collaborative study. J Hepatobiliary Pancreat Sci 2020; 27 (09) 581-597
- 37 Park HJ, Kim SY, Kim HJ. et al. Intraductal papillary neoplasm of the bile duct: clinical, imaging, and pathologic features. AJR Am J Roentgenol 2018; 211 (01) 67-75
- 38 Ohtsuka M, Shimizu H, Kato A. et al. Intraductal papillary neoplasms of the bile duct. Int J Hepatol 2014; 2014: 459091
- 39 Harris AC, Ben-Ezra JM, Contos MJ, Kornstein MJ. Malignant lymphoma can present as hepatobiliary disease. Cancer 1996; 78 (09) 2011-2019
- 40 Lei KI. Primary non-Hodgkin's lymphoma of the liver. Leuk Lymphoma 1998; 29 (3-4): 293-299
- 41 Elsayes KM, Menias CO, Willatt JM, Pandya A, Wiggins M, Platt J. Primary hepatic lymphoma: imaging findings. J Med Imaging Radiat Oncol 2009; 53 (04) 373-379
- 42 Hu HJ, Qu YJ, Tian ZX, Zhang ZP. Clinical and radiographic observations from four patients with primary hepatic lymphoma. Exp Ther Med 2016; 11 (02) 381-386
- 43 Patnana M, Sevrukov AB, Elsayes KM, Viswanathan C, Lubner M, Menias CO. Inflammatory pseudotumor: the great mimicker. AJR Am J Roentgenol 2012; 198 (03) W217-27
- 44 Calistri L, Maraghelli D, Nardi C. et al. Magnetic resonance imaging of inflammatory pseudotumor of the liver: a 2021 systematic literature update and series presentation. Abdom Radiol (NY) 2022; 47 (08) 2795-2810
- 45 Yan FH, Zhou KR, Jiang YP, Shi WB. Inflammatory pseudotumor of the liver: 13 cases of MRI findings. World J Gastroenterol 2001; 7 (03) 422-424
Address for correspondence
Publication History
Article published online:
17 April 2023
© 2023. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Darbari A, Sabin KM, Shapiro CN, Schwarz KB. Epidemiology of primary hepatic malignancies in U.S. children. Hepatology 2003; 38 (03) 560-566
- 2 Kahla JA, Siegel DA, Dai S. et al. Incidence and 5-year survival of children and adolescents with hepatoblastoma in the United States. Pediatr Blood Cancer 2022; 69 (10) e29763
- 3 Trobaugh-Lotrario AD, López-Terrada D, Li P, Feusner JH. Hepatoblastoma in patients with molecularly proven familial adenomatous polyposis: clinical characteristics and rationale for surveillance screening. Pediatr Blood Cancer 2018; 65 (08) e27103
- 4 McArthur JW, Toll GD, Russfield AB, Reiss AM, Quinby WC, Baker WH. Sexual precocity attributable to ectopic gonadotropin secretion by hepatoblastoma. Am J Med 1973; 54 (03) 390-403
- 5 Grunewald TG, von Luettichau I, Welsch U. et al. First report of ectopic ACTH syndrome and PTHrP-induced hypercalcemia due to a hepatoblastoma in a child. Eur J Endocrinol 2010; 162 (04) 813-818
- 6 Raney B. Hepatoblastoma in children: a review. J Pediatr Hematol Oncol 1997; 19 (05) 418-422
- 7 McCarville MB, Roebuck DJ. Diagnosis and staging of hepatoblastoma: imaging aspects. Pediatr Blood Cancer 2012; 59 (05) 793-799
- 8 Towbin AJ, Meyers RL, Woodley H. et al. 2017 PRETEXT: radiologic staging system for primary hepatic malignancies of childhood revised for the Paediatric Hepatic International Tumour Trial (PHITT). Pediatr Radiol 2018; 48 (04) 536-554
- 9 Meyers RL, Czauderna P, Otte JB. Surgical treatment of hepatoblastoma. Pediatr Blood Cancer 2012; 59 (05) 800-808
- 10 Suriawinata AA, Thung SN. Malignant liver tumors. Clin Liver Dis 2002; 6 (02) 527-554, ix ix.
- 11 Kim JR, Lee KB, Kwon W, Kim E, Kim SW, Jang JY. Comparison of the clinicopathologic characteristics of intraductal papillary neoplasm of the bile duct according to morphological and anatomical classifications. J Korean Med Sci 2018; 33 (42) e266
- 12 Sherman M. Vinyl chloride and the liver. J Hepatol 2009; 51 (06) 1074-1081
- 13 Groeschl RT, Miura JT, Oshima K, Gamblin TC, Turaga KK. Does histology predict outcome for malignant vascular tumors of the liver?. J Surg Oncol 2014; 109 (05) 483-486
- 14 Antonescu C. Malignant vascular tumors–an update. Mod Pathol 2014; 27 (Suppl. 01) S30-S38
- 15 Koyama T, Fletcher JG, Johnson CD, Kuo MS, Notohara K, Burgart LJ. Primary hepatic angiosarcoma: findings at CT and MR imaging. Radiology 2002; 222 (03) 667-673
- 16 Makhlouf HR, Ishak KG, Goodman ZD. Epithelioid hemangioendothelioma of the liver: a clinicopathologic study of 137 cases. Cancer 1999; 85 (03) 562-582
- 17 Mehrabi A, Kashfi A, Fonouni H. et al. Primary malignant hepatic epithelioid hemangioendothelioma: a comprehensive review of the literature with emphasis on the surgical therapy. Cancer 2006; 107 (09) 2108-2121
- 18 Ganeshan D, Pickhardt PJ, Morani AC. et al. Hepatic hemangioendothelioma: CT, MR, and FDG-PET-CT in 67 patients-a bi-institutional comprehensive cancer center review. Eur Radiol 2020; 30 (05) 2435-2442
- 19 Zhou L, Cui MY, Xiong J. et al. Spectrum of appearances on CT and MRI of hepatic epithelioid hemangioendothelioma. BMC Gastroenterol 2015; 15: 69
- 20 Alomari AI. The lollipop sign: a new cross-sectional sign of hepatic epithelioid hemangioendothelioma. Eur J Radiol 2006; 59 (03) 460-464
- 21 Liu X, Yu H, Zhang Z. et al. MRI appearances of hepatic epithelioid hemangioendothelioma: a retrospective study of 57 patients. Insights Imaging 2022; 13 (01) 65
- 22 Hornick JL, Fletcher CD. PEComa: what do we know so far?. Histopathology 2006; 48 (01) 75-82
- 23 Cai PQ, Wu YP, Xie CM, Zhang WD, Han R, Wu PH. Hepatic angiomyolipoma: CT and MR imaging findings with clinical-pathologic comparison. Abdom Imaging 2013; 38 (03) 482-489
- 24 Nonomura A, Enomoto Y, Takeda M, Takano M, Morita K, Kasai T. Angiomyolipoma of the liver: a reappraisal of morphological features and delineation of new characteristic histological features from the clinicopathological findings of 55 tumours in 47 patients. Histopathology 2012; 61 (05) 863-880
- 25 Yang X, Li A, Wu M. Hepatic angiomyolipoma: clinical, imaging and pathological features in 178 cases. Med Oncol 2013; 30 (01) 416
- 26 Arnaoutakis DJ, Kim Y, Pulitano C. et al. Management of biliary cystic tumors: a multi-institutional analysis of a rare liver tumor. Ann Surg 2015; 261 (02) 361-367
- 27 Soares KC, Arnaoutakis DJ, Kamel I. et al. Cystic neoplasms of the liver: biliary cystadenoma and cystadenocarcinoma. J Am Coll Surg 2014; 218 (01) 119-128
- 28 Davies W, Chow M, Nagorney D. Extrahepatic biliary cystadenomas and cystadenocarcinoma. Report of seven cases and review of the literature. Ann Surg 1995; 222 (05) 619-625
- 29 Sang X, Sun Y, Mao Y. et al. Hepatobiliary cystadenomas and cystadenocarcinomas: a report of 33 cases. Liver Int 2011; 31 (09) 1337-1344
- 30 Lewin M, Mourra N, Honigman I. et al. Assessment of MRI and MRCP in diagnosis of biliary cystadenoma and cystadenocarcinoma. Eur Radiol 2006; 16 (02) 407-413
- 31 Vyas S, Markar S, Ezzat T. et al. Hepato-biliary cystadenoma with intraductal extension: unusual cause of obstructive jaundice. J Gastrointest Cancer 2012; 43 (Suppl. 01) S32-S37
- 32 Hai S, Hirohashi K, Uenishi T. et al. Surgical management of cystic hepatic neoplasms. J Gastroenterol 2003; 38 (08) 759-764
- 33 Tholomier C, Wang Y, Aleynikova O, Vanounou T, Pelletier JS. Biliary mucinous cystic neoplasm mimicking a hydatid cyst: a case report and literature review. BMC Gastroenterol 2019; 19 (01) 103
- 34 Schlitter AM, Born D, Bettstetter M. et al. Intraductal papillary neoplasms of the bile duct: stepwise progression to carcinoma involves common molecular pathways. Mod Pathol 2014; 27 (01) 73-86
- 35 Zen Y, Jang KT, Ahn S. et al. Intraductal papillary neoplasms and mucinous cystic neoplasms of the hepatobiliary system: demographic differences between Asian and Western populations, and comparison with pancreatic counterparts. Histopathology 2014; 65 (02) 164-173
- 36 Kubota K, Jang JY, Nakanuma Y. et al. Clinicopathological characteristics of intraductal papillary neoplasm of the bile duct: a Japan-Korea collaborative study. J Hepatobiliary Pancreat Sci 2020; 27 (09) 581-597
- 37 Park HJ, Kim SY, Kim HJ. et al. Intraductal papillary neoplasm of the bile duct: clinical, imaging, and pathologic features. AJR Am J Roentgenol 2018; 211 (01) 67-75
- 38 Ohtsuka M, Shimizu H, Kato A. et al. Intraductal papillary neoplasms of the bile duct. Int J Hepatol 2014; 2014: 459091
- 39 Harris AC, Ben-Ezra JM, Contos MJ, Kornstein MJ. Malignant lymphoma can present as hepatobiliary disease. Cancer 1996; 78 (09) 2011-2019
- 40 Lei KI. Primary non-Hodgkin's lymphoma of the liver. Leuk Lymphoma 1998; 29 (3-4): 293-299
- 41 Elsayes KM, Menias CO, Willatt JM, Pandya A, Wiggins M, Platt J. Primary hepatic lymphoma: imaging findings. J Med Imaging Radiat Oncol 2009; 53 (04) 373-379
- 42 Hu HJ, Qu YJ, Tian ZX, Zhang ZP. Clinical and radiographic observations from four patients with primary hepatic lymphoma. Exp Ther Med 2016; 11 (02) 381-386
- 43 Patnana M, Sevrukov AB, Elsayes KM, Viswanathan C, Lubner M, Menias CO. Inflammatory pseudotumor: the great mimicker. AJR Am J Roentgenol 2012; 198 (03) W217-27
- 44 Calistri L, Maraghelli D, Nardi C. et al. Magnetic resonance imaging of inflammatory pseudotumor of the liver: a 2021 systematic literature update and series presentation. Abdom Radiol (NY) 2022; 47 (08) 2795-2810
- 45 Yan FH, Zhou KR, Jiang YP, Shi WB. Inflammatory pseudotumor of the liver: 13 cases of MRI findings. World J Gastroenterol 2001; 7 (03) 422-424