

Subscribe to RSS
DOI: 10.1055/s-0046-1816559
Biliary Stricture: Imaging Overview
Authors


Abstract
Biliary strictures are narrowings involving any part of the biliary tree, intrahepatic or extrahepatic. This pathology has various etiologies, including benign and malignant. Patients mostly present with jaundice and features of cholangitis. Although ultrasonography is the initial modality in most cases, computed tomography scan and magnetic resonance imaging form the main imaging techniques that help in the localization and characterization of the strictures and assist in providing a definite or possible diagnosis. This review provides an overview of the role of imaging in the evaluation of biliary strictures.
Introduction
Biliary stricture is defined as a pathological narrowing of the bile ducts that impedes the normal flow of bile from the liver to the duodenum. They are clinically significant as they can lead to obstructive jaundice, cholangitis, liver dysfunction, and biliary cirrhosis if not promptly identified and managed. While a significant proportion of biliary strictures tend to be indeterminate initially, biliary strictures may be classified as benign or malignant.[1]
Radiological evaluation plays a central role in the diagnosis and management of biliary strictures. Imaging not only confirms the presence of a stricture but also helps localize the level of obstruction, assess its extent, and suggest possible etiology. Ultrasonography (USG) is typically the first-line modality, while magnetic resonance cholangiopancreatography (MRCP), computed tomography (CT), and endoscopic retrograde cholangiopancreatography (ERCP) offer detailed anatomical and functional insights. Timely and accurate imaging is essential in differentiating benign and malignant causes and for guiding appropriate therapeutic strategies, including surgical, endoscopic, or percutaneous interventions.[1] [2] [3] [4]
Benign Biliary Strictures
About 30% of diagnosed biliary strictures are benign in nature.[5] The etiology of benign biliary strictures (BBSs) is diverse, with iatrogenic injury being the most prevalent cause.[6] These commonly include cholecystectomy, bile duct surgeries, and liver transplantation. Other notable causes include primary sclerosing cholangitis (PSC), IgG4-related sclerosing cholangiopathy, portal cholangiopathy, recurrent pyogenic cholangitis, acquired immune deficiency syndrome cholangiopathy, and chemotherapy-associated sclerosing cholangitis. More often than not, they may follow a more insidious course requiring intensive multidisciplinary management, which increases health care costs. Accurate imaging assessment and targeted interventions are essential for diagnosis and guiding appropriate management.[7] [8]
Malignant Biliary Strictures
A majority of biliary strictures tend to be malignant in nature.[5] The most common causes of malignant biliary strictures (MBS) include pancreatic adenocarcinoma, gallbladder cancer, and cholangiocarcinoma. Less frequently, they may result from metastatic disease involving the pancreas or liver, ampullary tumors extending into the bile duct, or malignant periportal lymphadenopathy.
In patients presenting with obstructive jaundice, all bile duct strictures should be presumed malignant until a benign cause is definitively established.[8] Preoperative confirmation of malignancy is crucial, as it significantly influences clinical decision-making and may necessitate extensive surgical intervention. The prognosis for MBS is highly variable. Gallbladder cancer, pancreatic adenocarcinoma, and cholangiocarcinoma are often diagnosed at advanced stages, which can severely limit treatment options. Therefore, early suspicion and accurate characterization through imaging are essential for timely diagnosis and effective management.
Role of Imaging
Ultrasonography
USG is typically the first-line imaging technique used to evaluate obstructive jaundice.[3] It is widely preferred due to its noninvasive nature, availability, and ability to provide real-time imaging. USG demonstrates a high sensitivity in identifying biliary obstruction and can accurately determine the level at which the obstruction occurs, with an overall accuracy exceeding 90% ([Fig. 1]).[4] However, its effectiveness in identifying the specific underlying cause of the obstruction is considerably limited, with reported accuracy rates ranging from 30 to 70%.[3] Additionally, the diagnostic quality of USG is significantly influenced by the skill and experience of the operator, patient's habitus, and bowel gas.[3] [4]

USG serves its purpose of acting as a first-line modality in the following ways[3]:
-
Detecting if biliary dilatation is present or not.
-
Determining the level of block with any associated intra-/peri-/extra-ductal thickening or mass.
-
Extent of stricture (length of narrowing/involvement of biliary confluence).
-
Associated biliary complications (cholangitic abscess/bilomas/hepatolithiasis/choledocholithiasis).
-
Amenability of percutaneous interventions (percutaneous transhepatic biliary drainage/abscess or collection drainage/tissue sampling)
-
Any changes in chronic liver disease and portal hypertension.
-
However, USG has the following shortcomings:
-
Delineating the true extent of disease (especially the mid- and distal common bile duct segment) is difficult.
-
Duct wall/periductal thickenings can very often be missed.
-
No information on the enhancement character of the disease.
-
Limited evaluation of the transition point (in terms of abrupt cut-off/beaking).
Many of these limitations can be overcome by following a stepwise approach or a fixed scanning protocol. Visualization may be further improved by left lateral decubitus (for the extrahepatic bile duct), pancreatic window, and oral water intake (for the distal bile duct).
Beyond traditional grayscale imaging, ultrasound elastography is emerging as a valuable noninvasive adjunct. This technique measures tissue stiffness and has significant potential in evaluating biliary strictures. In the evaluation of biliary strictures, it has the potential to differentiate benign from malignant lesions by detecting increased stiffness associated with malignancy (secondary to desmoplasia); however, there is as yet no available literature proving the modality's efficacy for the same. Elastography also aids in assessing liver fibrosis in chronic biliary disorders such as PSC and biliary atresia, helping guide prognosis and management.[9] Additional advantage is that the liver stiffness can be followed up noninvasively in patients with secondary biliary cirrhosis to look for treatment response or disease progression.
Contrast-Enhanced Ultrasound
Conventional USG has limited capability in visualizing the microcirculation/vascularity of biliary lesions, which can result in missed or inaccurate diagnoses in a considerable number of cases. Contrast-enhanced ultrasound (CEUS) involves injecting a USG contrast agent (SonoVue—commonly available agent in India) intravenously, followed by saline flush and imaging the region of interest for 60 to180 seconds after injection.[4] [10]
CEUS plays an important role in the characterization of biliary strictures, particularly in differentiating benign from malignant etiologies. CEUS showed an overall accuracy of 86.4%, with a sensitivity of 85.7% for detecting malignant biliary lesions (including cholangiocarcinoma) and a specificity of 88.2% for benign biliary etiologies (such as biliary sludge or lithiasis).[11] CEUS also enhances visualization of bile duct invasion in hepatic tumors and better delineates the extension of hilar neoplasms. It can help assess the vascularity patterns and enhancement dynamics of strictures or associated masses, which aids in distinguishing cholangiocarcinoma from benign inflammatory causes. CEUS is especially valuable in evaluating hilar (Klatskin) tumors, detecting malignant transformation in congenital anomalies like Caroli's disease, and differentiating bile duct malignancy and non-shadowing stones or sludge. Its real-time imaging capability and absence of nephrotoxicity make it a useful adjunct in patients with renal dysfunction or when magnetic resonance imaging (MRI) is contraindicated.[4] [10]
Computed Tomography
CT, particularly with multi-detector (MDCT [multi-detector CT]) technology, provides improved sensitivity over USG for not only detecting biliary strictures, but also characterizing them with good accuracy. MDCT enhances lesion visualization through superior spatial resolution and contrast enhancement patterns ([Figs. 2] and [3]). Studies have shown a sensitivity of 75–80% and a specificity of 60–80% for predicting the nature of biliary strictures using CT.[5] CT is also relevant in providing detailed information on local extension, vascular invasion, lymphadenopathy, and distant metastases. In malignant biliary disease, MDCT shows excellent accuracy for identifying arterial and portal vein involvement (sensitivity: 85–86%; specificity: 97%) and moderate sensitivity (53%) but high specificity (95%) for nodal disease.[12] With few variations, the overall CT protocol for biliary pathology assessment remains the same throughout all institutions. In our institute, we advocate distending the gastrointestinal tract by 800 to 1,000 mL of oral water prior to the scan. An intravenous nonionic contrast agent is then administered at ∼1.5–2 mL/kg (80–100 mL) dose. Three phases are acquired following contrast injection: late arterial (30 seconds), portal venous (70 seconds), and delayed (180 seconds) phases. All three phases provide crucial information on detection and staging:


-
Late arterial phase: arterial anatomy and variations (required for pre-op planning), artery involvement (resectability for malignant strictures), arterial phase enhancement (malignant strictures show more enhancement).
-
Portal venous phase: nodal and organ metastasis, venous patency and involvement, lesion enhancement pattern.
-
Delayed phase: delayed contrast retention (contrast retention is common with scirrhous and fibrotic lesions).
Despite significant advances in scanners, CT cannot replicate the contrast resolution offered by MRI. Biliary radicles and ducts appear hypodense in relation to the surrounding soft tissue and parenchyma and that significantly limits the exact character and extent of narrowing, especially when the dilatation is not significant. It is a common practice to make reformatted images of the biliary tree on the porto-venous phase using the MinIP function wherever corresponding MRCP images are not available ([Fig. 2]). Despite these efforts, the multiparametric assessment possible on MRI is not achievable on a CT scan.
Dual-Energy CT
Spectral CT, also known as dual-energy CT, enhances biliary imaging by providing material-specific data and improved tissue characterization. It enables iodine mapping, virtual noncontrast imaging, and monoenergetic reconstructions, which improve lesion conspicuity and delineation of biliary strictures or masses ([Fig. 4]). Spectral CT has the potential to enhance the detection of subtle bile duct wall enhancement, vascular invasion, and lymphadenopathy, aiding in the differentiation between benign and malignant strictures. However, there is no published data proving the accuracy of the modality for the same. It is particularly valuable in patients who cannot undergo MRI. Additionally, it reduces beam-hardening artifacts and improves contrast resolution, making it a useful adjunct in comprehensive biliary assessment and treatment planning.[13] [14]

Split-Bolus CT Technique
The split-bolus technique of CT involves administering intravenous contrast in two separate boluses at timed intervals, allowing simultaneous capture of multiple contrast phases—typically arterial and venous or venous and delayed—in a single scan acquisition. This approach reduces radiation exposure while preserving diagnostic information. In biliary imaging, it enhances visualization of both vascular anatomy (allowing surgical resectability assessment) and biliary structures, aiding in the assessment of strictures, masses, vascular invasion, and postoperative complications. It is particularly useful for preoperative evaluation in cholangiocarcinoma or pancreatic cancer, optimizing lesion characterization and surgical planning while reducing radiation exposure to the patient.[15] [16]
CT Cholangiography
CT cholangiography is a diagnostic imaging technique used to visualize the biliary tree, often in patients with suspected biliary obstruction, biliary anomalies, or bile duct injuries. It involves intravenous administration of an iodinated contrast agent (meglumine iotroxate [Biliscopin] or meglumine iodoxamate [Endobil]) that is excreted into the bile. CT images are acquired 60 to 90 minutes after injection, allowing contrast-filled bile ducts to be clearly delineated.[17] [18]
This modality offers high spatial resolution and is particularly useful when MRCP is contraindicated or unavailable. It can effectively demonstrate biliary anatomy, strictures, dilatations, and post-surgical anatomy. However, its utility may be limited in patients with impaired liver function, as contrast excretion into bile may be insufficient. Additional radiation exposure and the inherent risks of iodinated contrast agents remain notable limitations. Despite these factors, CT cholangiography is highly valuable for preoperative planning, particularly in evaluating bile duct injuries or performing living liver donor assessments.
Although they have clinical value, these contrast agents are not available in India and many other countries, mainly due to the availability of better imaging modalities like MRCP and ERCP.
Magnetic Resonance Imaging
MRI, particularly MRCP, is increasingly utilized for evaluating biliary strictures. Compared with MDCT, MRCP offers several advantages: it avoids ionizing radiation and provides detailed, noninvasive cholangiographic images that help determine the site, extent, and character of the biliary strictures. Higher contrast resolution imaging is possible with MRI, which allows for better delineation of the stricture in terms of abruptness, irregularity, and angle of narrowing, especially in cases with mild biliary dilatation ([Figs. 5] and [6]). MRCP helps in differentiating malignant from benign strictures, with a reported sensitivity of 38 to 90% and a specificity of 70 to 85%, along with 88 to 96% accuracy in predicting the extent of involvement of the bile duct by cholangiocarcinoma.[5]

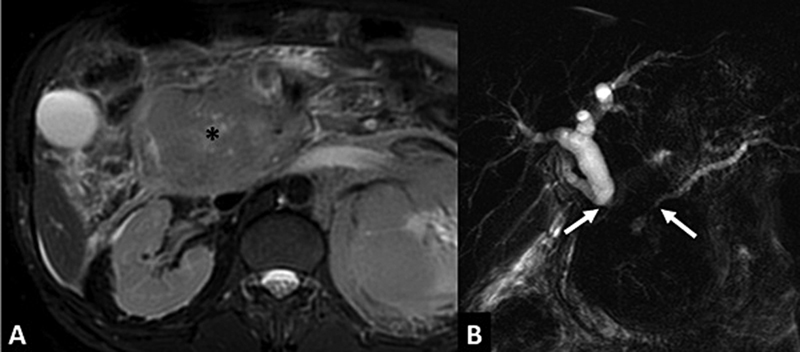
Apart from anatomic and enhancement character, signal character on multiple sequences (T2-weighted [T2W], T1-weighted [T1W], diffusion-weighted imaging [DWI]) provides greater information on the character of the biliary stricture. Benign or fibrotic strictures tend to be hypointense on T1W and T2W MRI without any diffusion restriction ([Fig. 7]), while malignant or cellular strictures show intermediate or hyperintense signal on T2W MRI with associated diffusion restriction and early contrast enhancement.[2] Another important advantage is that MRCP does not require contrast injection into the biliary system, reducing the risk of postprocedural cholangitis, a key limitation of ERCP, while providing a biliary tree map noninvasively.[2] [5] [8]

The MRI protocol across institutions tends to be similar, with only a few differences. The protocol for MRI with MRCP for biliary pathology involves: axial T1W in-phase and out-of-phase, T2W fat-saturated, and DWI sequences; coronal T2W fat-saturated and balanced steady-state free precession sequences; three-dimensional (3D) MRCP, thick-slab single-shot MRCP; and post-contrast axial 3D T1 fat-saturated sequences (pre-contrast, late arterial [25–30 seconds], portal venous [50–55 seconds], hepatic venous [60–70 seconds], and delayed [180 seconds] phases) and coronal T1 fat-saturated sequences.
Contrast-enhanced MRI is commonly performed for newly diagnosed biliary strictures, especially when malignancy is suspected. However, it may be omitted in postoperative settings—such as after cholecystectomy or liver transplantation—where the etiology is typically benign, and the likelihood of malignancy is low.
T1 Magnetic Resonance Cholangiography
Another method of performing cholangiography is doing a contrast-enhanced T1 imaging of the biliary tree, also known as functional MR cholangiography. This technique uses hepatobiliary-specific gadolinium-based contrast agents such as gadobenate dimeglumine (Gd-BOPTA), gadolinium ethoxybenzyldiethylenetriamine penta-acetic acid (Gd-EOB-DTPA), and, historically, mangafodipir trisodium. These agents are excreted into the bile, allowing for high signal intensity on delayed T1W 3D fat-saturated GRE (gradient recalled echo) images (typically 10–120 minutes post-injection depending on the type of contrast agent used), offering superior direct bile duct visualization compared with conventional T2 MRCP ([Fig. 8]).

T1-MRCP provides both functional and anatomical insights, with reduced susceptibility to artifacts compared with T2-MRCP. In cases of suspected biliary obstruction, the addition of T1-MRC to standard MRI protocols, including T2-MRCP, has been shown to increase sensitivity from approximately 60 to 91% and improve diagnostic confidence, especially in cases of subtle and equivocal strictures.[19] [20]
Endoscopic Modalities
Unlike the traditional imaging techniques discussed so far, endoscopic modalities not only enable image-based characterization but also allow for the collection of histological samples.[5] A key advantage of these techniques is the ability to perform therapeutic interventions during the same session. As with all invasive procedures, endoscopic methods typically require more extensive patient preparation, are expensive, and carry a variable risk of complications.
The three most commonly used endoscopic procedures are discussed below.
ERCP has traditionally been central in evaluating biliary strictures, allowing for visualization, sampling (brushings, biopsies, or fluid cytology), and therapeutic intervention ([Fig. 9]). ERCP with brush cytology and intraductal biopsies have high specificity (around 99–100%) for detecting MBSs, but their sensitivity is limited, ranging from 45 to 48%, due to the fibrotic nature of tumors.[5] Advanced tools like cholangioscopy, confocal endomicroscopy, and spectroscopy are emerging, aiming to improve tissue characterization.

Endoscopic ultrasound (EUS) is increasingly being used for hilar and distal biliary strictures, offering high sensitivity (more than 70%), especially when paired with fine needle aspiration (EUS-FNA).[5] While EUS-FNA improves diagnostic yield, concerns about needle tract seeding, particularly in proximal strictures, limit its use in transplant candidates. Still, EUS is valuable in detecting malignancy, lymphadenopathy, or alternative causes such as impacted stones or metastatic lesions.[5]
Intraductal ultrasonography, performed during ERCP, provides high-resolution imaging of the bile duct wall. It involves the insertion of a high-frequency probe (12–40 MHz) into the bile duct probe guided by a wire.[2] [5] Owing to the very high local resolution, it enhances the accuracy of stricture characterization and can assist in local tumor staging. Despite promising performance, its use is limited by availability and operator expertise and is mainly available in tertiary health care centers and academic institutions.[21] [22]
Percutaneous Transhepatic Cholangiography
Percutaneous transhepatic cholangiography (PTC) is a valuable diagnostic and therapeutic modality for evaluating biliary strictures, particularly when endoscopic access is limited or unsuccessful, such as in high hilar strictures or cases with surgically altered anatomy. It demonstrates a sensitivity of 70.8 to 86.7% and a specificity of 47.6 to 100% for diagnosing biliary strictures.[23] In malignant strictures, PTC shows a sensitivity of 61% and a specificity of 100%, while biopsy via PTC yields 80% sensitivity and 100% specificity.[23]
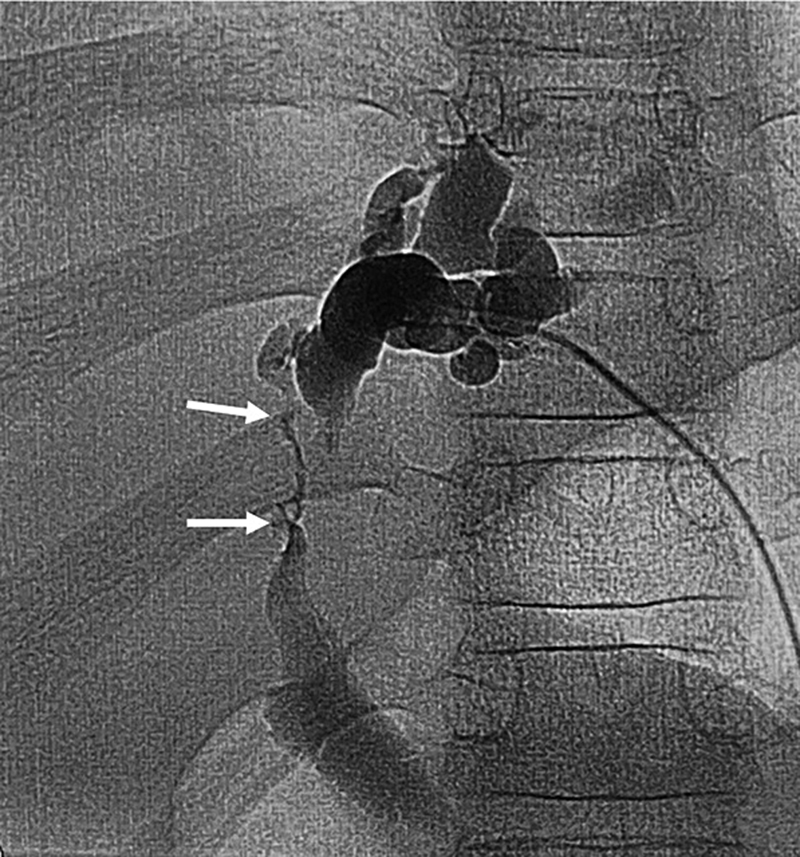
PTC involves percutaneous puncture of a peripheral intrahepatic biliary radicle and injecting contrast under fluoroscopy ([Fig. 10]). It offers detailed imaging of the intrahepatic and extrahepatic bile ducts and allows for direct intervention, including drainage, stent placement, balloon dilation, and tissue sampling. In the differentiation of benign from malignant strictures, PTC can reveal specific morphological features—malignant strictures often appear as irregular, long-segment narrowing with abrupt transition or shouldered margin, while benign strictures are typically short, smooth, and gradually tapered.[23] [24] Fluoroscopic assessment during PTC may also identify subtle mucosal irregularities or filling defects, which can be missed during cross-sectional imaging owing to higher spatial resolution. Additionally, intraprocedural brush cytology or biopsy can be obtained, which enhances diagnostic accuracy. However, a significant disadvantage of PTC is the 2D nature of the images provided. Although oblique and lateral images can be obtained with tube rotation, a simultaneous 3D image available with CT/MRI cannot be replicated. Also, the procedure is invasive and associated with risks such as bleeding or infection. All said, PTC is indispensable in complex cases where noninvasive imaging or ERCP fails to provide a definitive diagnosis or therapeutic route.[25]
Benign versus Malignant Biliary Stricture
Differentiating BBS from MBS is a critical diagnostic challenge with significant therapeutic implications. A systematic multimodality approach—typically involving USG, CT, MRI/MRCP, and occasionally ERCP or PTC—is essential. Key features differentiating malignant and benign strictures are summarized in [Table 1].[2] [6] [10]
Abbreviation: MRI, magnetic resonance imaging.
Features Suggestive of Malignancy
MBSs are most commonly due to cholangiocarcinoma, pancreatic carcinoma, metastases, or gallbladder carcinoma. Key imaging signs include:
-
Stricture length: malignant strictures tend to be long-segment (>12 mm) and irregular.
-
Margin characteristics: abrupt transition, shouldered edges, and asymmetry favor a malignant etiology.
-
Wall thickening: irregular, eccentric wall thickening >3 mm, often with heterogeneous enhancement.
-
Enhancing mass: presence of a soft-tissue mass at the site of stricture is highly suggestive of malignancy.
-
Biliary ductal changes: marked upstream biliary dilatation, especially if disproportionate to the level of narrowing.
-
Periductal involvement: loss of fat planes, vascular encasement, or invasion of adjacent organs.
-
Lymphadenopathy: enlarged, often necrotic or clustered, nodes in the porta hepatis or peripancreatic region.
-
Diffusion restriction (on MRI): suggestive of hypercellular malignant tissue.
Features Favoring Benign Etiology
BBSs are often related to inflammation, trauma, prior interventions, or autoimmune conditions. Imaging features include:
-
Short segment narrowing, usually <10 mm, with smooth, tapered margins.
-
Symmetric wall thickening, usually mild and without significant enhancement.
-
Associated findings include:
-
− Postoperative changes (e.g., anastomotic stricture).
-
− Chronic pancreatitis or adjacent inflammatory fat stranding.
-
− Choledocholithiasis or sludge causing transient narrowing.
-
-
No associated mass, vascular involvement, or significant lymphadenopathy.
-
Improvement or stability over time on follow-up imaging.
-
Normalization with medical treatment (e.g., antibiotics or steroids in IgG4 cholangitis).
Bismuth Classification
The Bismuth–Corlette classification is a widely used system to describe the anatomical extent of hilar bile duct strictures, originally developed for perihilar cholangiocarcinoma but also applicable to benign strictures involving the biliary confluence ([Tables 2] and [3]; [Figs. 11] and [12]).


|
Type |
Description |
|---|---|
|
Type I |
Stricture located below the primary biliary confluence |
|
Type II |
Stricture involves the primary biliary confluence, but does not extend into right or left hepatic ducts |
|
Type IIIa |
Stricture involves the primary biliary confluence and extends into the right hepatic duct/left secondary confluence |
|
Type IIIb |
Stricture involves the primary biliary confluence and extends into the left hepatic duct/left secondary confluence |
|
Type IV |
Multifocal or bilateral involvement of right and left hepatic ducts. |
|
Type |
Description |
|---|---|
|
Type I |
Stricture located more than 2 cm distal to the primary biliary confluence |
|
Type II |
Stricture within 2 cm from the primary biliary confluence |
|
Type III |
Stricture involving the primary biliary confluence, but is patent |
|
Type IV |
Stricture involving and blocking the primary biliary confluence |
|
Type V |
Stricture involving the hepatic duct and an aberrant right segmental branch |
Despite best efforts, it is very frequently impossible to characterize the biliary stricture with just wall thickening into either category. IgG4-related sclerosing cholangitis can closely mimic cholangiocarcinoma on imaging; however, certain distinguishing features may suggest the diagnosis, including the presence of multiple strictures, associated autoimmune pancreatitis, elevated serum IgG4 levels, and a dramatic response to steroid therapy.[26] Similarly, PSC may present with a characteristic beaded appearance of the bile ducts, featuring alternating strictures and dilations, often in a multifocal distribution and typically associated with underlying inflammatory bowel disease.[27] While biomarkers such as CA 19–9 may aid in supporting the diagnosis, they are not definitive.
In cases where imaging findings remain inconclusive, tissue sampling through ERCP, EUS-FNA, or brush cytology becomes essential for accurate diagnosis.
Conclusion
In conclusion, differentiating benign from MBSs is a complex but essential task that significantly influences patient management and outcomes. A thorough understanding of the imaging features—such as stricture morphology, wall characteristics, presence of associated masses, and ancillary findings—is critical. While cross-sectional modalities like contrast-enhanced CT and MRI/MRCP form the backbone of noninvasive evaluation, integration of clinical history, laboratory markers, and, when necessary, tissue sampling remains indispensable. Radiologists play a central role in guiding the diagnostic pathway by recognizing subtle imaging clues, suggesting appropriate further investigations, and helping to avoid both overtreatment and delayed diagnosis.
Conflict of Interest
All the authors hereby declare that they have no conflicting interests (including but not limited to commercial, personal, political, intellectual, or religious interests).
Author Contributions
P.A.: Literature search and manuscript preparation and editing.
K.S.M.: Manuscript editing and contribution to figures.
Guarantor of the case: K.S.M.
Prior Presentation of Case
This case has not been presented at any professional meeting to the best of our knowledge.
-
References
- 1 Shanbhogue AKP, Tirumani SH, Prasad SR, Fasih N, McInnes M. Benign biliary strictures: a comprehensive review. AJR Am J Roentgenol 2011; 197 (02) W295-W306
- 2 Katabathina VS, Dasyam AK, Dasyam N, Hosseinzadeh K. Adult bile duct strictures: role of MR imaging and MR cholangiopancreatography in characterization. Radiographics 2014; 34 (03) 565-586
- 3 Fadahunsi OO, Ibitoye BO, Adisa AO, Alatise OI, Adetiloye VA, Idowu BM. Diagnostic accuracy of ultrasonography in adults with obstructive jaundice. J Ultrason 2020; 20 (81) e100-e105
- 4 Spârchez Z, Radu P. Role of contrast-enhanced US in biliary disease. Med Ultrason 2014; 16 (01) 41-47
- 5 Singh A, Gelrud A, Agarwal B. Biliary strictures: diagnostic considerations and approach. Gastroenterol Rep (Oxf) 2015; 3 (01) 22-31
- 6 Ma MX, Jayasekeran V, Chong AK. Benign biliary strictures: prevalence, impact, and management strategies. Clin Exp Gastroenterol 2019; 12: 83-92
- 7 Yadlapati S, Khashab MA. Clinical approach to indeterminate biliary strictures. World J Gastroenterol 2020; 26 (06) 634-646
- 8 Adler DG, Baron TH, Davila RE. et al. Approach to the patient with a biliary stricture. Gastrointest Endosc 2016; 83 (01) 22-30
- 9 Gallotti A, D'Onofrio M, Pozzi Mucelli R. Ultrasound elastography in biliary tract diseases. World J Gastroenterol 2014; 20 (22) 7231-7236
- 10 Claudon M, Dietrich CF, Choi BI. et al. Contrast-enhanced ultrasound for the characterization of focal liver lesions: a prospective multicenter clinical trial. Br J Radiol 2010; 83 (992) 743-753
- 11 Fontán FJ, Reboredo ÁR, Siso AR. Accuracy of contrast-enhanced ultrasound in the diagnosis of bile duct obstruction. Ultrasound Int Open 2015; 1 (01) E12-E18
- 12 Baron RL, Stanley RJ, Lee JK, Koehler RE, Balfe DM. CT of the bile ducts: evaluation of benign and malignant obstruction. AJR Am J Roentgenol 2004; 183 (05) 1327-1332
- 13 Franco PN, Spasiano CM, Maino C. et al. Principles and applications of dual-layer spectral CT in gastrointestinal imaging. Diagnostics (Basel) 2023; 13 (10) 1740
- 14 Liang H, Zhou Y, Zheng Q. et al. Dual-energy CT with virtual monoenergetic images and iodine maps improves tumor conspicuity in patients with pancreatic ductal adenocarcinoma. Insights Imaging 2022; 13 (01) 153
- 15 Chong S, Lee SS, Kim YJ. et al. Split-bolus multidetector CT of the liver: optimizing arterial and venous phase enhancement. AJR Am J Roentgenol 2008; 190 (06) 1548-1555
- 16 Nikhileswar K, Sharma S, Srivastava DN. et al. Comparison of split bolus dual energy CT and standard multiphase CT in assessing vascular invasion in patients with biliary malignancies: a randomized study. Abdom Radiol (NY) 2025; ( e-pub ahead of print).
- 17 Caoili EM, Paulson EK, Heyneman LE, Branch MS, Eubanks WS, Nelson RC. Helical CT cholangiography with three-dimensional volume rendering using an oral biliary contrast agent: feasibility of a novel technique. AJR Am J Roentgenol 2000; 174 (02) 487-492
- 18 Taenzer V, Volkhardt V. Double blind comparison of meglumine iotroxate (Biliscopin), meglumine iodoxamate (Endobil), and meglumine ioglycamate (Biligram). AJR Am J Roentgenol 1979; 132 (01) 55-58
- 19 Mortelé KJ. et al. Multimodality imaging of pancreatic and biliary congenital anomalies. AJR Am J Roentgenol 2013; 201 (04) W601-W609
- 20 Seale MK, Bakare G, Jha RC. et al. Hypervascular liver lesions: role of MRI. J Magn Reson Imaging 2010; 31 (05) 1259-1272
- 21 Fujita N, Noda Y, Kobayashi G. et al. Intraductal ultrasonography (IDUS) for the diagnosis of biliopancreatic diseases. Best Pract Res Clin Gastroenterol 2009; 23 (05) 729-742
- 22 Park DH, Lee SS, Lee SK. et al. Accuracy of intraductal ultrasonography for differentiation of malignant and benign bile duct strictures. Clin Gastroenterol Hepatol 2018; 16 (07) 975-982
- 23 Chang HY, Liu B, Wang YZ. et al. Percutaneous transhepatic cholangiography versus endoscopic retrograde cholangiography for the pathological diagnosis of suspected malignant bile duct strictures. Medicine (Baltimore) 2020; 99 (11) e19545
- 24 Kurdia KC, Irrinki S, Siddharth B, Gupta V, Lal A, Yadav TD. Percutaneous transhepatic cholangiography in the era of magnetic resonance cholangiopancreatography: a prospective comparative analysis in preoperative evaluation of benign biliary stricture. JGH Open 2021; 5 (07) 820-824
- 25 Young M, Collier SA. Percutaneous transhepatic cholangiography. [Updated 2025 Jul 21]. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2025. Jan-. Accessed January 19, 2025 at: https://www.ncbi.nlm.nih.gov/books/NBK493190/
- 26 Tabata T, Kamisawa T, Hara S. et al. Differentiating immunoglobulin g4-related sclerosing cholangitis from hilar cholangiocarcinoma. Gut Liver 2013; 7 (02) 234-238
- 27 Mohammad Alizadeh AH, Shahnazi A, Rasoulzadeh A. et al. Characteristic findings of primary sclerosing cholangitis on endoscopic retrograde cholangiography: which is the most common finding?. Clin Med Insights Gastroenterol 2011; 5: 1-4
Address for correspondence
Publication History
Article published online:
13 February 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Shanbhogue AKP, Tirumani SH, Prasad SR, Fasih N, McInnes M. Benign biliary strictures: a comprehensive review. AJR Am J Roentgenol 2011; 197 (02) W295-W306
- 2 Katabathina VS, Dasyam AK, Dasyam N, Hosseinzadeh K. Adult bile duct strictures: role of MR imaging and MR cholangiopancreatography in characterization. Radiographics 2014; 34 (03) 565-586
- 3 Fadahunsi OO, Ibitoye BO, Adisa AO, Alatise OI, Adetiloye VA, Idowu BM. Diagnostic accuracy of ultrasonography in adults with obstructive jaundice. J Ultrason 2020; 20 (81) e100-e105
- 4 Spârchez Z, Radu P. Role of contrast-enhanced US in biliary disease. Med Ultrason 2014; 16 (01) 41-47
- 5 Singh A, Gelrud A, Agarwal B. Biliary strictures: diagnostic considerations and approach. Gastroenterol Rep (Oxf) 2015; 3 (01) 22-31
- 6 Ma MX, Jayasekeran V, Chong AK. Benign biliary strictures: prevalence, impact, and management strategies. Clin Exp Gastroenterol 2019; 12: 83-92
- 7 Yadlapati S, Khashab MA. Clinical approach to indeterminate biliary strictures. World J Gastroenterol 2020; 26 (06) 634-646
- 8 Adler DG, Baron TH, Davila RE. et al. Approach to the patient with a biliary stricture. Gastrointest Endosc 2016; 83 (01) 22-30
- 9 Gallotti A, D'Onofrio M, Pozzi Mucelli R. Ultrasound elastography in biliary tract diseases. World J Gastroenterol 2014; 20 (22) 7231-7236
- 10 Claudon M, Dietrich CF, Choi BI. et al. Contrast-enhanced ultrasound for the characterization of focal liver lesions: a prospective multicenter clinical trial. Br J Radiol 2010; 83 (992) 743-753
- 11 Fontán FJ, Reboredo ÁR, Siso AR. Accuracy of contrast-enhanced ultrasound in the diagnosis of bile duct obstruction. Ultrasound Int Open 2015; 1 (01) E12-E18
- 12 Baron RL, Stanley RJ, Lee JK, Koehler RE, Balfe DM. CT of the bile ducts: evaluation of benign and malignant obstruction. AJR Am J Roentgenol 2004; 183 (05) 1327-1332
- 13 Franco PN, Spasiano CM, Maino C. et al. Principles and applications of dual-layer spectral CT in gastrointestinal imaging. Diagnostics (Basel) 2023; 13 (10) 1740
- 14 Liang H, Zhou Y, Zheng Q. et al. Dual-energy CT with virtual monoenergetic images and iodine maps improves tumor conspicuity in patients with pancreatic ductal adenocarcinoma. Insights Imaging 2022; 13 (01) 153
- 15 Chong S, Lee SS, Kim YJ. et al. Split-bolus multidetector CT of the liver: optimizing arterial and venous phase enhancement. AJR Am J Roentgenol 2008; 190 (06) 1548-1555
- 16 Nikhileswar K, Sharma S, Srivastava DN. et al. Comparison of split bolus dual energy CT and standard multiphase CT in assessing vascular invasion in patients with biliary malignancies: a randomized study. Abdom Radiol (NY) 2025; ( e-pub ahead of print).
- 17 Caoili EM, Paulson EK, Heyneman LE, Branch MS, Eubanks WS, Nelson RC. Helical CT cholangiography with three-dimensional volume rendering using an oral biliary contrast agent: feasibility of a novel technique. AJR Am J Roentgenol 2000; 174 (02) 487-492
- 18 Taenzer V, Volkhardt V. Double blind comparison of meglumine iotroxate (Biliscopin), meglumine iodoxamate (Endobil), and meglumine ioglycamate (Biligram). AJR Am J Roentgenol 1979; 132 (01) 55-58
- 19 Mortelé KJ. et al. Multimodality imaging of pancreatic and biliary congenital anomalies. AJR Am J Roentgenol 2013; 201 (04) W601-W609
- 20 Seale MK, Bakare G, Jha RC. et al. Hypervascular liver lesions: role of MRI. J Magn Reson Imaging 2010; 31 (05) 1259-1272
- 21 Fujita N, Noda Y, Kobayashi G. et al. Intraductal ultrasonography (IDUS) for the diagnosis of biliopancreatic diseases. Best Pract Res Clin Gastroenterol 2009; 23 (05) 729-742
- 22 Park DH, Lee SS, Lee SK. et al. Accuracy of intraductal ultrasonography for differentiation of malignant and benign bile duct strictures. Clin Gastroenterol Hepatol 2018; 16 (07) 975-982
- 23 Chang HY, Liu B, Wang YZ. et al. Percutaneous transhepatic cholangiography versus endoscopic retrograde cholangiography for the pathological diagnosis of suspected malignant bile duct strictures. Medicine (Baltimore) 2020; 99 (11) e19545
- 24 Kurdia KC, Irrinki S, Siddharth B, Gupta V, Lal A, Yadav TD. Percutaneous transhepatic cholangiography in the era of magnetic resonance cholangiopancreatography: a prospective comparative analysis in preoperative evaluation of benign biliary stricture. JGH Open 2021; 5 (07) 820-824
- 25 Young M, Collier SA. Percutaneous transhepatic cholangiography. [Updated 2025 Jul 21]. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2025. Jan-. Accessed January 19, 2025 at: https://www.ncbi.nlm.nih.gov/books/NBK493190/
- 26 Tabata T, Kamisawa T, Hara S. et al. Differentiating immunoglobulin g4-related sclerosing cholangitis from hilar cholangiocarcinoma. Gut Liver 2013; 7 (02) 234-238
- 27 Mohammad Alizadeh AH, Shahnazi A, Rasoulzadeh A. et al. Characteristic findings of primary sclerosing cholangitis on endoscopic retrograde cholangiography: which is the most common finding?. Clin Med Insights Gastroenterol 2011; 5: 1-4